
Remember me
3.1| Characteristics of the patients 630 patients with advanced NSCLC were identified through an electronic database as having received pembrolizumab (monotherapy or combination chemotherapy) and chemotherapy. Among these individuals, 169 patients received pembrolizumab treatment, either alone or in combination with chemotherapy, while 461 patients underwent chemotherapy. The baseline demographic, clinical, and pathologic characteristics of the 630 patients were displayed in Table 1. The gender differences, TNM stage, pathological histology, the number of treatment lines (first/second-line treatment), and smoking status between the two groups before PSM were statistically significant (p < 0.05). After matching, the differences in other confounding variables between the two groups became statistically insignificant (p > 0.05).
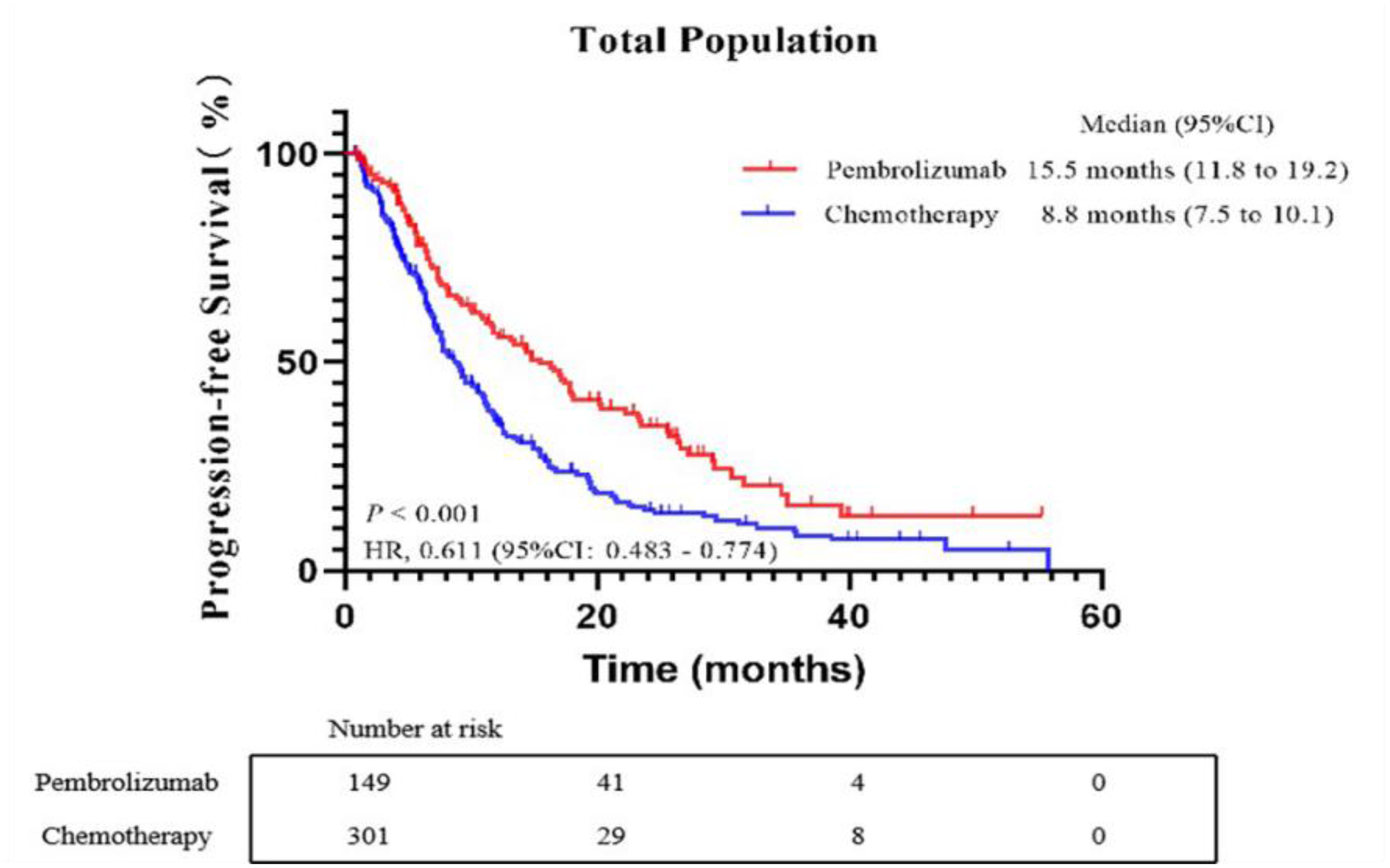
Table 1 Baseline characteristics and treatment details of NSCLC patients receiving pembrolizumab or chemotherapySurvival analysisAt the final evaluation point, out of the total patients, 281 (63.00%) experienced disease progression. Specifically, in the pembrolizumab group, 91 patients (62.33%) had disease progression, while in the chemotherapy group, this number was 190 (63.30%). The median PFS was notably different between the two groups: patients in the pembrolizumab group had a median PFS of 15.5 months (95%CI: 11.819.2), in contrast to the chemotherapy group, which had a median PFS of 8.8 months (95%CI: 7.510.1). This difference was statistically significant, with a Hazard Ratio (HR) of 0.611 (95% CI, 0.4830.774; p < 0.001), as illustrated in Fig. 1. For patients in the pembrolizumab group, the median OS had not been reached at the time of analysis. In contrast, for those in the chemotherapy group, the median OS was recorded at 26.2 months (95%CI: 0.483–0.774). The difference in survival outcomes between the two groups was significant, with an HR of 0.532 (95%CI, 0.399–0.709; p < 0.001), as depicted in Fig. 2.
