
Remember me
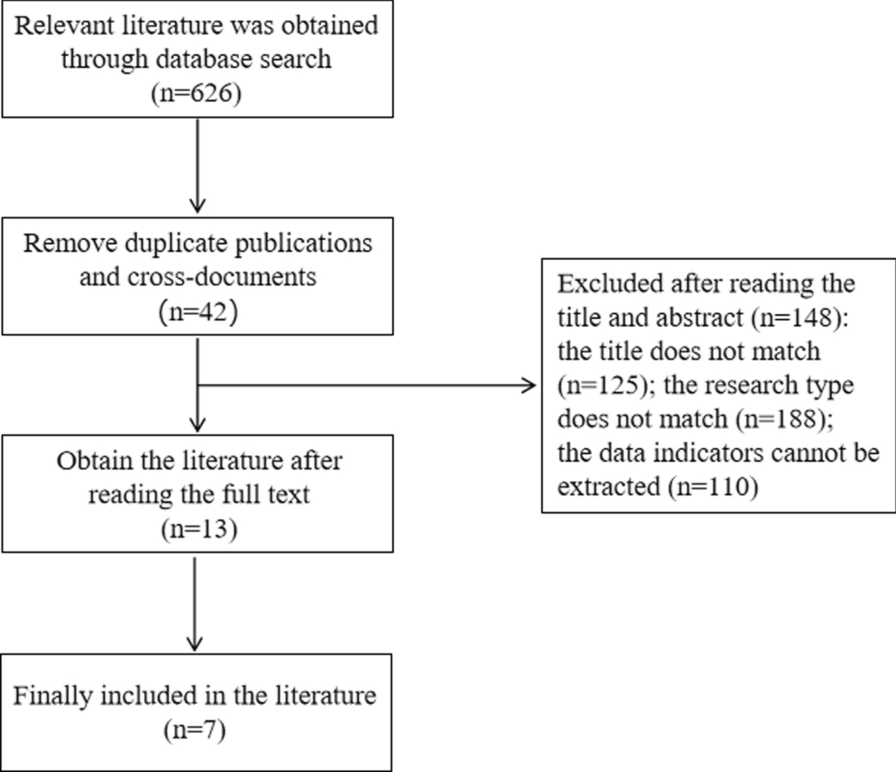
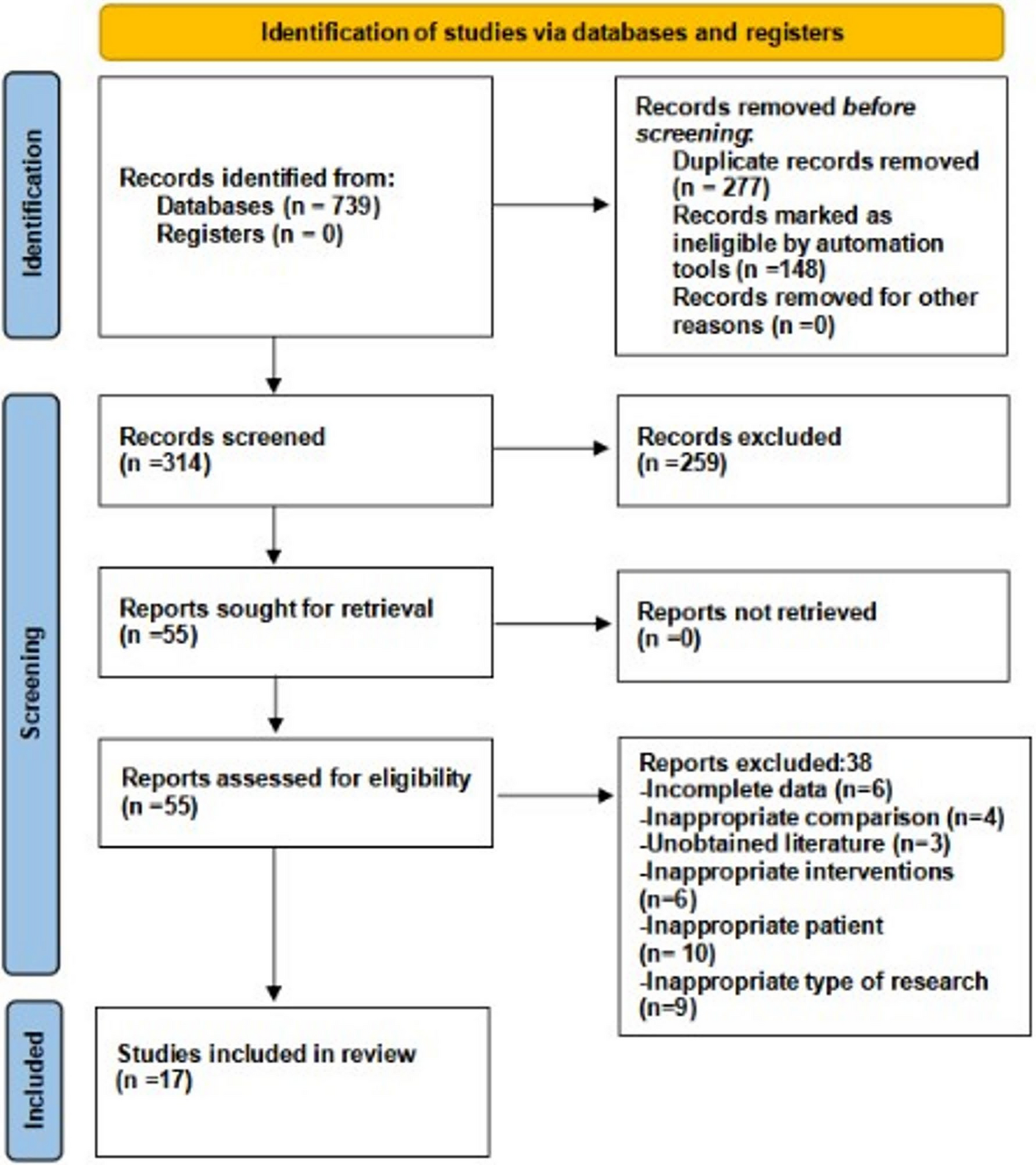





Initially, 739 articles in total were obtained using the search strategy, 277 of which were excluded after removing duplicates, and 55 were obtained by reading the titles and abstracts in strict accordance with the inclusion and exclusion criteria. Finally, through reading the full text, 38 more studies were excluded (Supplementary Material S3) and 9 studies were included. Fig. 1 depicts the literature screening procedure.
Fig. 1
The Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) flow diagram to show study selection
Study characteristicsIn all, 17 articles were incorporated into this meta-analysis, all of which were published after 2019. A total of seven case series studies [19,20,21,22,23,24,25], nine cohort studies [26,27,28,29,30,31,32,33,34], and one RCT [35] were included. Table 1 presents basic information about all the included studies. The sample size for all included studies exceeded 30 cases; 14 studies utilized fiber tape as the suture material, 1 study employed high resistance suture [24], 1 study used ultra-high molecular weight polyethylene/polyester suture tape [32], and 1 study utilized ultrahigh-strength tape [31]. Across all included studies, there were a total of 833 male and 588 female participants. The follow-up duration for all studies was equal to or greater than 2 years. A total of 4 studies focused on people younger than 23 years old [25, 27, 29, 30], while the remaining 13 studies