Osteoarthritis is a chronic musculoskeletal disease that often occurs in people’s daily lives. The knee joint is one of the main areas where osteoarthritis occurs. It is generally caused by knee joint degeneration, trauma, strain and other factors, and the degradation of knee joint cartilage tissue. Clinically, its main pathological features include narrowing of the knee joint space, osteophytes, and sclerosis. The prevalence increases sharply with age. It is most common in middle-aged and elderly people who are obese or exercise a lot. They will experience joint pain and obvious swelling when walking and daily life. If not treated in time, it may even cause deformity and even disability. Currently, TKA is clinically the main treatment for end-stage knee osteoarthritis, and most patients who undergo knee arthroscopy require TKA later.
This meta-analysis commented on the influence of knee arthroscopy on the efficacy of subsequent TKA. The results reflected that previous knee arthroscopy increased the knee stiffness rate, periprosthetic infection rate, revision rate, and reoperation rate after TKA. There was no statistically significant difference in postoperative knee flexion range of motion and VTE incidence between the two groups. Periprosthetic infection is a common complication after TKA. This meta-analysis found that arthroscopic surgery can increase the rate of periprosthetic infection after TKA. The possible reason is that joint effusion and hematoma after arthroscopy will increase the risk of incision infection; joint capsule injury, the uncertainty of operation time, and postoperative injection of drugs into the joint cavity all increase the risk of potentially pathogenic bacteria entering the joint cavity, thereby increasing the infection rate after TKA [30]. Postoperative joint stiffness is another common complication after TKA. This meta-analysis found that knee arthroscopy increases the rate of postoperative stiffness after TKA. The possible reasons are that the perfusion fluid replaces joint synovial fluid during arthroscopic surgery, and that postoperative bleeding, hematoma, effusion, and synovial inflammatory reaction increase the level of fibrous tissue in the joint cavity, synovial thickening [3, 12], and tissue adhesion. In addition, patients who are afraid of activities owing to pain after surgery, do not pay attention to rehabilitation, and do not cooperate may limit the range of activities before surgery and increase the risk of joint stiffness after TKA.
On the basis of the comparative results of periprosthetic infection rates, we compared the reoperation rate revision rate and revision rate after TKA and found that knee arthroscopy increased the reoperation rate revision rate and revision rate after TKA. The possible reason is that the osmotic pressure of arthroscopy perfusion fluid will affect the metabolism of knee joint tissue, destroy the cartilage structure [26], and expose the subchondral bone, thereby stimulating an autoimmune response and causing osteolysis. In addition, arthroscopic surgery affects bone cement penetration during TKA, causing an increase in fibrous tissue and thickening of the synovial membrane at the postoperative bone-cement interface [28]. This leads to a reduction in the structural holding force between bone cement and trabecular bone, thereby affecting the stability of the prosthesis [22], thus increasing the revision rate and reoperation rate after TKA. This is also consistent with the findings of Marsh et al. [23], who identified prior arthroscopic procedures as a significant positive predictor of TKA revision. In addition, the study by Hernigou et al. [24] demonstrated that patients over the age of 70 years who underwent arthroscopic partial meniscectomy had a higher risk of eventually requiring TKA.
This study found that there was no statistically significant difference in postoperative knee flexion range of motion and VTE incidence between the two groups. Postoperative knee flexion range of motion is strongly influenced by the quality of postoperative rehabilitation. Active participation and adherence to rehabilitation protocols are essential for restoring knee joint mobility. However, the routine use of tourniquets during arthroscopy, aimed at improving surgical visualization, prolongs venous stasis and may subsequently elevate the risk of VTE. As a major orthopedic surgery, TKA causes blood flow stasis, vessel wall damage, and blood hypercoagulability, which are also important risk factors for VTE [20]. Therefore, orthopedic surgeons should standardize the use of tourniquets during surgery, operate them gently and carefully to avoid venous damage, and provide appropriate fluid replenishment during and after surgery to reduce blood viscosity and prevent the occurrence of postoperative VTE.
