
Remember me
Utilizing the TriNetX Research Network, 1698 stage IV lung cancer patients with NSCLC histology were identified who had received one of the indicated ICIs (nivolumab, pembrolizumab, atezolizumab, durvalumab, or avelumab) after diagnosis of bone metastases. These patients were divided into those who also received RT up to 3 months after their bone metastasis diagnosis (Cohort 1: RT + IO, n = 991) and those who received IO only (Cohort 2: IO only, n = 707). Among the 991 patients who received RT, 55% received radiation before starting immunotherapy, 38% received it after, and 7% received both within a 1-day window. Baseline statistics were compared between cohorts for general demographic variables, select comorbidities, sites of additional metastasis, chemotherapy and bone-targeting therapeutic agents, and select laboratory values. After 1:1 propensity score matching, each group included 623 patients. Matching substantially improved balance across covariates, with most standardized mean differences (SMDs) falling below 0.1.
Before matching, the RT + IO group was slightly younger (mean age at index: 64.5 vs. 66.9 years, SMD = 0.23), but age was balanced after matching (66.1 vs. 66.5 years, SMD = 0.003). The proportion of female patients was 37% vs. 41% before matching and balanced at 40% of each group after matching. Race and ethnicity distributions were comparable post-matching. Comorbidities, including coronary artery disease, diabetes, hypertension, and hypothyroidism, were evenly distributed. All patients had bone metastases by definition, and rates of other metastatic sites (including brain, liver, adrenal, and lung) were similar after matching. Imbalances in liver (SMD = 0.14) and adrenal (SMD = 0.11) metastases seen before matching were reduced (SMDs = 0.03 and 0.01, respectively). Chemotherapy was similar between groups post-matching, with carboplatin, cisplatin, paclitaxel, and pemetrexed use showing minimal differences. Roughly one-quarter of each group had received first-line chemotherapy (24%), and small differences in agents like carboplatin, paclitaxel, and pemetrexed were reduced with matching. Bone-targeting agent use (zoledronic acid and denosumab) remained low in both cohorts. Laboratory values including BMI, albumin, calcium, phosphate, LDH, and hemoglobin were well balanced. The proportion of patients with albumin < 3.5 g/dL was 30% vs. 38% before matching and equal at 36% in both groups after matching. Overall, the two treatment groups were well balanced across demographic, clinical, and biochemical variables following propensity-score matching.
Measures of associationThe measures of association included 3-month, 6-month, and 1-year mortality outcomes for all stage IV NSCLC histologies combined, as well as for the individual subsets of AC-NOS and SCC-NOS (Table 2). Additional subtypes were not analyzed separately due to insufficient sample size, so patients in the cohort who had NSCLC histologies other than AC-NOS or SCC-NOS were not included in a subset analysis. RT was associated with significantly improved outcomes in the overall cohort at both 3 months (risk difference [RD] = − 6.1%, 95% CI − 9.5%, − 2.6%, p = 0.001) and 6 months (RD = − 6.9%, 95% CI − 12%, − 2.2%, p = 0.004). At 1 year, the difference was not statistically significant (RD = − 4.4%, 95% CI − 9.9%, 1.0%, p = 0.108).
In the AC-NOS subset, which included 353 patients per group after matching, RT was associated with a significant reduction in 3-month mortality (RD = − 4.0%, 95% CI − 7.9%, − 0.05%, p = 0.046). No significant difference was observed at 6 months (RD = -2.3%, 95% CI − 6.8%, 2.2%, p = 0.129) or 1 year (RD = − 0.66%, 95% CI − 7.6%, 6.3%, p = 0.418). For the SCC-NOS subset, which included 99 patients per group after matching, outcomes at 3 months (RD = − 8.6%, 95% CI − 16%, − 0.34%, p = 0.040) favored the RT + IO group and reached statistical significance. However, differences at 6 months (RD = − 6.0%, 95% CI − 17%, 5.0%, p = 0.266) and 1 year (RD = − 0.9%, 95% CI − 14%, 12%, p = 0.764) were not statistically significant. These results may be limited by the smaller sample sizes in this subgroup.
