General characteristics of the study
This prospective observational study was conducted under the approval of the Charité ethics committee (Ethikkommission der Charité Universitätsmedizin Berlin) under application numbers EA1/193/16, EA1/291/16, and EA1/018/17. The study recruited 95 patients between December 2016 and May 2018 at the Department of Surgery, Campus Virchow Klinikum (Charité—Universitätsmedizin Berlin). Inclusion criteria for the liver resection cohort were: age 18 years or older, not currently pregnant, indication for liver resection, written informed consent, and the ability to provide information and consent. In total, 25 patients suffered from HCC. The control group comprised 24 patients who underwent surgery, mostly abdominal hernia operations (supplement table I), respectively. The inclusion criteria for control patients were; absence of liver disease, no ongoing immunosuppressive therapy, no chronic infectious and no history of malignant tumors. Participants who did not fulfil these criteria were excluded from the study.
Isolation and cryopreservation of peripheral blood mononuclear cells
PBMCs were obtained from HCC patients and control patients. Venous blood was collected aseptically before and several days after surgery, with 3 ml collected in an EDTA tube and 4 ml collected in a heparinized tube. The blood samples were subsequently processed for the preservation of plasma. The tubes were spun at 2500 g and 4 °C for 15 min. Subsequently, the blood plasma was transferred to fresh tubes, cryopreserved in liquid nitrogen, and ultimately kept at − 80 °C.
To isolate PBMCs, the absent blood plasma in the EDTA tube was substituted with 2 ml of FACS buffer [PBS (500 ml) + 1% BSA (5 g) + NaN₃ (0.5 g)], filtered with a 0.2 μm filter prior to usage. The EDTA blood sample was mixed with 40 ml of lysis buffer, comprising 80.2 g/l NH₄Cl (1.5 mol/l), 8.4 g/l NaHCO₃ (0.10 mol/l), and 372.2 mg/l EDTA dissolved in 800 ml sterile distilled H2O adjusted to pH 7.4 after filtering through a 0.2 µm filter. Following a lysis time of several minutes, the erythrocytes underwent lysis and the liquid became clear. Subsequently, the lysed cells were centrifuged at 400g and 4 °C for 5 min, and the supernatant was discarded. This process was repeated using 10 ml of lysis buffer. Remaining blood cells were temporarily stored on ice, and lysis was stopped by adding 2 ml of PBS (pH 7.4 phosphate-buffered saline solution containing 8.0 g NaCl, 0.2 g KCl, 1.42 g Na₂HPO₄, and 0.27 g KH₂PO₄ per liter). Finally, isolated PBMCs were placed in cryopreservation vials, each containing approximately 10,000,000 cells with 100 μl of DMSO and 900 μl of FBS serum (fetal bovine serum). The cryopreservation vials were kept in a refrigerated container (Thermo Scientific™ Mr. Frosty™) at − 80 °C for 24 h prior to being transferred for long-term storage at − 156 °C.
Thawing of peripheral blood mononuclear cells
To defrost the cryopreserved PBMCs, first 1 ml of CTL Anti-Aggregate Wash Medium™ for each sample in a 37 °C water bath was thawed. Then, it was mixed with 19 ml of T-cell medium (RPMI 1640, supplemented with 5 ml of l-alanine/l-glutamine, 4 µl of β-Mercaptoethanol, 5 ml of Penicillin/Streptomycin (100 U/ml), and 50 ml of FBS). The solution was divided into two Falcon tubes, with 10 ml in each and incubated in a water bath for 20 min to regulate the pH and temperature. The cryopreserved samples were held in a water bath of 37 °C for 1 min to partially thaw them while keeping a frozen portion intact. Following this, the nearly thawed PBMC were carefully mixed with 1 ml of CTL Anti-Aggregate Wash Medium and slowly transferred dropwise into the remaining solution of CTL and RMPI medium in a Falcon tube. The cell suspension was centrifuged at 400g for 10 min at room temperature. The supernatant was subsequently removed, and the remaining 10 ml of solution were subjected to the same process. The supernatant was then removed, and the remaining 10 ml of solution were subjected to the same process. Thereafter, cell counting was performed. The supernatant was removed once again, and the PBMCs were suspended in 300 μl of EasySepCell™ Medium, which is a mixture of Dulbecco's PBS, FBS (2%), and EDTA (1 mM) in PBS from STEMCELL Technologies. The supernatant was then removed, and the remaining 10 ml of solution were subjected to the same process.
Isolation and cultivation of T cells
For the purpose of T cell isolation, the EasySep™ Human T Cell Isolation Kit [(Catalog #17951) STEMCELL Technologies GmbH, Cologne, Germany] was utilized. This kit employs antibody complexes conjugated with magnetic particles to effectively isolate unwanted cells. Initially, 250 μl of thawed cells were mixed with 12 μl of an isolation cocktail, and the solution was incubated in FACS tubes for 5 min at room temperature. Following this step, 10 μl of RapidSpheres were added, and the whole suspension was filled up to a total volume of 2.5 ml with EasySep™ Medium. Next, the FACS tubes were placed in the EasySep™ magnet [(Catalog #18000] STEMCELL Technologies GmbH, Cologne, Germany) for three minutes to isolate T cells.
