Restoration of decayed or compromised primary anterior teeth presents a multifactorial challenge, particularly in young children where aesthetics, durability, and gingival health are key concerns. This systematic review synthesised evidence from seven RCTs comparing prefabricated ZCs with alternative full-coverage restorations. Across all trials, ZC demonstrated superior outcomes in retention, gingival health, plaque accumulation, and aesthetics, with no recurrent caries reported in ZC groups in most studies. CSC had higher rates of failure, caries, and poorer aesthetics. These findings are consistent with previous clinical and observational studies that have reported favourable performance of ZCs in paediatric anterior restorations (Alhissan and Pani 2021; Yanover et al. 2021a; Yanover et al. 2021b). However, a consistent concern was opposing enamel wear associated with ZC.
Retention and material stability are critical for long-term clinical success. ZCs achieved high retention rates, often reaching or approaching 100% at follow-up points ranging from 6 to 18 months (Özdemir et al. 2022; Ravada et al. 2022; Vaghela et al. 2021). In contrast, CSCs showed notably lower retention, with failures often attributed to their technique sensitivity and dependency on moisture control and the need for sufficient tooth structure for bonding (Gill et al. 2020; Misgar et al. 2022; Özdemir et al. 2022). One trial reported a retention rate of only 77.8% for CSCs compared to 100% for ZCs at 18 months (Özdemir et al. 2022), which aligns with previous findings of Gill et al. (2020), who reported 95% retention for ZCs versus 79% for CSCs at 12 months. Longer-term retrospective data reinforce these findings. Kupietzky et al. (2003) retrospectively evaluated 112 CSCs in 40 children and found an 88% retention rate after approximately 18 months, with none of the restorations being completely lost and only 12% showing partial resin loss. In an extended follow-up, Kupietzky et al. (2005) examined 145 CSCs and observed a slightly reduced retention rate of 80% after an average of 31.3 months, with partial loss of resin in 20% of cases but no complete failures. These findings confirm that CSCs can perform acceptably over time but remain vulnerable to marginal breakdown and chipping. Earlier research emphasised the clinical reliability of ZCs in young children, even in high-risk cases requiring pulp therapy or extensive coronal coverage (Alrashdi 2024; Rocha et al. 2021).
It is worth noting, however, that not all evidence favours zirconia in every context. A recent 2.5-year retrospective cohort study found significantly higher failure rates in ZCs compared to stainless steel crowns following pulpotomy in primary molars (Brenner et al. 2025). Importantly, these failures were primarily linked to pulpotomy outcomes rather than crown integrity, as the major complications included abscess and fistula. Whilst these findings pertain to posterior teeth and different clinical scenarios, they emphasise the need for cautious extrapolation and longer-term anterior-specific trials.
CSC are also prone to chipping and material loss, likely due to bonding failure or marginal leakage (Özdemir et al. 2022; Misgar et al. 2022). Conversely, ZCs, with their monolithic design and use of resin-modified glass ionomer cement (RMGIC), provide more stable outcomes and minimise marginal failures (Vaghela et al. 2021; Ravada et al. 2022). These advantages reflect zirconia’s high flexural strength, fracture resistance, and reduced susceptibility to microleakage compared to composite restorations (Waggoner and Cohen 1995; Alonso and Caserio 2012).
ZCs consistently outperformed CSCs in preserving gingival health. Their highly polished, biocompatible surfaces limit bacterial adhesion and biofilm formation, which likely explains the lower bleeding and inflammation scores observed clinically (Özdemir et al. 2022). Alaki et al. (2020) demonstrated significantly reduced plaque accumulation and gingival bleeding in ZC-treated teeth compared to CSCs after 12 months. Further supporting this, Mathew et al. (2020) found that Streptococcus mutans adhered less to posterior zirconia surfaces compared to stainless steel crowns, with lower plaque scores and gingival inflammation sustained across a 12-month follow-up period. Immunological and microbiological findings also echo this trend. Saharia et al. (2024) reported that children restored with posterior ZCs exhibited lower interleukin-6 (IL-6) levels and reduced Lactobacillus casei counts compared to those with stainless steel crowns, indicating better periodontal tissue response and lower microbial colonisation. These findings highlight zirconia’s favourable interaction with the surrounding gingival environment. Moreover, Abdelhafez and Dhar (2025) compared posterior stainless steel crowns, ZCs, and Bioflx crowns and found that zirconia showed superior results in terms of plaque control and gingival index at both 6- and 12-month assessments. Nonetheless, some variability in results was observed in the present review. One study reported that both ZC and CSC groups exhibited gingival inflammation that was higher than the caries-free control group, likely due to poor oral hygiene and the increased mobility of exfoliating incisors (Özdemir et al. 2022). The authors also noted that limited brushing compliance, especially during the COVID-19 pandemic, might have contributed to poorer outcomes, irrespective of crown material. These challenges highlight the importance of parental support and oral hygiene instruction following crown placement, regardless of the restoration used.
