
Remember me
The 55 patients diagnosed with PTL from multiple centers in China (Table 1) had a median age of 65 years (range, 23–84 years). The median follow-up was 42 months (IQR, 26–100). Thirty-two patients (58.2%) presenting with advanced-stage disease (Ann Arbor III/IV). Seventeen (30.9%) patients reported B symptoms, and 27 (49.1%) had high or high-intermediate IPI scores. Immunochemical staining was performed on all 55 patients, with 49 (89.1%) diagnosed with DLBCL, of which 39 (70.9%) were classified as the non-GCB subtype. Elevated LDH levels were found in 22 (40%) patients; 7 (12.7%) had bulky disease, and 17 (30.9%) patients had extranodal involvement.
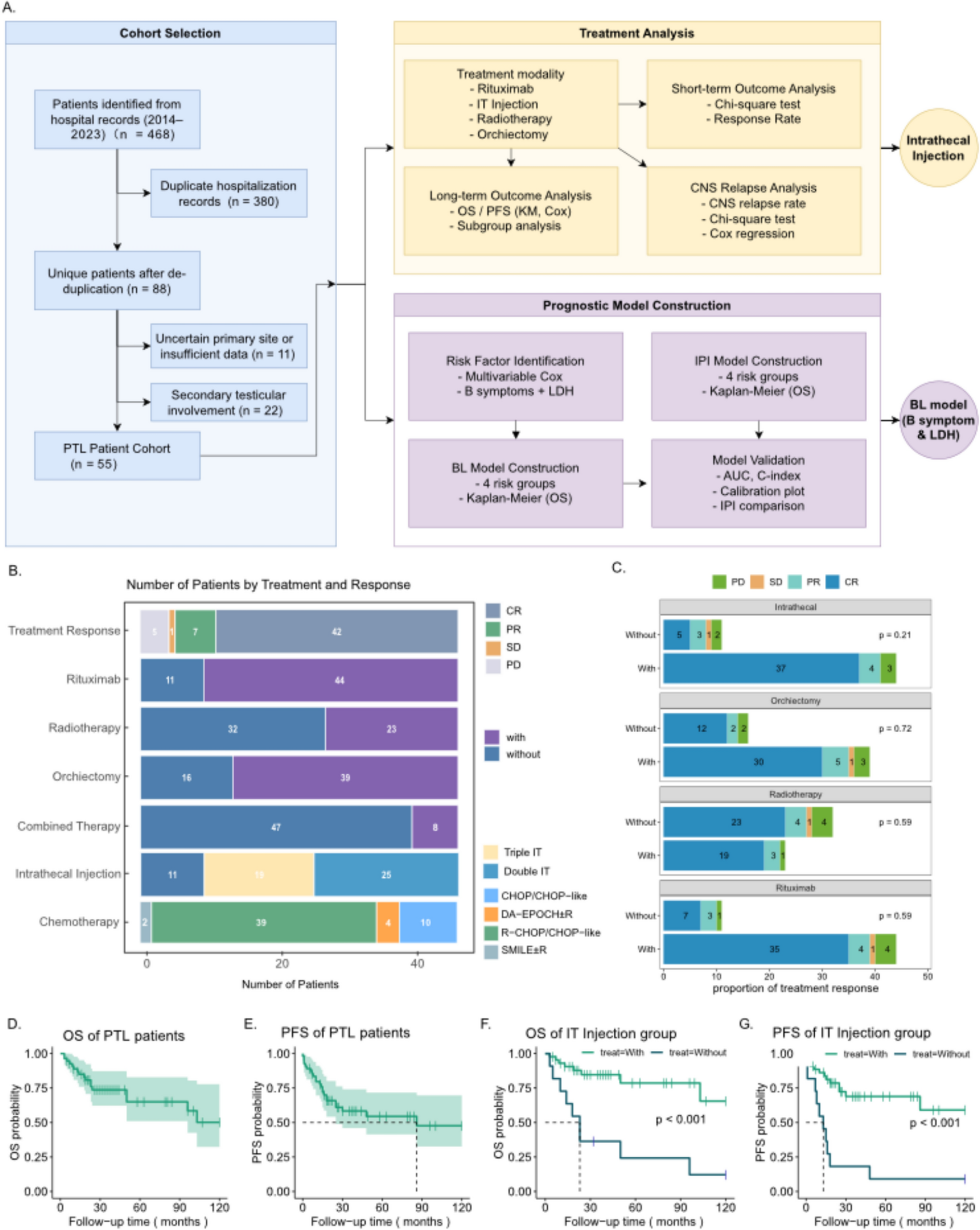
Table 1 Clinical characteristics of primary testicular lymphomaWe conducted a prognostic analysis of each treatment plan, focusing on short-term response, long-term survival, and CNS relapse (Fig. 1A). Among the 55 patients evaluated for therapeutic efficacy (Fig. 1B), CR was achieved in 42 patients (76%), while PR was observed in 7 patients (13%). One patient (1.8%) showed SD, and 5 patients (9.1%) showed PD. The short-term treatment did not show significant differences (Fig. 1C). Forty-four (80%) patients received 4 to 8 cycles of IT prophylaxis and thirty-nine (71%) patients underwent orchiectomy (Fig. 1B). All patients received systemic chemotherapy, and 23 (43%) patients received prophylactic radiotherapy. Forty-nine (89%) patients received R ± CHOP or CHOP-like regimens, while 2 received DA-EPOCH ± R, and 2 received SMILE.
