
Remember me
Cone-beam computed tomography data for PMCIs were collected from CBCT scans of children aged 3–6 years who visited Peking University Hospital of Stomatology between January 2019 and April 2022. The scans were obtained for clinical diagnosis and treatment purposes unrelated to the present study. Qualified CBCT files were documented in the Digital Imaging and Communications in Medicine format. All procedures complied with the relevant laws and institutional guidelines. The requirement for informed consent was waived by our institution’s Ethics Committee, because the present study involved retrospective analysis of anonymised data and there was no additional risk to participants. The study was approved by the Ethics Committee (approval number: PKUSSIRB-202281147).
Inclusion/exclusion criteriaThe inclusion criteria included clear scans with full images of PMCIs showing complete apical development, no morphological abnormalities (for example, significant abnormalities in tooth size and shape, such as fused teeth, malformed cusps, dens invaginatus, and tooth dilacerations), no dental hard-tissue injury or caries lesion extending into the dentine layer radiographically, no internal or external root resorption, and no prior treatment. Scans with substantial motion artifacts were excluded.
Sample size calculationA pilot study was conducted to determine the appropriate sample size. The calculation was performed using PASS 2021 (NCSS LLC., Kaysville, UT, USA), with an alpha error of 0.05, an allowable error of ± 0.5 mm, and a known standard deviation of the length from the roof of pulp chamber to the root canal apex (this parameter was chosen to provide guidance for root canal treatment). The estimated sample size for each variant was 16.
Radiographic techniquesThis study was a retrospective study of previous data, and all CBCT scans were obtained for diagnose purposes unrelated to the study. Considering the requirements for imaging reconstruction accuracy, CBCT scans with the minimum slice thickness were selected. The 3D Accuitomo CBCT machine (J. Morita Manufacturing Corp., Kyoto, Japan) was used to obtain images with a voxel size of 0.125 mm. All images were acquired by licensed radiologists at 90 kV and 5.0 mA with an exposure time of 17.5 s.
Sample model reconstruction and analysisTo ensure the accuracy of our results, all researchers have undergone necessary training processes to master the digital software involved and have passed the relevant examinations.
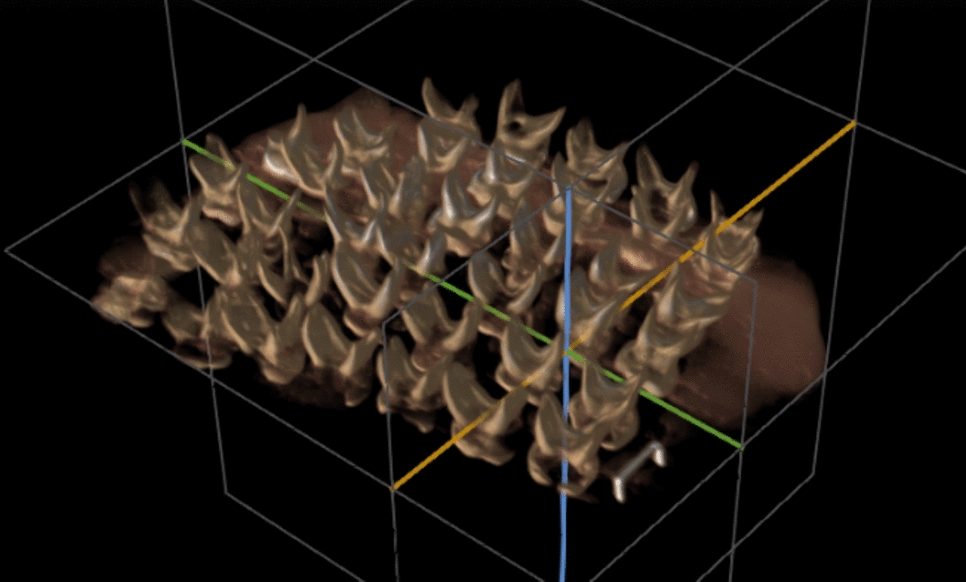
3D modellingThe 3D morphology of the hard tissues and pulp cavity of PMCIs was obtained using Mimics 24.0 (Materialize Nv, Leuven, Belgium), based on a threshold-based semi-automatic segmentation method, which was then manually corrected. The PMCI models were reviewed by two paediatric dentists with over 20–30 years of clinical experience to ensure that they were consistent with the original CBCT, then exported in “.stl” format. In the case of differing opinions between the two experts, consensus was reached after discussion (Fig. 1).
Fig. 1
Segmentation and coordinate adjustment. a Threshold selection for hard tissue; b threshold selection for pulp chamber and canal; c extracted hard tissue (blue) and pulp chamber and canals (red); d profile lines for hard tissue (blue) and pulp chamber and canals (red), consistent with the original cone-beam computed tomography (CBCT) scan; e coordinate axes adjustment. Point A indicates the midpoint of the section at the apical labial curvature
Coordinate adjustmentThe coordinate axis of the model was adjusted in Geomagic Control X (3D Systems Corp., Rock Hill, SC, USA), using the same criteria such that the connection line between the two pulp horns was aligned with the system’s x-axis; the line passing through the midpoint of the section at the apical labial curvature (point A) and perpendicular to the x-axis was aligned with the z-axis; and the line passing through the intersection of the x- and z-axes and perpendicular to these two lines was aligned with the y-axis (Fig. 1).