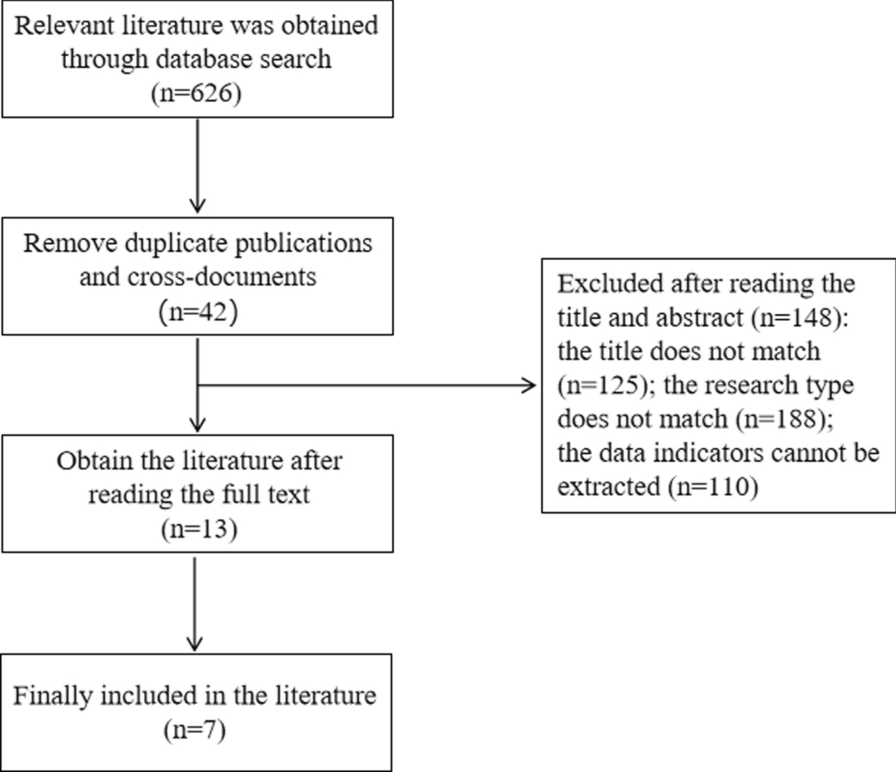
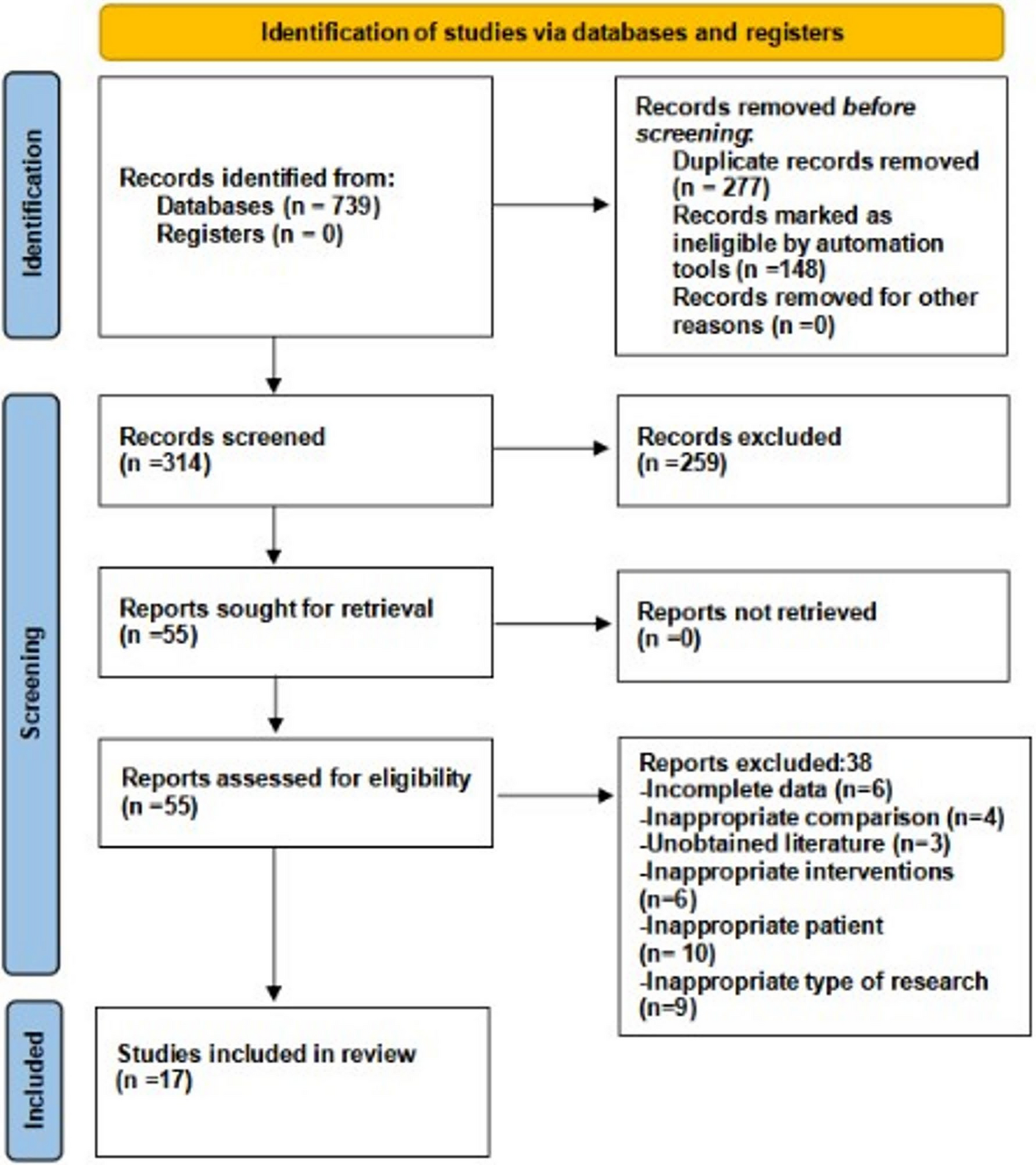
This study used established search strategies and strictly screened literature according to exclusion and inclusion criteria to compare the influence of knee arthroscopy on subsequent TKA. Arthroscopic surgery and TKA are relatively mature in clinical operations, and the outcome indicators involved in this article are of high clinical concern. Therefore, the conclusions drawn in this study through meta-analysis have practical clinical significance. However, the variety of knee arthroscopy surgery methods, knee prostheses, and differences in the interval between two surgeries may affect the authenticity of this study to a certain extent.
At present, the concepts of stepped treatment and personalized treatment of KOA are popular in clinical practice. As a treatment for end-stage KOA, the prognosis of TKA is tightly related to the patient’s quality of life and knee joint function. Therefore, it is crucial to study the influence of knee arthroscopy on the efficacy of TKA. This meta-analysis found that arthroscopic surgery can increase the revision rate, reoperation rate, periprosthetic infection rate, and postoperative stiffness rate after subsequent TKA. Before patients undergo TKA, nonsurgical treatment of KOA may be more effective. However, the diagnostic value of arthroscopy should not be ignored in patients who fail conservative treatment and whose imaging cannot provide sufficient evidence of TKA [1].
