In the present study, we demonstrated that TLV with the LV4B prototype is feasible in a swine model of severe ARDS leading to high mortality in control conditions. This prototype was designed to monitor and control pulmonary liquid volumes during a short course of TLV. After one hour of follow-up, TLV was well tolerated in terms of hemodynamic and systemic responses in animals with severe ARDS. TLV also tended to prevent the appearance of severe hypoxemia and subsequent mortality from hemodynamic collapse, while also reducing lung lesions at histology.
Importantly, we used an oleic acid model of ARDS, which causes alveolar membrane damage and “reproduce most of the pathophysiology of clinical [..] ARDS” [12]. This model reliably produces lung injury with rapid and severe hypoxemia, pulmonary hypertension, and respiratory compliance decrease [12]. It is considered particularly relevant to study severe ARDS complicated by acute heart failure or pulmonary hypertension, while less suitable for studying the inflammatory pathophysiology of ARDS, as compared to other models.
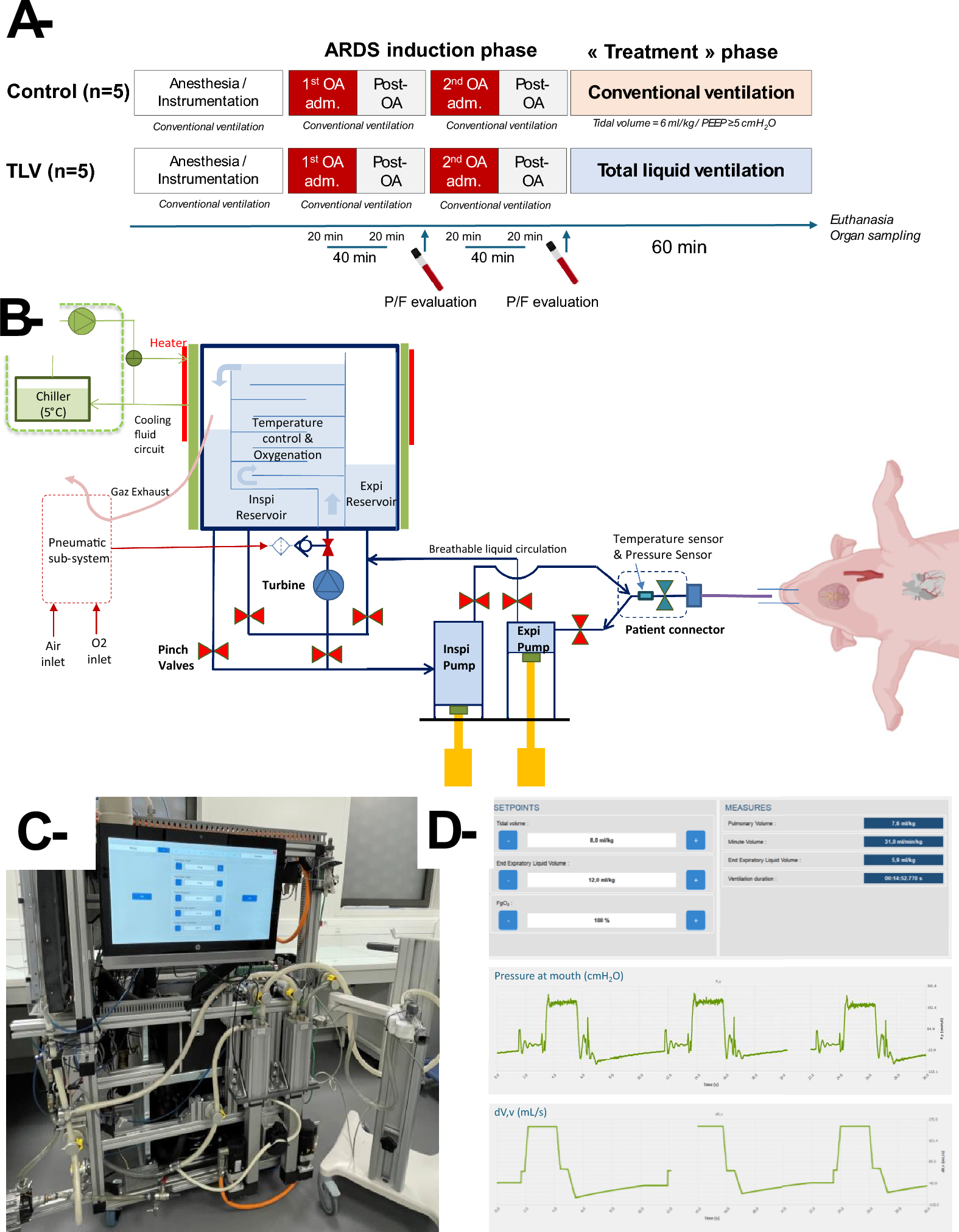
In previous studies, the benefits of TLV have been documented in different ARDS models including meconial aspiration in lambs [13], post-cardiac arrest lung injury in piglets [14] and oleic acid in sheep [8, 9]. In the latter large animal studies, TLV was maintained during 4 [9] and 24 h [8], respectively, demonstrating the feasibility of a prolonged period of TLV. In the present study, animals were evaluated during only one hour after the initial injury since our goal was to evaluate the performance of a new generation of liquid ventilator capable of controlling EELqV and optimizing expiratory flow through a dedicated algorithm designed to prevent airway collapse. Airway collapse management is one of the biggest challenges during TLV due to active expiration [11, 15]. Failure to do so impairs proper ventilation and/or necessitates increasing lung filling with a risk of subsequent lung trauma.
