Study design and setting
This cross-sectional study was conducted between November 2023 and November 2024 at the Pratheeksha Child Development Centre, Pushpagiri Institute of Medical Sciences, and the Department of Periodontology, Paediatric and Preventive Dentistry, Pushpagiri College of Dental Sciences, Kerala, India. The study protocol was approved by the Institutional Ethics Committee (Ref. No. PIMS/IEC/2023/45), and all procedures were performed in accordance with the Declaration of Helsinki.
Study population and sampling
A total of 300 children aged 3–12 years were enrolled. Participants were recruited via convenience sampling. All eligible SHCN children attending the outpatient and therapy departments during the study period were invited consecutively until the target sample size for that group was reached. To ensure comparability, controls were purposively selected from a larger pool of school-going and outpatient children from the same institution to achieve overall matching for age (± 6 months) and gender. A few SHCN children could not participate due to non-cooperation or caregiver unavailability despite repeated behaviour management attempts.
Participants were divided into two groups: the SHCN group (n = 150) and a matched healthy control group (n = 150). SHCN participants were recruited from the outpatient and therapy departments of the Pratheeksha Child Development Centre, while controls were recruited from local schools and pediatric outpatient clinics of the same institution. Controls were matched to SHCN participants for age (± 6 months) and gender to ensure comparability. Due to the heterogeneity of the SHCN population, exact matching was not feasible, and some variability in demographic characteristics remained.
The SHCN group included children with at least one diagnosed condition, such as neurodevelopmental disorders (e.g., autism), intellectual disability, speech and language disorders, motor disorders (e.g., cerebral palsy), developmental delay, seizure disorders, or multiple/complex disabilities (e.g., Down syndrome). Categories were defined based on the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) and International Classification of Diseases (ICD-11) diagnostic criteria. Diagnoses were confirmed through official medical records and recent consultation notes from pediatricians, neurologists, psychiatrists, or speech–language pathologists. Caregiver interviews further verified diagnosis, treatment history, and duration of the condition. Children with more than one condition were classified under multiple/complex disabilities. Children with no diagnosed medical, neurological, or developmental conditions formed the control group.
Inclusion and exclusion criteria
Eligible participants were children aged 3–12 years whose parents or legal guardians provided written informed consent. SHCN children required a documented diagnosis confirmed by a pediatrician or relevant specialist. Exclusion criteria included acute systemic illness at the time of examination, incomplete clinical or behavioral data, or persistent non-cooperation despite standard behaviour management techniques. These criteria ensured participant safety and reliable assessments, and multiple behaviour management attempts were made before exclusion.
Sample size calculation
Sample size was calculated using G*Power version 3.1 for a chi-square test comparing proportions between SHCN and control groups. Assuming an effect size (w) of 0.3 (moderate association per Cohen’s convention), a power of 95% (1–β = 0.95), and α = 0.05, the required sample size was approximately 134 per group. The final sample size of 300 (150 SHCN and 150 controls) was determined after considering both statistical and practical factors. This increase accounted for possible dropouts, incomplete data, and non-cooperation during examinations. Given the heterogeneity of the SHCN population, a larger sample enabled subgroup analyses and improved the precision and generalizability of results, while remaining feasible within the study sites and recruitment period.
Data collection
Data were collected by calibrated examiners through structured interviews and clinical examinations.
Demographic and background data
Parents or caregivers completed a structured questionnaire covering: age, gender, medical history, birth information, oral hygiene practices (brushing frequency, fluoride toothpaste use, parental assistance), dietary preferences (cariogenic vs. non-cariogenic, based on a food frequency chart) (Bowen et al. 2012), and reported oral habits (mouth breathing, bruxism, nail biting, object biting, self-injurious behaviors).
Behavioral and functional assessments
Behavioral cooperation was evaluated using the FBRS (Frankl 1962), a validated four-point ordinal scale: (1) Definitely Negative, (2) Negative, (3) Positive, (4) Definitely Positive. Ratings were assigned by the examiner based on overall behavior. The FBRS informed adaptations in the examination protocol (e.g., knee-to-knee positioning, distraction techniques) to optimize comfort and data completeness.
Clinical examination
Oral examinations were conducted in a child-friendly environment using either an adjustable dental chair or a knee-to-knee position, depending on age, cooperation, and physical limitations. Sterile diagnostic instruments (mouth mirror, explorer, periodontal probe) and headlamps/flashlights were used for adequate illumination. The Tell-Show-Do technique was consistently applied to encourage cooperation.
Oral health assessments
Standardized clinical examinations assessed:
1.