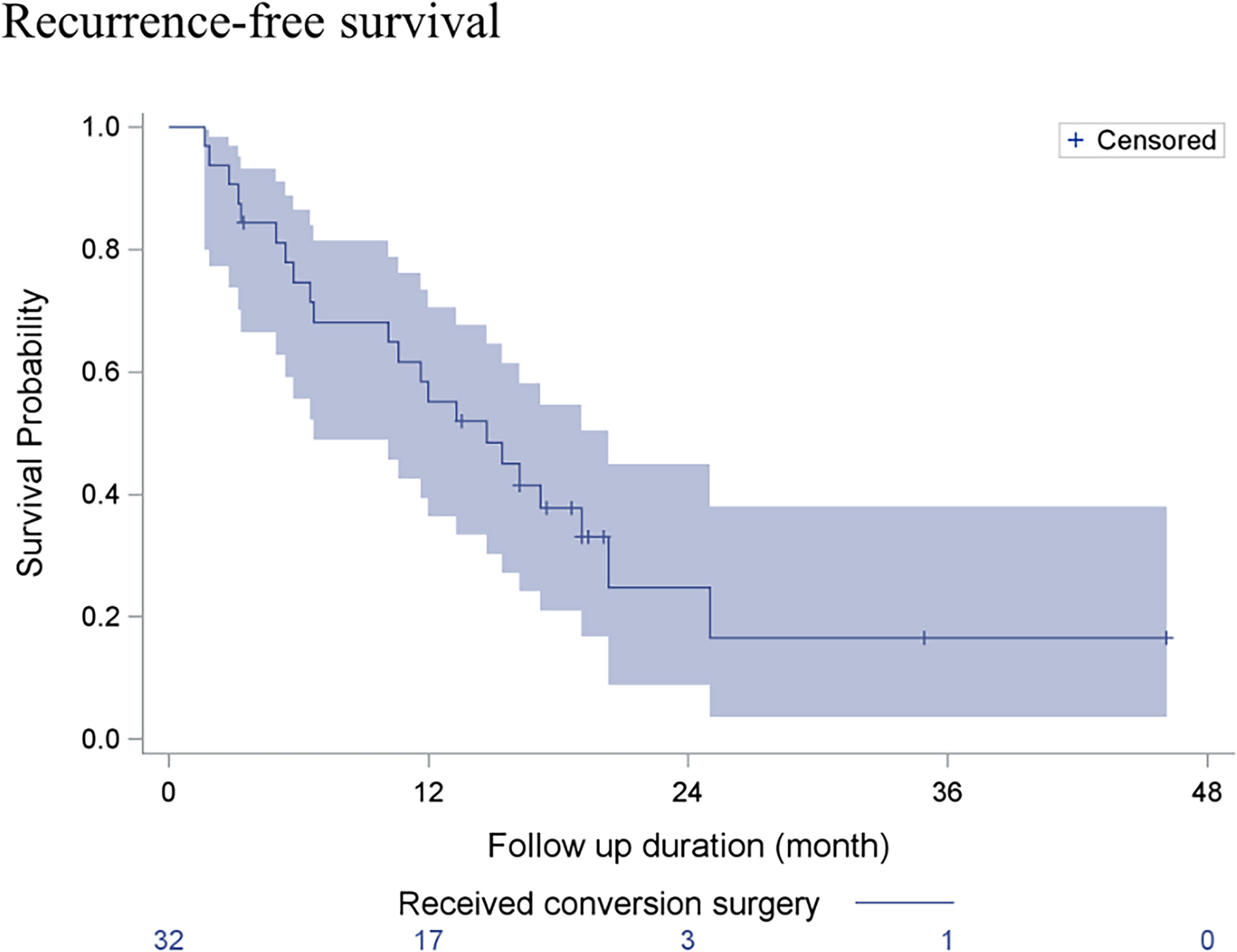
During our follow-up, 18 deaths and 19 relapses occurred. The Kaplan–Meier curves revealed that the estimated 1-year, 3-year, and 5-year OS rates were 88.9%, 73.7%, and 65.0%, respectively (Fig. 1D). The 1-year, 3-year, and 5-year PFS rates were 79.7%, 58.4%, and 54.5%, respectively (Fig. 1E).
Intrathecal prophylaxis improves survival and reduces CNS relapseIT prophylaxis demonstrated a clear survival benefit in patients with PTL in our cohort. Among the 55 patients, 44 received IT prophylaxis, while 11 did not, and related treatment details were summarized (Supplementary Table 1). Patients in the non-IT group experienced significantly worse outcomes, with 10 deaths and disease progression observed in all 11 cases. In contrast, IT prophylaxis significantly improved OS (p < 0.01, Fig. 1F) and PFS (p < 0.001, Fig. 1G), whereas other treatment modalities showed no significant impact on survival in this cohort (Supplementary Fig. 1).
Multivariable analyses confirmed that IT prophylaxis is an independent prognostic factor for improved outcomes classified by across various treatment modalities (Supplementary Table 2), with better OS (HR = 0.18, p < 0.001) and PFS (HR = 0.21, p < 0.001). Subgroup analysis showed that IT prophylaxis significantly improved OS and PFS across multiple