2.5.3. Variation observation and model classificationA paediatric dentist observed the models from the coronal, sagittal, and vertical axes, classifying them by root numbers and root canal types according to the Vertucci classification (Vertucci 1984). The classifications were reviewed by a paediatric specialist with over 30 years of clinical experience and four other paediatric dentists. The observers were trained in morphological classification and passed the relevant examinations; thereafter, a pilot study was conducted to perform a standard consistency test on results of tooth-anatomy classifications by the observers. The Fleiss Kappa coefficient was 0.9 for inter-observer agreement, and the mean Cohen's Kappa was 0.96 for intra-observer reliability when reassessed after 1 month.
Measurements of hard-tissue featuresThe total length (L), crown height (H), crown width (W), and height-to-width ratio (R) of the crown were selected as representative morphological parameters of the hard tissues. A labial curvature was observed in the middle or apical third of all PMCI roots, dividing the length of the whole tooth into coronal (CL) and apical (AL) segments, bounded by point A (Fig. 1).
Measurements of pulp chamber and canalsThe volume (v) of the pulp chamber and canals was determined first. The entire length of the pulp chamber and canals (l) was then measured along the direction of each root canal, with multiple measurements taken if more than one canal was present. Considering the significant labial curvature of PMCIs, (l) was divided into a coronal segment (cl) and an apical segment (al). The ratio of the apical segment to the total length (p) was calculated. The distance (da) from the canal terminus to the anatomical apex of the root was also recorded (Fig. 2). The intersection angle between the coronal and apical sections of the canals was defined as the apical labial curvature angle (α), with an average angle recorded if multiple canals were present. A cross-section of the pulp cavity was made at half the root length, and its mesiodistal diameter (mdd), labio-palatal diameter (lpd), and mesio-distal-to-labio-palatal diameter ratio (r) were measured.
Fig. 2
Variants of primary maxillary central incisors (PMCIs). a Type I: A single canal extending from the pulp chamber to the canal terminus, illustrated with a CBCT example and a distinct reconstructed tooth model. b Type III: A single canal bifurcating into two canals, which converge into one near the canal terminus; includes a CBCT example and a reconstructed tooth model (tooth labelled 61 was also Type III but excluded due to root resorption). c Type V: A single canal that bifurcates into two distinct canals before reaching the canal terminus; includes a CBCT example and a reconstructed tooth model. CBCT, cone-beam computed tomography
Construction of the main-type average modelThe variant with the highest prevalence amongst the PMCIs was defined as the main type, and an average model was created.
Template selectionThe model with morphological parameters closest to the average was selected as the reference template for subsequent 3D averaging.
Model mirroringIf no discernible difference existed between the left and right sided teeth, all tooth models on the left side were mirrored using Geomagic Control X. A common average model was then calculated for both sides. For positional differences, separate average models were computed for each side.
Labelling of characteristicsFeature points on the external surface of the hard tissue and pulp cavity were selected as alignment landmarks. The coordinates (X, Y, and Z) of each landmark were manually identified three times. The mean value of these coordinates served as the final result, recorded in “.csv” format (Fig. 3).
Fig. 3
Alignment landmarks on hard tissue and pulp cavity. For hard tissue: Pt 1—apex of the root; Pt 2—most convex point on the cingulum; Pt 3—vertex of the mesial incisal angle; Pt 4—vertex of the distal incisal angle. For pulp cavity: Pt 1—most concave point on the labial side; Pt 2—most convex point on the palatal side; Pt 3—most mesial point at the root canal orifice level; Pt 4—most distal point at the root canal orifice level; Pt 5—most convex point on the lingual side of the pulp chamber; Pt 6—mesial pulp horn; Pt 7—distal pulp horn; Pt 8—centre point of the roof of the pulp chamber
Size normalization and alignmentThe landmark coordinate set files of the selected reference template and remaining models were imported into MATLAB R2019b (MathWorks Inc., Natick, MA, USA). Using the Procrustes Analysis (PA) algorithm, size scaling coefficients and rotation matrices were determined for the remaining models based on the reference template (Gower 2001; Wen et al. 2022). These values were then applied to the corresponding models in Geomagic Control X to achieve size normalisation and alignment for all models.
Average model constructionUsing the “Average” function in Geomagic Control X with the “Minimum Deviation” standard, the average models of the hard tissues as well as pulp chamber and canal were generated, respectively.
Statistical analysisAll statistical analyses were performed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA). The measurement indices were tested for normality using the Kolmogorov–Smirnov (K–S) test and for homogeneity of variance, with position (left and right) and sex as categorical variables. For indices that were normally distributed and homogeneous, comparisons were made using an independent sample t-test. For indices that did not conform to a normal distribution, the Mann–Whitney U test was employed. Subsequently, the same tests were conducted using the type of variation as a categorical variable. The significance level (alpha level) was set at 0.05.
Comments (0)