As a sensitivity analysis, the same comparisons were repeated without propensity score matching and are presented in Supplemental Table 5. These results were consistent with the primary analysis. In the unmatched analysis, RT was again associated with significantly lower mortality for the overall cohort at 3 months (RD = − 7.8%, 95% CI − 11%, − 4.8%, p < 0.001), 6 months (RD = − 8.5%, 95% CI − 13%, − 4.0%, p < 0.001), and 1 year (RD = − 4.6%, 95% CI − 9.4%, 0.13%, p = 0.056). In the AC-NOS subset, RT was associated with significantly improved 3-month (RD = − 6.9%, 95% CI − 11%, − 3.1%, p < 0.001) and 6-month (RD = − 6.3%, 95% CI − 11%, − 1.3%, p = 0.013) mortality, with no difference observed at 1 year (RD = − 2.3%, 95% CI − 8.3%, 3.7%, p = 0.446). In the SCC-NOS subset, RT was associated with a statistically significant reduction in 3-month mortality (RD = − 8.2%, 95% CI − 16%, − 0.68%, p = 0.028), while results at 6 months (RD = − 9.9%, p = 0.064) and 1 year (RD = − 7.9%, p = 0.198) again favored RT, but did not reach significance.
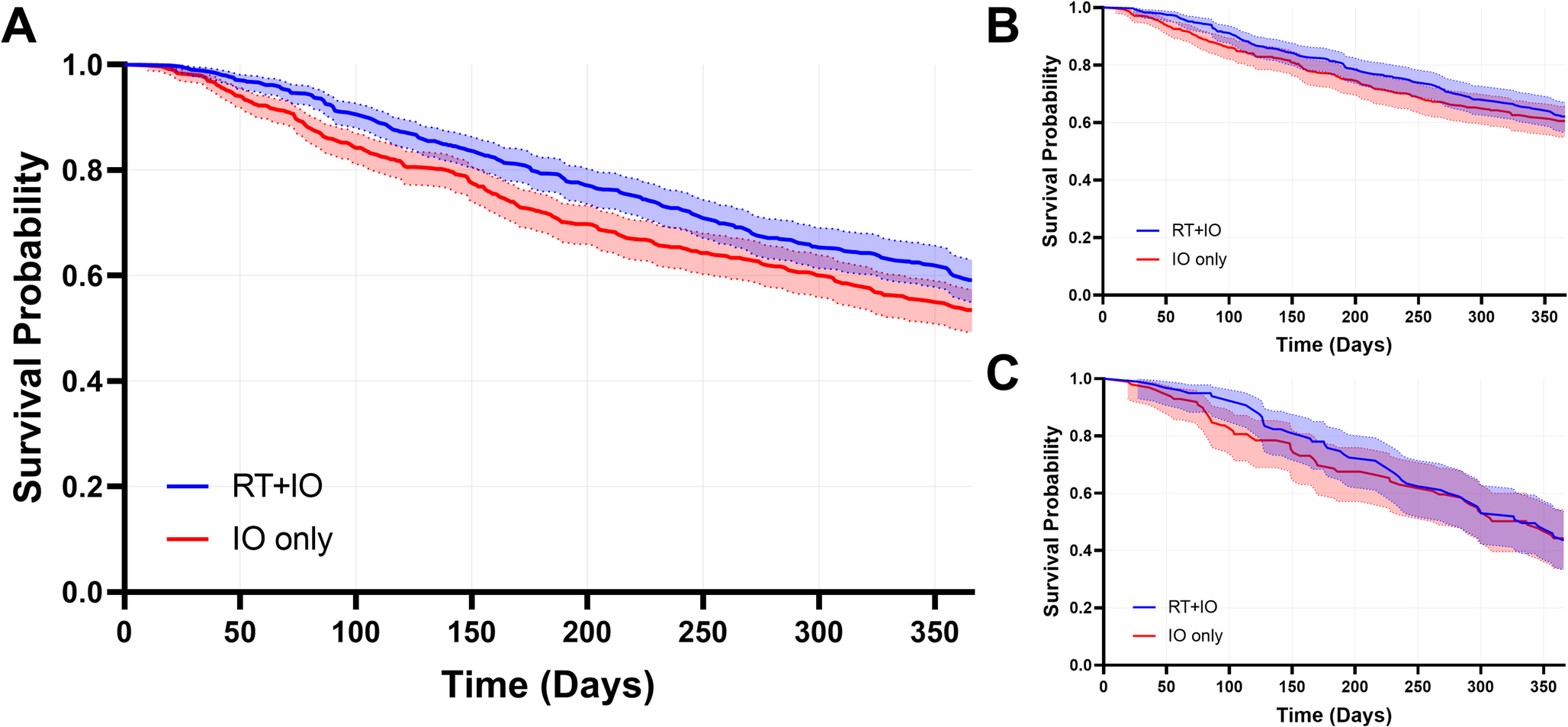
Kaplan–Meier survival analysisKaplan–Meier log-rank testing was used to assess 3-month, 6-month, and 1-year survival outcomes for all histologies combined, as well as for the individual histologic subsets of AC-NOS and SCC-NOS (Table 3). RT was associated