Aesthetics was a central concern across most trials, with ZCs consistently outperforming CSCs in both parental and child satisfaction measures (Gill et al. 2020; Labbé et al. 2023; Vaghela et al. 2021). Whilst CSCs offer good initial aesthetics with customisable shades, their colour stability deteriorates over time due to surface roughness, staining, and marginal breakdown. Vaghela et al. (2021) reported that 29.4% of CSCs exhibited shade mismatch at 9 months, whereas ZCs maintained 100% colour stability. These findings reinforce conclusions from earlier studies reporting that discoloration and chipping are major limitations of CSC in long-term use (Alonso and Caserio 2012). These aesthetic limitations were also documented by Kupietzky et al. (2003), who noted that teeth receiving pulpotomy prior to CSC placement frequently displayed significant colour mismatch, especially when obturated with iodoform-based pastes. Furthermore, in a follow-up study of caregiver perspectives, Kupietzky and Waggoner (2004) found that although colour mismatch was the most common aesthetic complaint amongst parents, it did not significantly affect overall satisfaction. Interestingly, the study revealed a statistically significant relationship between perceived durability and overall satisfaction, suggesting that function and longevity may outweigh cosmetic imperfections in caregiver perception. Children’s perspectives further reinforce the advantage of zirconia. Surveys using Likert scales and smiley face evaluations revealed that children expressed greater satisfaction with ZCs, often citing durability and aesthetics as reasons (Murali et al. 2022; Özdemir et al. 2022; Vaghela et al. 2021). For instance, 92.8% of children rated ZCs as "very happy" at 9 months compared to only 66.7% for CSCs (Özdemir et al. 2022). These results echo prior research that emphasises the increasing aesthetic awareness of both caregivers and paediatric patients, and the important psychosocial role of anterior dental appearance in early childhood (Lee 2002).
Enamel wear on opposing dentition emerged as a concern in some of the included trials. Ravada et al. (2022) reported wear in 10 opposing teeth restored with ZCs at 12 months, whereas no wear was recorded in the CSCs. Similarly, Alaki et al. (2020) found enamel wear in 11.7% of opposing teeth after 12 months in the ZC group, compared to none in the CSC group. Such concerns are consistent with earlier in vitro research showing that zirconia, whilst biocompatible, may exhibit abrasive effects on antagonist teeth over time (DeLong et al. 1989).
However, such wear was not a universal finding. Trials with shorter follow-ups reported no differences. Vaghela et al. (2021) and Özdemir et al. (2022) both found no evidence of opposing enamel wear up to 9–18 months. Given the short functional lifespan of primary dentition, the clinical impact of enamel wear remains uncertain, but careful occlusal adjustment may help minimise risk.
Regarding pulpal health, no significant differences were found between ZCs and CSCs in the majority of the studies. Although ZCs generally require more extensive tooth preparation, which may theoretically increase pulpal stress, none of the included studies reported adverse pulpal outcomes directly attributable to ZC use. Radiographic follow-up in multiple trials confirmed that both crown types preserved pulpal vitality over time (Labbé et al. 2023; Misgar et al. 2022). These findings are supported by prior clinical evidence indicating that when proper restorative technique is followed, ZCs do not compromise biological safety, even in endodontically treated teeth (Walia et al. 2014).
The findings of this review indicated that ZC demonstrated superior outcomes in retention, gingival health, plaque accumulation, and aesthetics, with no secondary caries reported in ZC groups in most studies. A small but consistent concern was opposing enamel wear associated with ZC. Nevertheless, considerations such as cost, preparation requirements, and follow-up duration remain important factors in clinical decision-making.