subgroups (p < 0.05, Supplementary Fig. 2), with notable benefits in patients with DLBCL, non-GCB subtype, KI67 ≥ 50%, unilateral involvement, stage III/IV, absence of B symptoms, ECOG 0–1, normal ALB, elevated LDH, tumor size < 7.5 cm, ≥ 2 extranodal sites, and across various treatment modalities.
To explore the potential mechanism underlying these benefits, we analyzed CNS and systemic relapse patterns (Fig. 2A). In the non-IT group (n = 11), 10 patients relapsed (90.9%), with 4 experiencing CNS relapse (36.4%) and 6 exhibiting systemic relapse (54.5%). In contrast, the IT group (n = 44) demonstrated a lower relapse rate, with only 4 patients showing CNS relapse (9.1%) and 9 displaying systemic relapse (20.5%). Chi-square testing confirmed a significant difference between the groups (p < 0.001, Fig. 2B). Kaplan–Meier curves illustrated that IT prophylaxis markedly improves CNS relapse-free survival (p = 0.0028, Fig. 2C). Multivariable Cox analysis established IT prophylaxis as an independent factor in reducing CNS relapse risk (HR = 0.15, p = 0.009, Fig. 2D, Supplementary Table 3). No significant difference founded between double IT (methotrexate and dexamethasone) and triple IT (methotrexate, cytarabine, and dexamethasone) regimens (p = 0.914, Fig. 2E; Cox p = 0.6, Fig. 2F). These findings suggest that IT prophylaxis plays a pivotal and independent role in improving survival and reducing CNS relapse in patients with PTL.