included participants aged over 24 years. In total, ten studies provided the body mass index (BMI) range of the participants [19, 23,24,25,26, 28,29,30, 32, 33]. In addition, we separately summarized the conclusions of the included studies (Supplementary Material S4). All studies included in this meta-analysis had NOS scores between 8 and 9. (Supplementary Material S5).
Table 1 Baseline characteristics of included literatureResults of meta-analysisLysholm Knee Scoring ScaleIn total, 5 studies involving 328 participants reported the effect of SA on Lysholm Knee Scoring Scale [26, 27, 31, 32, 34]. The analysis was done using the fixed-effects model and revealed no discernible differences within the SA and non-SA groups (mean difference, MD = 0.21, 95% confidence intervals, 95%CI −1.05, 1.48, P = 0.74, I2 = 44%) (Fig. 2).
Fig. 2
Forest plots of Lysholm Knee Scoring Scale
IKDCThe pre–post meta-analysis contained two studies with 200 patients [23, 25]. The random-effects model was used to analyze the effects before and after operation, and the results of mete analysis demonstrated a substantial relationship between SA and the improvement of IKDC (MD = −48.31, 95%CI: −54.10, −42.51, P < 0.001, I2 = 51%) (Supplementary Material S6). Additionally, four studies involving 377 participants reported the effect of SA on IKDC [26, 28, 32, 33]. The random-effects model was used to analyze this, and it revealed no discernible differences within the SA and non-SA groups (MD = 5.80, 95%CI −0.40, 11.99, P = 0.07, I2 = 86%) (Fig. 3).