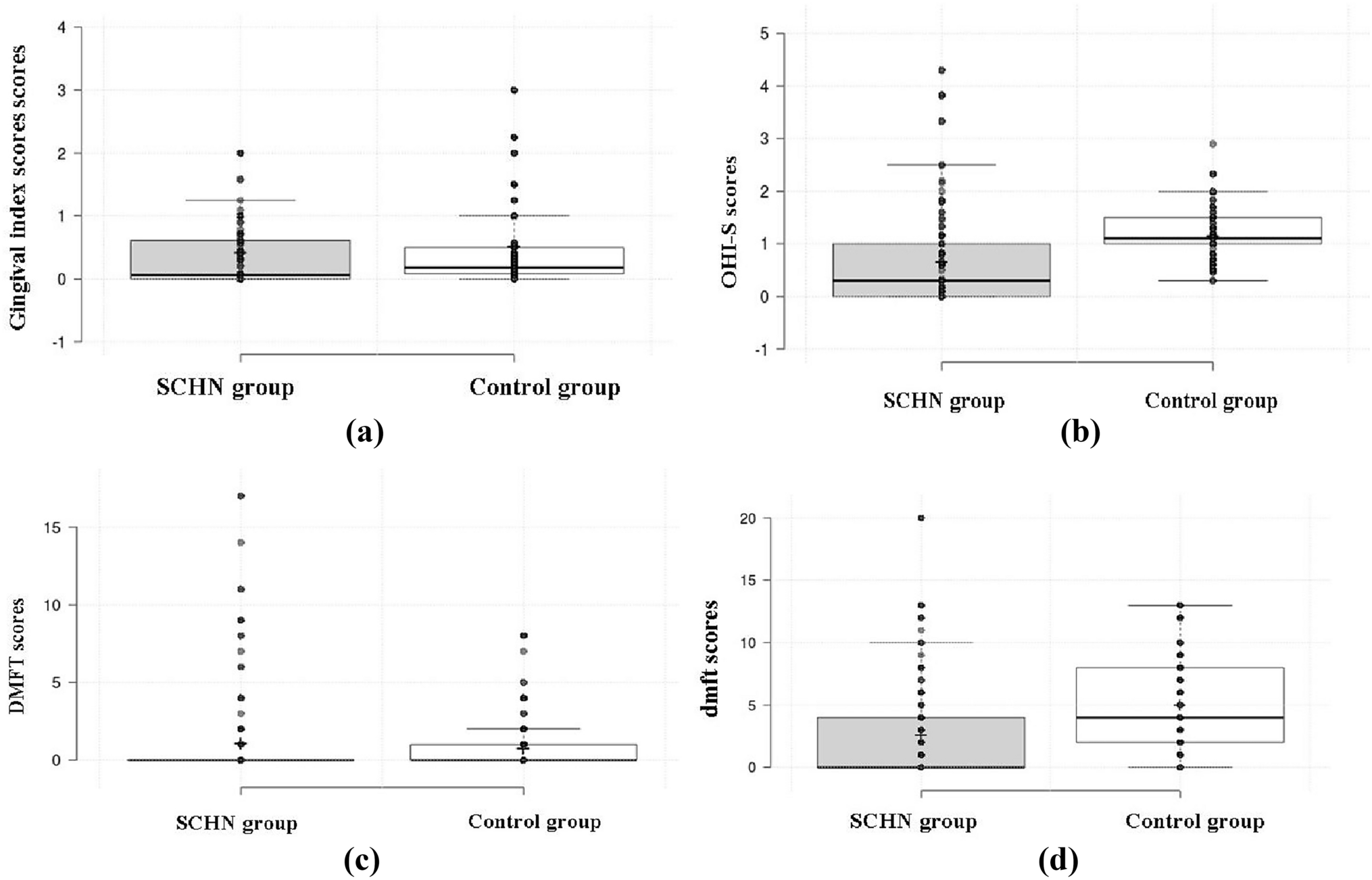
Oral hygiene and gingival health determined via Plaque Index (Silness and Löe 1964) and Gingival Index (Löe and Silness 1963).
2.
Caries experience recorded via dmft/DMFT indices (WHO 2013), with lesion activity classified using Nyvad’s criteria (WHO 2013).
3.
Oral habits identified via clinical observation and caregiver reports, documenting parafunctional behaviors (mouth breathing, digit sucking, bruxism, lip/nail biting, self-injury).
4.
Dental trauma classified using Andreasen’s criteria (enamel fracture, luxation, avulsion).
Examiner calibration
All clinical examinations were performed by two postgraduate residents Periodontology and Pediatric and Preventive Dentistry who had prior experience in oral health assessment of children with SHCN. Before data collection, both examiners underwent a comprehensive training and calibration session led by a senior faculty member Department of Periodontology and Pediatric and Preventive Dentistry, Pushpagiri College of Dental Sciences to ensure uniform understanding and application of diagnostic criteria.
Calibration involved the clinical assessment of 20 children (not included in the study sample), followed by discussion and consensus on diagnostic discrepancies. Reliability was re-evaluated after one week on 10% of the study participants to determine intra- and inter-examiner agreement. The Cohen’s kappa values for categorical variables and Intraclass Correlation Coefficients (ICC) for quantitative measures were both above 0.85, indicating excellent reproducibility.
Statistical analysis
Data were analyzed using SPSS version 27 (IBM Corp., Armonk, NY, USA). Descriptive statistics (means, standard deviations, frequencies) summarized demographic and clinical data. Group differences were assessed with inferential statistics. Multivariable linear regression was used to identify predictors of dmft scores in SHCN children. Independent variables included group type, age, brushing frequency, resistance to brushing, and preference for sweets. The analysis assessed predictor significance and the variance in dmft scores explained by the model.

Comments (0)