Fig. 1
Kaplan-Meier curves of progression-free survival (PFS) comparing the pembrolizumab group and chemotherapy group. CI, confidence interval; HR, hazard ratio
Fig. 2
Kaplan-Meier curves of overall survival (OS) comparing the pembrolizumab group and chemotherapy group. CI, confidence interval; HR, hazard ratio
Cost-effectiveness analysisThe K-M survival plots for PFS and OS in both the pembrolizumab and chemotherapy groups were derived from the dataset. These plots were tailored to individual patient data, and the corresponding fitted outcomes can be found in Table 2. The best-fit distribution of the survival curves was judged based on the AIC value of each fitted distribution and the smaller the AIC value, the better the fit of the distribution. The best-fit distributions for the K-M survival curves of PFS and OS in both the pembrolizumab and chemotherapy groups were identified as log-normal distributions. The results of the fitted distribution parameters for each survival curve model are shown in Table 3.
The study encompassing 450 patients, which assessed the efficacy and safety of pembrolizumab and chemotherapy groups, compiled treatment regimens from the initiation of therapy to the first occurrence of PD. It also documented subsequent treatment strategies post-PD. The varieties of anticancer drugs utilized in these regimens are detailed in Additional file 1: Table S1. The cost of the relevant drugs was obtained from the Guangdong Provincial GPO platform. The expense for each cycle of various anticancer medications was determined using the treatment dosage guidelines for different drugs specified in the 2022 CSCO NSCLC treatment guidelines. This calculation was combined with the characteristics of a hypothetical patient, who has a Body Surface Area (BSA) of 1.80 m², weighs 65 kg, and has a Creatinine clearance rate (Ccr) of 90 ml/min/1.73 m². The upper and lower bounds of the drug costs were estimated by adjusting the drug cost by ± 20%. A uniform Gamma distribution was selected for the cost variability of drug treatments.
Drawing from the findings of the aforementioned safety assessment, significant non-immune-related adverse reactions observed in both the pembrolizumab and chemotherapy groups include anemia, neutropenia, and thrombocytopenia. These will be factored into the cost calculation for adverse reactions, incorporating negative utility values for such reactions. The costs for prevention and treatment of adverse reactions, screening, and supportive care described above were obtained from published literature and were shown in Additional file 1: Table S2.
The study calculated utility values for patients without disease progression and those with disease progression, as well as negative utility values for three severe adverse reactions: anemia, neutropenia, and thrombocytopenia. Both the utility values for patients and the negative utility values for adverse reactions were sourced from literature (Additional file 1: Table S3). All utility value data were subjected to ± 20% as upper and lower limits of utility values, and Beta distribution was chosen.
Table 4 displays the outcomes of the cost-effectiveness analysis comparing the pembrolizumab group to the chemotherapy group, excluding the impact of any complimentary drug policy. For the chemotherapy group, the average cost per patient was $81,784, with an average QALY of 2.63. In contrast, the pembrolizumab group experienced an enhanced clinical benefit of 1.69 QALY, but at an increased cost of $329,021, resulting in an ICER of $146409.07/QALY when compared to the chemotherapy group.
Table 4 presents the cost-effectiveness analysis results for the pembrolizumab group versus the chemotherapy group, considering the complementary drug policy. In this analysis, the average cost for the chemotherapy group was $59,112 per patient, with a mean QALY of 2.63. The pembrolizumab group, on the other hand, showed a clinical benefit increase of 1.69 QALY but incurred a higher cost of $153,893. This resulted in an ICER of $56127.74/QALY in comparison to the chemotherapy group.
Table 2 K-M survival curve fitting results for PFS and OS in the pembrolizumab and chemotherapy groupsTable 3 Survival curve distribution parametersTable 4 Results of cost-utility analysisSensitivity analysisThe study conducted a DSA on several cost parameters including drug costs, utility values for two disease states, associated screening and treatment expenses, and utility values for adverse effects, with variations set at ± 20% of their base values. The WTP threshold was set at three times China’s GDP per capita for the year 2022. The findings indicated that the price of pembrolizumab, the utility values associated with disease progression and non-progression, and the cost of CT scans significantly influenced the outcomes, both with and without the consideration of complementary drugs. These results are depicted in Figs. 3 and 4. It was also noted that a reduction in the price of pembrolizumab would lead to a further decrease in the ICER values.
This study conducted a PSA through 1000 Monte Carlo simulations, as shown in Figs. 5 and 6.
From the cost-effectiveness acceptability curves, it’s evident that when comparing the pembrolizumab group (without complimentary drugs) and the chemotherapy group, as well as the pembrolizumab group (with complimentary drugs) against the chemotherapy group, the chemotherapy group attains 100% acceptability at a cost threshold of approximately three times China’s GDP per capita ($36070.2), outperforming the pembrolizumab group. Additionally, in the pembrolizumab group with complimentary drugs, its cost-effectiveness acceptability curve relative to the chemotherapy group indicates that at a threshold of three times Guangzhou’s per capita GDP ($64523.8), pembrolizumab achieves 100% acceptability.
Fig. 3
Tornado chart for one-way sensitivity analysis (Free medication is not considered)
Fig. 4
Tornado chart for one-way sensitivity analysis (Consider Medication giveaways)
Fig. 5
Curves of cost-effectiveness acceptability (Free medication is not considered)
Fig. 6
Curves of cost-effectiveness acceptability (Consider Medication giveaways)
Comments (0)