Eventually, isolated T cells were then carefully transferred to a new FACS tube, and a maximum of 1,000,000 isolated T cells, but at least 500,000, were transferred to a 96-well standard microtiter plate. The cells were stained using anti-CD28 and protein transport inhibitor (0.2 μl in 100 μl PBS). The plate was incubated with T cell medium replenished to 100 μl for four hours at 37 °C.
Antibody staining
After four hours of incubation, the T cells that were isolated underwent washing with 100 μl of PBS and were centrifuged at room temperature for 5 min with 400 g. The supernatant was removed meticulously, and cells were stained with extracellular stains (50 μl each of 5 μl of PBS, 5 μl of FC block, 1 μl of CD203a, 1 μl of CCR6, 1 μl of CCR4, and 0.1 μl of Zombie UV) for 15 min in a dark at room temperature. Following, the cells were centrifuged with 100 μl of FACS buffer for 5 min at 400g and room temperature. The supernatant was subsequently removed before the cells were treated with 100 μl of fixation buffer for 20 min.
Afterward, intracellular staining was performed using 48 μl of Perm Wash, 1 μl each of IL-17 and IL-22, with the cells again being centrifuged with 100 μl of Perm Wash and stained with appropriate antibodies for 15 min. The cells were washed with 100 μl of FACS buffer, centrifuged, and then replenished with 200 μl of FACS buffer. The cells were finally transported on ice for flow cytometric measurement using the Hoechst UV filter and BD LSRFortessa™ X-20, with the FACSDiva software BD FACSDiva™ v9.0 (BD Biosciences, San Jose, USA). A number of events adapted to the patient sample were measured in each case. To adjust for overlapping emission spectra during multiple staining events, we utilized the FACSDiva software to calculate the compensation matrix. To establish compensation, we conducted a single staining on all antibodies in patient samples from the group who had undergone liver resection.
eNAD⁺ measurement in plasma
eNAD+ levels were measured in all 95 patients of the liver resection group and in 24 control patients pre- and postoperatively. To determine NAD⁺ levels, a dichotomous pH extraction procedure incorporating heat was employed as previously described (Brunnbauer et al. 2018).
Frozen heparin plasma was thawed gradually at ambient temperature, then partitioned into two equal portions—one for NAD⁺ extraction and the other mixed with 270 μl of an albumin adjusted revised simulated body fluid (r-SBFA) for NADH extraction. The r-SBF solution was prepared by adjusting the pH to 7.4 in 1000 ml of DEPC water. The ingredients used were sodium chloride (5.403 g), sodium hydrogen carbonate (0.740 g), sodium carbonate (2.046 g), potassium chloride (0.225 g), potassium dihydrogen phosphate (0.138 g), magnesium chloride hexahydrate (0.311 g), 2-(4-(2-hydroxyethyl)−1-piperazinyl)ethanesulfonic acid (HEPES) (11.928 g), calcium chloride dihydrate (0.388 g), sodium sulfate (0.072 g) and bovine serum albumin (40 g).
To extract the samples, acid and base solutions were used as follows: 300 μl of 0.3 N HCl for eNAD+, 300 μl of 0.3 N KOH for NADH, and 300 μl of 0.3 N HCl for r-SBFA. The tubes were then incubated at 60 °C for 10 min, followed by equilibration on ice for 10 min. After 300 μl of neutralization buffer was added and centrifugation was performed at 16,000g for 10 min at 4 °C, a transparent 96-well standard microtiter plate was used for sample measurement. For the measurement of eNAD⁺, 50 μl of each sample were utilized, whereas for the measurement of NADH, 5 μl of each sample and 45 μl of a control sample (300 μl of r-SBF in 1:10 dilution) were utilized. Then, 150 μl of the master mix [TEA buffer: 1:10 diluted and adjusted to a pH of 7.4, alcohol dehydrogenase (ADH): 1:10 diluted, polymethylsiloxane polyhydrate (PMS): 10 mg/ml solution, 3-(4,5-dimethylthiazol-2-yl)−2,5-diphenyltetrazolium bromide (MTT)] was mixed with the samples. A solution of 1 mg/ml diluted in 100% ethanol (EtOH) was resuspended twice following timed conditions. After leaving it to stand for 5 min at room temperature in darkness, the microplate was analysed using a microplate reader (Infinite 200 PRO, Tecan Trading AG, Switzerland) at a temperature of 25 °C to determine the absorbance at 565 nm for 30 min.