Importantly, EELqV level appeared relatively low with the LV4B prototype as compared to the initial lung filling observed in previous TLV studies [8, 9]. For instance, the lung was initially filled with 30 mL/kg of breathable liquid in the long-term TLV study in sheep [8]. This level corresponds to the upper range observed in our study and was only reached in 2/5 animals. In addition, this level was only progressively achieved in the present study, whereas previous studies [8, 9] started at this level with a manual infusion into the endotracheal tube before connection to the TLV prototype. In comparison, LV4B performed a reproducible, programmed lung filling to facilitate TLV implementation in clinical conditions. This filling phase is known to be at risk since gas elimination should be concomitant with the progressive liquid administration to prevent lung trauma [3, 5]. If not properly managed, overdistention of the lung might occur. Therefore, LV4B’s ability to fill the lung with real-time monitoring of pulmonary liquid volume brings a significant advancement.
In a previous study in piglets with intact lungs, we have already shown that EELqV should be maintained at low or moderate levels, below functional residual capacity, during short episodes of liquid ventilation [16]. In the middle of a 30 min of TLV, air was indeed still observed in the upper pulmonary territory in this study [16]. Given these findings, the actual lung volume refers to the total volume consisting of both trapped air and actual EELqV. Accordingly, EELqV likely needs to be gradually increased over the first 30 min of the TLV to compensate for the slow elimination of gases, aiming to achieve an optimal filling and avoid the occurrence of airway collapse at end-expiration. The critical pressure promoting airway pressure indeed depends upon the lung filling level of the recruited region [5]. As already described, TLV was performed for 60 min in the present study, during which the EELqV had to be gradually increased over the course of TLV. We speculate that this phenomenon is inevitable in response to the progressive removal of trapped gas during the TLV. Even though we had to increase the EELqV up to 30 mL/kg in some animals, it remained lower than the level reported in former studies. In addition, when examining the difference between the 20% and 50% reduction in expiratory flow for collapse prevention, the 50% reduction showed higher minute ventilation (> 60 mL/kg/min) and lower levels of EELqV (< 20 mL/kg), demonstrating a better resolution of collapse occurrence and confirming the possibility of lowest EELqV. In addition, the stability of the EELqV after 30 min of TLV suggests that the lung was recruited and that air was mostly eliminated. In a previous study in piglets submitted to 180 min of TLV, lungs were indeed fully filled after 60 min with no more trapped air in the upper area evaluated by CT scan [17]. In any case, the relevance of maintaining EELqV at the lowest possible level has been well shown during partial liquid ventilation in rats [18], in which the risk due to air trapping was well evidenced [19].
Notably, despite the short duration of the follow-up, we were able to evidence improved oxygenation in surviving animals of the TLV group, as well as reduced inflammatory and congestive lesions at histology. These effects may be partially attributed to the lung lavage properties of TLV, which washed exudates and hemorrhagic debris from the injured lungs. In previous studies, TLV was even proposed for proper lung lavage in specific conditions such as meconial aspiration [13]. The anti-inflammatory and lung-protective effects of TLV can also be related to increased alveolar recruitment and reduced transpulmonary pressure, strains, and ventilation/perfusion mismatch as compared to gas ventilation [3, 4]. Several studies also suggested a direct anti-inflammatory effect of organofluorine due to the suppression of the air–liquid interface in the alveoli [7, 14]. This is not directly supported by the evaluation of the cytokine levels within the injured lungs in our study, as they were significantly increased in TLV versus control animals, which is inconsistent with the histology data. This discrepancy may be partly due to the shorter follow-up in control animals, which died prematurely from refractory hypoxemia and hemodynamic collapse. This could provoke immunoparalysis and altered immune cell reactivity despite increased recruitment in the pulmonary vascular walls and alveoli. Interestingly, a similar increase in pulmonary cytokine levels was observed in a lamb model of extreme prematurity [20]. This phenomenon could be explained by the fact that organofluorine compounds are cleared by phagocytic cells, leading to cytokine secretion [4, 21]. Supporting this hypothesis, safety studies involving the intravenous administration of PFOB demonstrated increased cytokine blood levels, along with mild, reversible flu-like symptoms, with no further consequence on the longer term [22]. Therefore, this could be a normal consequence of breathable liquid elimination but obviously deserves further investigations in the longer term.
Despite the positive findings observed in the present study, several limitations have to be acknowledged, among which the most important ones are the limited number of animals and the short duration of follow-up. In fact, the limited number of animals might have been too small to achieve adequate statistical power to show significant differences for several parameters, especially considering the premature death of several animals in the Control groups. The necessity to confirm results after prolonged duration has already been discussed, even if the primary goal was here to evaluate the feasibility of TLV with LV4B in very severe conditions. The latter point could also be considered as a limitation since short-term mortality was very high in Control conditions, with major and acute pulmonary hypertension and systemic repercussions. It could be important to evaluate findings in different conditions, e.g., milder ARDS or severe ARDS in combination with ECMO. Indeed, it would allow to determine whether TLV should be considered as an alternative or a bridge to ECMO. Finally, one would argue that we did not fully optimize the protective ventilation in the Control group, which would also require further analysis. For example, PEEP was fixed at 5 mmH2O in the Control group and no additional rescue maneuvers were allowed, such as airway suctioning, prone positioning, or recruitment maneuvers. A part of TLV potential benefits could clearly be related to debris removal. In addition, respiratory mechanics remain hard to evaluate during TLV for a proper comparison with the Control conditions. Indeed, airway pressure during TLV differs from gas ventilation, under which this depends mostly on respiratory compliance and resistance. During TLV, inertance must be considered due to the high density and acceleration of the liquid filling of airways and endotracheal tube. Consequently, a direct correspondence between pressures (static or dynamic) measured at the mouth cannot directly be performed during TLV, deserving further investigations.



Comments (0)