with significant improvement in survival in the overall cohort at 3 months (HR = 0.54, 95% CI 0.38–0.76, p < 0.001), 6 months (HR = 0.69, 95% CI 0.55–0.87, p = 0.002), and 1 year (HR = 0.81, 95% CI 0.68–0.96, p = 0.014). At 1 year, the RT + IO group had a survival probability of 59%, compared with 54% in the IO-only group (Fig. 1A), reflecting a 5% absolute improvement in survival. Overall survival was also compared, and while the median survival was not significantly different between groups, median survival was 16.0 months for RT + IO and 14.7 months for IO only. In the AC-NOS subset, RT was associated with significantly better survival at 3 months (HR = 0.62, 95% CI 0.39–0.997, p = 0.046). Differences at 6 months (HR = 0.78, 95% CI 0.56–1.1, p = 0.129) and 1 year (HR = 0.90, 95% CI 0.71–1.2, p = 0.418) were not statistically significant. At 1 year, the survival probabilities of the RT + IO group were 62% and were 61% for the IO-only group (Fig. 1B). In the SCC-NOS subset, RT was associated with significantly improved survival at 3 months (HR = 0.39, 95% CI 0.15–0.99, p = 0.040). Results at 6 months (HR = 0.73, 95% CI 0.43–1.3, p = 0.266) and 1 year (HR = 0.94, 95% CI 0.64–1.4, p = 0.764) again favored the RT + IO group but were not significant. Survival probabilities for both groups were 44% at 1 year. (Fig. 1C).