Fig. 2
Impact of IT prophylaxis on relapse in PTL patients. A Flowchart from IT regimen to recurrence. B Comparison of relapse rates between IT and non-IT groups. C Kaplan–Meier Curve of CNS relapse-free survival with IT prophylaxis. D Multivariable cox analysis of IT prophylaxis on CNS relapse risk. E Comparison of double IT vs. triple IT on CNS relapse-free survival. F Cox analysis of double IT vs. triple IT on CNS relapse risk
BL—a simplified two-factor prognostic model outperforms the IPITo address the limitations of existing prognostic tools in PTL, we developed a simplified risk model based on two readily accessible clinical variables: B symptoms and serum LDH levels (Fig. 1A, Fig. 3A). Variables with p < 0.1 in univariate Cox regression were included in multivariate analysis, which identified B symptoms (HR = 5.80, p = 0.001) and elevated LDH (HR = 2.98, p = 0.044) as independent predictors of OS (Table 2).
Fig. 3
Prognostic evaluation and validation of IPI and BL models in PTL patients. A Workflow of prognostic model development for PTL patients. B Kaplan–Meier (KM) curve for OS stratified by IPI model. C Time-dependent ROC curves for the IPI model at 12, 36, and 60 months. D KM curve for OS stratified by the BL model. E Time-dependent ROC curves for the BL model at 12, 36, and 60 months. F Time-dependent C-index curves comparing the IPI and BL models. G Calibration plot for OS using the BL model at 12, 36, and 60 months
Table 2 Clinical factors associated with PFS and OS in MCL patients on COX analysisFor benchmark, we first evaluated the performance of the IPI in this cohort. While a significant OS difference was observed between the high- and low-risk groups (p = 0.04, Fig. 3B), the intermediate groups overlapped, and other comparisons did not reach statistical significance (p > 0.05). The AUCs of the IPI for 1-, 3-, and 5-year OS were 0.656, 0.804, and 0.724, respectively (Fig. 3C), indicating modest discriminatory power.
Based on our multivariate results, we constructed a new scoring system—the BL model. Patients were stratified into four risk categories: Low-risk (L): 0 points; Low-intermediate (LI): 1 point for LDH; High-intermediate (HI): 1 point for B symptoms; High-risk (H): both factors present. The BL model demonstrated clear prognostic separation. In OS analysis (Fig. 3D), the high-risk group had significantly worse outcomes than both the low-risk (p < 0.001) and high-intermediate (p = 0.039) groups. The model yielded higher AUCs than the IPI: 0.883, 0.894, and 0.854 at 1-, 3-, and 5-year OS, respectively (Fig. 3E).
Internal validation using 1000 bootstrap resamples further supported the model's robustness. The BL model achieved a corrected C-index of 0.798 (95% CI 0.713–0.883), with time-dependent C-index values ranging from 0.846 to 0.690 across 1 to 120 months. In contrast, the IPI had a lower corrected C-index of 0.716 (95% CI 0.591–0.841), and time-dependent values between 0.793 and 0.592 (Fig. 3F). Calibration curves for 1-, 3-, and 5-year OS confirmed excellent agreement between predicted and observed survival probabilities (Fig. 3G) by 1000 bootstrap, which highlight the BL model as a simple yet powerful prognostic tool that outperforms the IPI in real-world PTL patients.
To assess the robustness of the BL score across different treatment, we performed subgroup analyses based on six key therapies: rituximab, orchiectomy, contralateral testicular irradiation, CHOP-like regimens, R-CHOP/R-CHOP-like regimens, and standard therapy. Five of six comparisons yielded statistically significant results (p ≤ 0.05, Supplementary Fig. 3). Although the standard therapy subgroup (n = 11) did not reach statistical significance, the limited sample size likely contributed to this result, and a consistent trend with the overall cohort was still observed. Time-dependent AUCs in subgroup ranged from 0.795 to 0.903, comparable to the full cohort (0.854–0.894).
Comments (0)