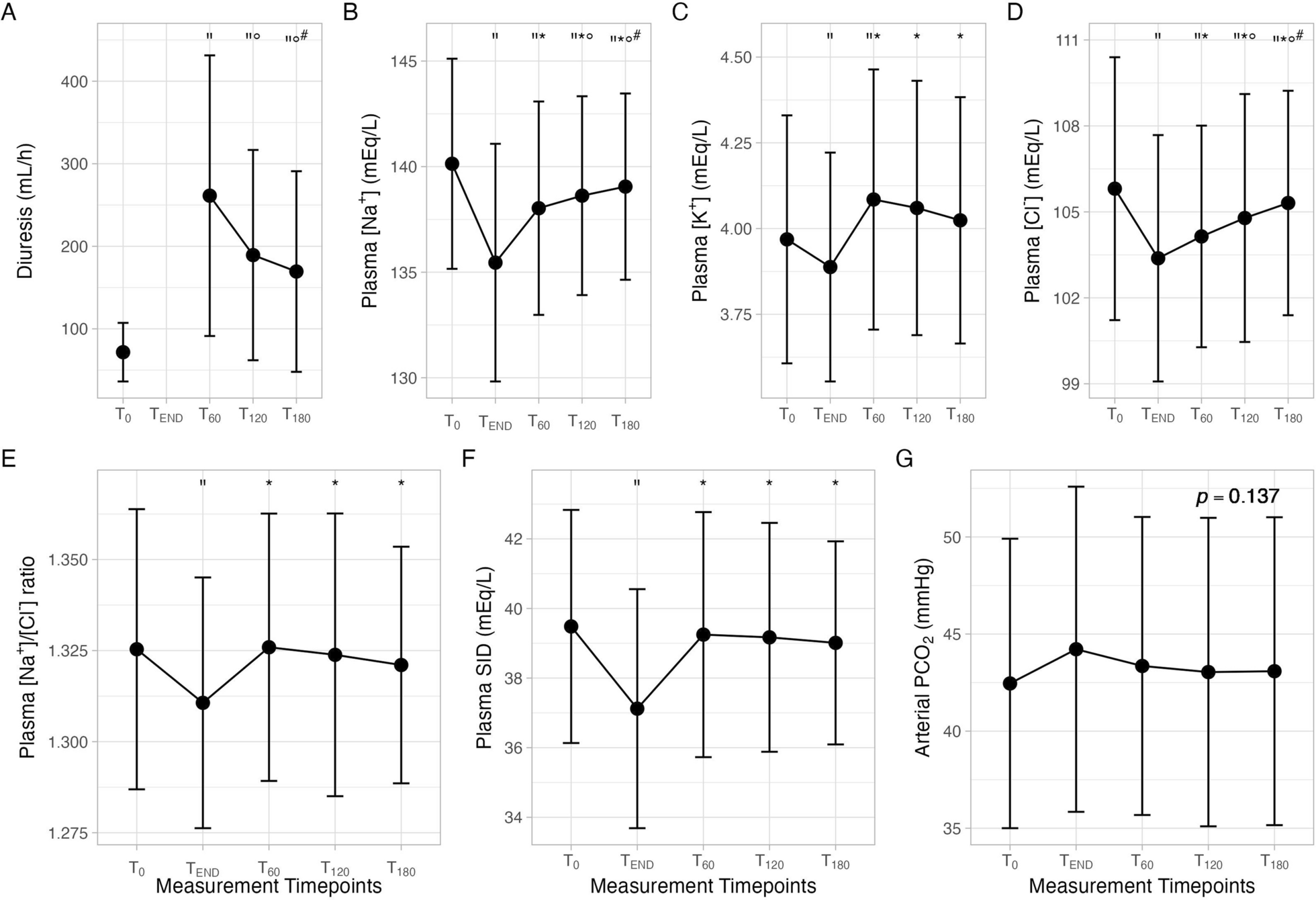
The present study showed the plasma and urinary physiochemical effects of an intravenous administration of mannitol in mechanically ventilated patients: (1) diuresis increased significantly immediately after the end of the infusion, then decreased up to 180 min; (2) haemoglobin, plasma sodium and chloride concentrations decreased significantly after the end of the infusion, then significantly increased; (3) arterial pH as well as plasma SID decreased significantly at the end of the infusion resulting in dilutional acidosis; and (4) urinary SID and urinary ammonium concentration initially decreased, then after 60 min both increased significantly.