Strengths, limitations, clinical implications, and future perspectives
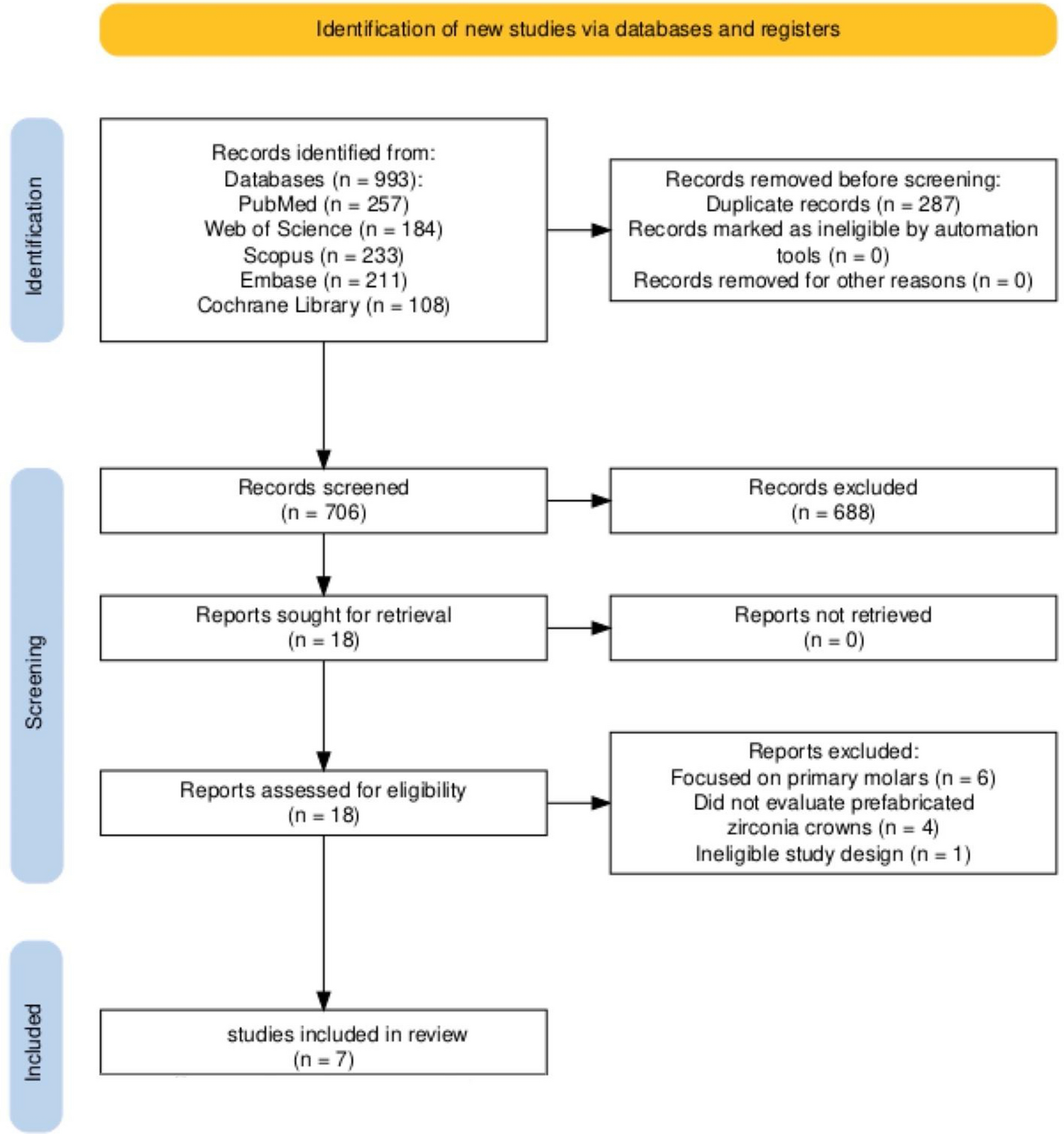
This systematic review possesses several notable strengths that enhance the validity and relevance of its findings. It is focussed exclusively on RCTs with a minimum follow-up of 3 months, thereby ensuring a high level of evidence and minimising the risk of selection and performance biases inherent in observational studies. Moreover, the review was conducted in accordance with PRISMA guidelines and registered prospectively, which promotes methodological transparency and reproducibility (Supplementary file 4). However, several limitations in the current body of evidence must be acknowledged. First, although all studies were RCTs, many were rated as having “some concerns” in at least one domain of the RoB2 tool, particularly due to insufficient reporting of allocation concealment and the inability to blind operators or outcome assessors. Second, heterogeneity existed across studies in terms of comparator crown types, evaluation criteria, and outcome measurement tools. For example, some trials used subjective parental satisfaction surveys or non-standardised visual scoring (Ravada et al. 2022; Vaghela et al. 2021), whilst others employed more objective indices such as USPHS criteria or Silness and Löe plaque and gingival indices (Alaki et al. 2020; Gill et al. 2020; Özdemir et al. 2022). Third, most studies included only healthy, cooperative children treated in university settings, potentially limiting the generalisability of findings to broader paediatric populations, including those with behavioural challenges or systemic health conditions. Additionally, the review was restricted to studies published in English, which may have introduced language bias and led to the exclusion of relevant trials published in other languages, whilst the omission of grey literature raises the possibility of publication bias. Finally, due to heterogeneity in outcome definitions, follow-up durations, and comparator groups, a meta-analysis could not be performed, limiting the ability to generate pooled effect estimates.
The results of this systematic review have several important implications for clinical practice and future research. From a clinical standpoint, prefabricated ZCs demonstrate consistently superior performance to traditional full-coverage restorations, particularly in terms of crown retention, gingival health, aesthetics, and caregiver satisfaction. These findings support the routine use of ZCs in paediatric dental settings, especially for patients and families with high aesthetic expectations. However, the decision to use ZCs must also take into account potential trade-offs, such as increased cost, the need for greater tooth reduction, and the possibility of enamel wear on opposing teeth. Future research should aim to address existing gaps in the evidence. Longitudinal studies with extended follow-up periods are needed to assess long-term crown survival, impact on occlusion, and wear on opposing dentition. Additionally, standardisation of outcome measures, use of validated satisfaction scales, and inclusion of broader paediatric populations, such as uncooperative children or those with special healthcare needs, will enhance the external validity and generalisability of findings.

Comments (0)