However, some studies have suggested that knee arthroscopy may not significantly delay or accelerate the implementation of TKA. A secondary analysis of a randomized clinical trial indicated that, among patients with KOA undergoing either knee arthroscopy combined with nonoperative treatment or nonoperative treatment alone, there was no statistically significant association between knee arthroscopy and the timing of TKA. Moreover, compared with nonoperative treatment, knee arthroscopy did not significantly alter the cumulative incidence of TKA [33]. Similarly, a retrospective study found that prior medial meniscus arthroscopy appeared to have no negative impact on the rates of all-cause reoperation, revision, or complications following TKA [34]. These findings seem to contradict our results, and such discrepancies may arise from differences in study design, sample characteristics, and follow-up durations. Our study, employing a meta-analytic approach, incorporated multiple high-quality studies, resulting in a larger sample size and stronger statistical power. Nonetheless, the impact of knee arthroscopy on the implementation of TKA warrants further investigation.
In summary, knee arthroscopy has a negative influence on consecutive TKA. Knee arthroscopic operation increased the risk of revision, reoperation, postoperative stiffness, and periprosthetic infection after TKA, but there was no important difference in postoperative knee flexion range of motion and postoperative VTE rate. Further research with higher and more rigorous evidence levels is needed to demonstrate this in the future.






Comments (0)