The most commonly used diuretics for critically ill patients are loop diuretics (e.g., furosemide) and osmotic diuretics (e.g., mannitol). Despite their different clinical, pharmacological and pharmacokinetic characteristics, they significantly improve diuresis [17, 18].
In addition, both can significantly affect the composition of plasma and urine, leading to different alterations in acid–base equilibrium [11,12,13,14, 19]. According to the Stewart approach, an intravenous infusion of 40 mg of furosemide was found to significantly decrease the plasma chloride concentration and increase the plasma SID in critically ill patients. It was also found to increase urinary losses of all electrolytes and reduce urinary SID [20].
Mannitol was first used in 1945 to improve renal function in dogs following a period of ischaemia [21]. It is currently commonly administered in several clinical settings, including cases of drug intoxications, refractory oedema, oliguric renal failure and cerebral oedema. It is also used to prevent acute renal failure in patients with rhabdomyolysis or following the use of radiocontrast agents [2, 7, 17, 18, 22, 23]. Possible side effects include volume depletion due to its strong osmotic diuretic effect, as well as hypernatremia and metabolic acidosis, particularly with cumulative dosages and in cases of acute or chronic kidney failure [23,24,25,26]. Despite its common use in daily clinical practice, there is a paucity of studies that have described the physiological effects of mannitol in critically ill patients [17].
In the present study, the whole acid–base equilibrium of all patients was evaluated by simultaneously assessing plasma and urinary SID using an arterial blood gas analysis and analyzing urine composition by the K.IN.G analyzer [27].
The mannitol infusion immediately after 30 min provided a significant increase in diuresis compared to baseline, which remained significantly higher up to 180 min, yet significantly reduced compared to T30. A previous study reported that, for a similar dosage of mannitol administered to healthy subjects, urine flow increased from 78 ± 29 to 287 ± 21 mL/h at 90 min, with peak serum concentration occurring after 15 min [28].
At the end of mannitol infusion, plasma electrolyte concentrations decreased due to a dilutional effect, resulting in a reduction in SID. The same degree of dilution should be expected for Atot (mainly albumin and phosphate), with an alkalising influence that should partially compensate for the acidifying influence of the SID reduction. However, albumin levels remained constant, as well as arterial carbon dioxide levels, due to an unchanged ventilation throughout the study. Therefore, the predominant effect was the dilution of the SID, resulting in a dilutional metabolic acidosis [29,30,31].
Subsequently, at T60 the dilutional effect ended, in fact plasma electrolyte concentrations, pH and SID exhibited higher levels up to 180 min.
Similarly, the addition of mannitol to a priming solution for cardiopulmonary bypass resulted in an increase in diuresis and a decrease in serum sodium concentration (138 ± 28 to 133 ± 2.6 mEq/L) [32]. The duration of blood volume increase depends on the equilibrium rate of mannitol in the extracellular compartments and the renal excretion rate due to the osmotic diuresis.
At the urinary level the excretion of sodium and chloride did not change throughout the study, while ammonium concentration decreased significantly 30 min after the end of the infusion compared to TEND, causing a decrease in urinary SID. Then, 90 min after the end of the infusion, both urine ammonium concentration and urinary SID increased significantly and remained higher up to 180 min compared to T30. This increase in the SID could be interpreted as a compensatory mechanism exerted by the kidneys to counterbalance metabolic dilutional acidosis, or it could simply reflect only an initial increase in urine flow, followed by a subsequent reduction [11]. In fact, urinary ammonium concentration depends on how much ammonium the kidney produces (in response to acidosis) and on how diluted or concentrated the urine is. In our study, even though ammonium concentration significantly decreased and then increased, the absolute amount of ammonium excreted remained clinically unchanged at the different timepoints.
Moreover, both the plasmatic Na⁺/Cl⁻ and urinary Na/Cl ratios remained constant, meaning that the dilutional effect in plasma was prevalent, the kidney relative excretion pattern was unchanged, and any differences in ammonium excretion were just due to urine dilution or concentration.
To evaluate the possible influence of intravascular volume on the response to mannitol administration, the population was divided into two groups based on higher or lower urine output. The effects of mannitol infusion were found to be similar in both groups. The increase in free water clearance was independent from the baseline urine flow rate.



Comments (0)