Fig. 1
Kaplan–Meier survival curves comparing patients treated with immunotherapy (IO) alone versus IO plus radiotherapy (RT) following bone metastasis diagnosis in stage IV NSCLC. Kaplan–Meier curves show overall survival over 1 year by treatment group. Time zero is the date of bone metastasis diagnosis. Panel A displays survival for all NSCLC histologies combined. Panel B shows AC-NOS. Panel C shows SCC-NOS. In all groups, RT + IO is associated with higher survival probability over time
As a sensitivity analysis, survival outcomes were also evaluated in the full, unmatched cohort (Supplemental Table 6). Results were consistent with the matched analysis. For all histologies combined, RT was associated with significantly better survival at 3 months (HR = 0.44, 95% CI 0.32–0.60, p < 0.001), 6 months (HR = 0.63, 95% CI 0.51–0.77, p < 0.001), and 1 year (HR = 0.79, 95% CI 0.68–0.92, p = 0.002). Survival at 1 year was 59% for the RT + IO cohort and 54% for the IO-only cohort. In the unmatched AC-NOS subset, RT + IO was associated with significantly improved survival at 3 months (HR = 0.47, 95% CI 0.31–0.69, p < 0.001), 6 months (HR = 0.67, 95% CI 0.51–0.88, p = 0.004), while 1-year survival (HR = 0.84, 95% CI 0.69–1.0, p = 0.085) was not significant. 1-year survival in the RT + IO group was 61%, with 58% in the IO-only group. In the unmatched SCC-NOS subset, RT was again associated with significantly improved 3-month survival (HR = 0.44, 95% CI 0.20–0.95, p = 0.031) and 6-month survival (HR = 0.62, 95% CI 0.39–1.0, p = 0.048). At 1 year, the difference again favored RT + IO but was not significant (HR = 0.74, 95% CI 0.52–1.0, p = 0.083) with 53% survival in the RT + IO group and 44% survival in the IO-only group. These findings align with the matched results, confirm the robustness of the observed associations, and suggest the survival benefit associated with RT persists even in the absence of matching.
Cox proportional hazards modelA Cox proportional hazards model (Model 1) was constructed using time from the diagnosis of bone metastasis as time zero, with death as the outcome with a time frame of up to 1 year. RT + IO was associated with a significantly lower hazard of death (HR = 0.79, 95% CI 0.69–0.92, p = 0.002). Additional covariates independently associated with increased hazard included adrenal metastasis (HR = 1.8, 95% CI 1.4–2.2, p < 0.001), liver metastasis (HR = 1.4, 95% CI 1.2–1.7, p < 0.001), lymph node metastasis (HR = 1.3, 95% CI 1.1–1.5, p = 0.001), albumin < 3.45 g/dL (HR = 1.5, 95% CI 1.2–1.7, p < 0.001), and inpatient or observation care services (HR = 1.39, 95% CI 1.2–1.6, p < 0.001). Phosphate > 4.40 mg/dL was associated with a lower hazard of death (HR = 0.74, 95% CI 0.56–0.97, p = 0.032), which may reflect underlying nutritional or metabolic differences, or possibly serve as a surrogate for better overall clinical status. Age at index showed a modest but significant association (HR = 1.01, 95% CI 1.002–1.017, p = 0.009). Full model results are shown in Table 4.
Because survival curves between groups appeared more similar during the early follow-up period, suggesting a potential violation of the proportional hazards assumption, two stratified models were also assessed. In Model 2, covering the 0–100 day window (Supplemental Table 7), RT was associated with a substantially lower hazard of death (HR = 0.48, 95% CI 0.37–0.64, p < 0.001), suggesting the protective effect of RT may be strongest in the early period following bone metastasis. Adrenal, liver, and lymph node metastases, low albumin, inpatient/observation care, and older age were also significantly associated with increased mortality in this interval. Phosphate > 4.40 mg/dL was not significantly associated with early mortality (HR = 0.90, 95% CI 0.57–1.42, p = 0.650).
In Model 3, covering the 100-day to 1-year window (Supplemental Table 8), there was no difference in hazard between the RT + IO and IO-only groups (HR = 1.0, 95% CI 0.84–1.2, p = 0.958). Adrenal metastases (HR = 1.7, 95% CI 1.3–2.2, p < 0.001) and liver metastases (HR = 1.3, 95% CI 1.1–1.67, p = 0.016), low albumin (HR = 1.41, 95% CI 1.2–1.7, p < 0.001), and inpatient or observation care (HR = 1.3, 95% CI 1.1–1.6, p = 0.006) remained significant predictors of mortality. Phosphate > 4.40 mg/dL was associated with improved survival (HR = 0.68, 95% CI 0.48–0.95, p = 0.025). Age (HR = 1.0, 95% CI 1.0–1.011, p = 0.494), and lymph node metastases (HR = 1.2, 95% CI 0.99–1.4, p = 0.071) were not significant in this later window.
Comments (0)