Statistics
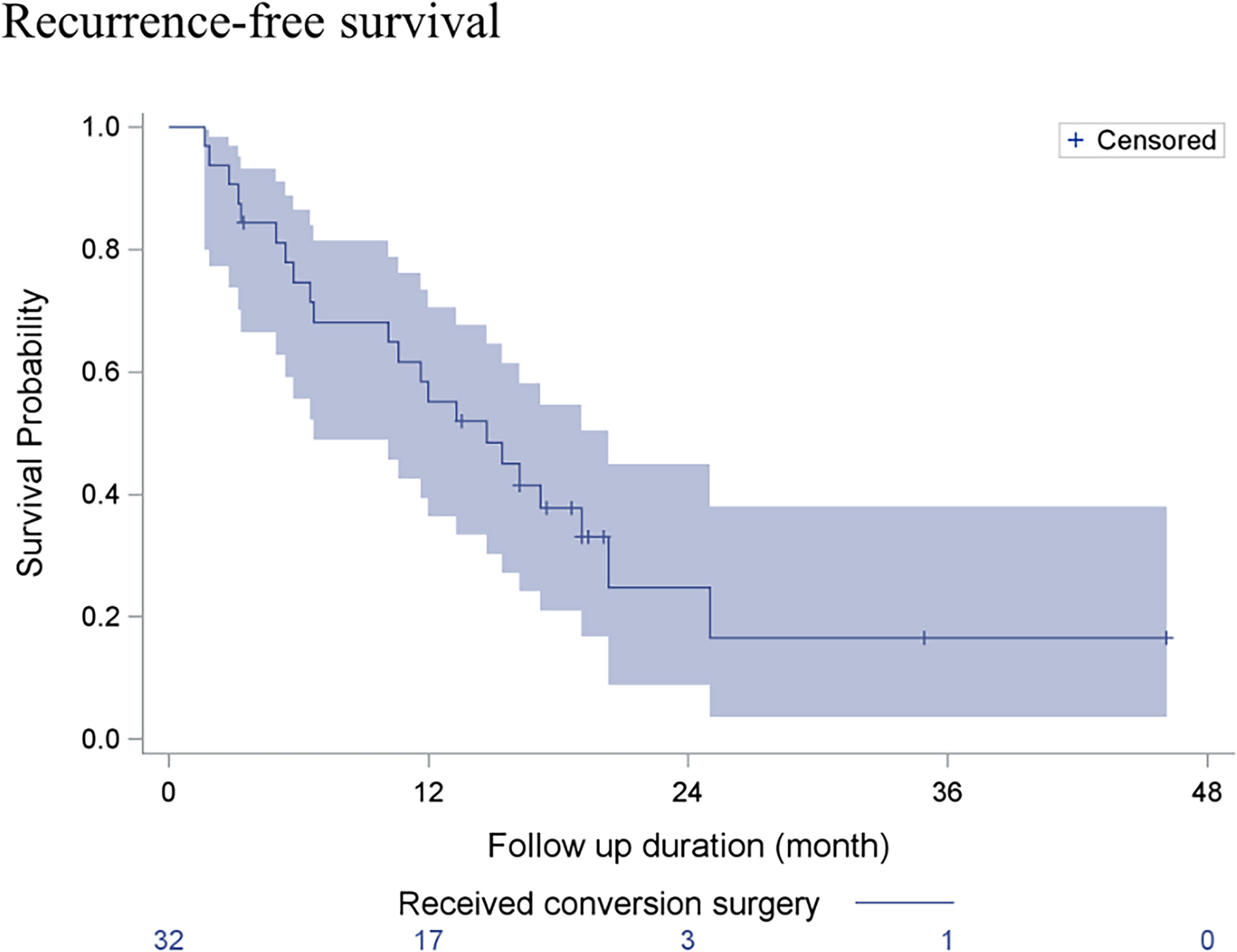
The statistical analysis was conducted using GraphPad Prism (GraphPad Software, Version 6.01, San Diego, USA). Patient demographics and clinical data were summarized using mean values and standard deviations. Unpaired t-tests were used for continuous variables, and chi-square tests were used for categorical variables. To assess the respective datasets for normality and warrant the use of unpaired t-tests, the D'Agostino–Pearson Omnibus Test was employed. Differences between liver resection patients and controls were evaluated using one-way ANOVA for normally distributed variables. The study compared the preoperative proportions of various subtypes of Th17 cells expressing CD203a in patients with HCC and healthy individuals using unpaired t-tests. Receiver operating characteristic (ROC) curves were used to evaluate diagnostic and prognostic biomarkers, with the area under the curve (ROC-AUC) measuring their diagnostic accuracy. To determine the optimal threshold for the potential biomarkers, the Youden index was derived. Recurrence-free and overall survival probabilities were calculated through implementation of the Logrank (Mantel–Cox) and Gehan-Breslow-Wilcoxon tests and conducted specifically in the HCC subgroup. Additionally, the Hazard Ratio (Mantel–Haenszel and Logrank) was computed. Statistical significance was determined using an alpha value of p < 0.05.

Comments (0)