Fig. 3 KOOS
KOOSThe pre–post meta-analysis contained three studies with 218 patients [20, 21, 28]. The random-effects model was used to analyze the effects before and after operation, and the results of the meta-analysis demonstrated a substantial relationship between SA and the improvement of KOOS (MD = −38.31, 95%CI −46.13, −30.49, P < 0.001, I2 = 87%) (Supplementary Material S6).
The effect of SA on VAS for pain.The pre–post meta-analysis contained three studies with 208 patients [20, 21, 25]. The random-effects model was used to analyze the effects before and after operation, and the results of meta-analysis demonstrated a substantial relationship between SA and the improvement of VAS (MD = 1.64, 95%CI 1.06, 2.21, P < 0.001, I2 = 70%) (Supplementary Material S6). In addition, four studies involving 447 patients reported the effect of SA on VAS for pain [27, 29, 30, 35]. A fixed-effects model was used to analyze this and revealed that VAS for pain was significantly reduced in the SA group compared with the control group (MD = −0.17, 95%CI −0.32, −0.02, P = 0.02, I2 = 0%) (Fig. 4).
Fig. 4
Forest plots of VAS for pain
VR-12 physicalThe pre–post meta-analysis contained three studies with 208 patients [20, 21, 25]. The random-effects model was used to analyze the effects before and after operation, and the results of the meta-analysis demonstrated a substantial relationship between SA and the improvement of VR-12 physical (MD = −17.49, 95%CI −22.07, −12.90, P < 0.001, I2 = 85%) (Supplementary Material S6). In addition, two studies involving 262 patients reported the effect of SA on VR-12 physical [30, 35]. A fixed-effects model was used for analysis and no significant difference was found between the SA group and the control group (MD = −0.51, 95%CI −0.94, 1.97, P = 0.49, I2 = 21%) (Fig. 5).
Fig. 5
Forest plots of VR-12 physical
Marx activity scaleThe pre–post meta-analysis contained three studies with 208 patients [20, 21, 25]. The fixed-effects model was used to analyze the effects before and after operation, and the results of the meta-analysis demonstrated a substantial relationship between SA and the improvement of Marx Activity Scale (MD = 4.04, 95%CI 3.69, 4.38, P < 0.001, I2 = 0%) (Supplementary Material S6). In addition, two studies involving 262 patients reported the effect of SA on the Marx Activity Scale [30, 35]. A fixed-effects model was used to analyze this and revealed no significant difference between the SA group and the non-SA group (MD = 0.87, 95%CI −0.36, 2.10, P = 0.16, I2 = 0%) (Fig. 6).
Fig. 6
Forest plots of Marx Activity Scale
SANEA total of four studies involving 307 participants reported the effect of SA on SANE [26, 28]. The analysis, using a fixed-effects model, differed significantly within the SA and non-SA groups (MD = 3.26, 95%CI 0.77, 5.76, P = 0.01, I2 = 13%) (Fig. 7). In terms of SANE scores, the SA group performed noticeably better than the group without SA.
Fig. 7 Tegner Activity Score
Tegner Activity ScoreIn total, three studies involving 293 participants reported the effect of SA on Tegner Activity Score [26, 27, 29]. The analysis using a random-effects model showed that there was no significant difference in Tegner Activity Score between the SA group and non-SA group (MD = 0.52, 95%CI −0.18, 1.22, P = 0.14, I2 = 65%) (Fig. 8).
Fig. 8
Forest plots of Tegner Activity Score
KT-1000 anteroposterior knee laxityA total of two studies involving 227 patients reported the effect of SA on KT-1000 anteroposterior knee laxity [29, 30]. The fixed-effects model was used to analyze this and revealed that the anteroposterior knee laxity of KT-1000 of the non-SA group was significantly better than that of the SA group (MD = 0.31, 95%CI 0.03, 0.59, P = 0.03, I2 = 0%) (Fig. 9).
Fig. 9
Forest plots of KT-1000 anteroposterior knee laxity
Return-to-sports rateA total of three studies involving 294 patients reported the effect of SA on the RTS rate [26, 27, 29]. The fixed-effects model was used to analyze this and revealed that there was no significant difference between the SA group and the non-SA group in improving the RTS rate (MD = 1.07, 95%CI 0.96, 1.19, P = 0.22, I2 = 16%) (Fig. 10).
Fig. 10
Forest plots of return-to-sports rate
Comments (0)