This study aimed to explore the effects of surgical timing on mortality and complications in older adults with hip fractures. Our main findings reveal that early surgery, performed within 24 h, is associated with a significantly lower mortality rate compared with surgery performed after 24 h (2.8% versus 5.2%, p = 0.046). However, we also found that acute infections and sepsis, regardless of the timing of surgery, are linked to increased mortality rates, suggesting that in these cases, prompt surgical intervention may be more beneficial than waiting for clinical stabilization.
Hip fractures are severe injuries that can result in postoperative complications, disability, lifelong immobility, and death, particularly in older adults [4, 36, 37]. Age, gender, comorbidities, anticoagulant medication, general health status, and the timing of surgery are all known factors that impact the survival of these patients. The relationship between the timing of surgery and postoperative outcomes has been widely studied and is known to influence the clinical outcomes and survival of patients suffering from hip fractures.
Although international clinical practice guidelines recommend surgical treatment of acute hip fractures within 48 h to prevent the occurrence of postoperative complications [26], in clinical practice, delay of surgery of hip fractures is common [4]. Most delays are caused by a patient’s comorbidities and acute events occurring at arrival in the emergency room, which increases surgical risk and perioperative complications, such as pneumonia, deep venous thrombosis, hemorrhage, pulmonary embolism, urinary tract infections, and decubital ulcerations [4].
Generally, clinicians take time to optimize patients’ medical conditions before surgery, even though some studies show that early surgery is connected to a shorter length of stay, less discomfort, a decrease in significant complications, and a drop in death rates for patients. [26, 38].
The timing–outcome relationship has been previously demonstrated in many studies: early surgery is beneficial in clinical outcomes and patient survival [27]. For example, Maheshwari et al. [27] illustrated a linear relationship between the delay in surgery and mortality. With every 10-h increase in time from hospital admission to surgery, there is an estimated 5% increase in odds of 1-year mortality. In our results, the mortality rate in patients that we treated within 24 h was 2.8%, and for those who underwent surgery after 24 h, the mortality was 5.2% (p = 0.046; OR 1.58), corresponding with findings from literature. There are numerous studies in literature with medium and long-term follow-ups that show a significant increase in the risk of mortality related to surgical timing [39,40,41].
According to epidemiological statistics from Pinto et al., older individuals with proximal femoral fractures have a 1-year death rate ranging from 14% to 20% [41], with some studies reporting an even higher rate of 40% [42].
This worrying fatality rate stresses the importance of identifying risk factors for death following surgery: age, gender, preoperative functional capability, preexisting comorbidities, and general health status [43]. While there has been extensive research on mortality predictors, there is limited exploration of risk prediction models and preventable risk factors. As mentioned, numerous studies agree that receiving surgical treatment as an urgent procedure, once the body meets the basic anesthetic requirements, is beneficial for older adults [44, 45], and lots of orthopedic societies such as the American Academy of Orthopedic Surgeons (AAOS) recommend surgical repair within 48 h of admission [45].
These findings emphasize the critical implications and potential complications associated with hip fractures in older adults, highlighting the significance of early and appropriate medical care to improve outcomes and reduce mortality risk. Unfortunately, mechanisms for how early surgery decreases mortality are still unclear, and the reasons for this association remain unanswered. According to Maheshwari et al., the prolonged inflammatory response in delayed surgery can lead to an increased risk of infection, delirium, and cardiovascular complications, which increase mortality risk. [27]. In 2017, Daniel Pincus conducted a study that included 42,230 patients with a mean age of 80.1 years treated surgically for hip fracture. The study showed that patients who postpone the operation by 24 h suffered complications such as pneumonia (p = 0.002), pulmonary embolism (p < 0.001), and myocardial infarction (p < 0.001) more frequently when compared with those whose waiting time before surgery was less than 24 h [46].
Furthermore, Dong et al. [26] performed a comprehensive review in 2011 including 15 studies, which showed that the occurrence of postoperative complications was influenced by the waiting time: patients who took more than 48 h to undergo surgery experienced severe postoperative complications and suffered not only pneumonia, pulmonary embolism, and myocardial infarction but also sepsis (p = 0.008) and cardiac arrest (p = 0.039) when compared with patients treated within 48 h (p = 0.010; p = 0.043) [26].
The most frequent postoperative complications described are confusion, urinary tract infection, and pneumonia (especially in people affected by pulmonary diseases) [21, 47]. In addition, surgical-site infections that require reoperation are of significant complication owing to the severity and complexity of treatment, and, probably, the association between poor wound healing and infection underlies a biological mechanism related to preexisting morbidities such as diabetes [21]. Indeed, comorbidities are important risk factors not only for surgical problems but also for postoperative complications, affecting patient outcomes; they are connected to infection up to 1 year after surgery [21].
In the study of Gadgaard et al., within 1 year after surgery, the cumulative incidence of any hospital-treated infection was 22.2% among patients with no comorbidity, 29.8% among patients with moderate comorbidity, and 36.6% among patients with severe comorbidity, showing that the cumulative incidence of any hospital-treated infection increased with increasing comorbidity level [21]. Our study results reveal a different aspect of this picture: acute infections and sepsis are related to increasing mortality rates in both patients treated surgically within 24 h and after 24 h, without significant differences. It suggests that treating patients with acute infections and sepsis surgically does not change the outcome in relation to surgery timing. In such cases, waiting for their full clinical recovery and reconditioning does not improve the postsurgical survival rate.
Furthermore, delaying surgery in the hope of clinical recovery and reconditioning might not yield better outcomes, as the ongoing presence of an acute infection or sepsis can lead to further deterioration of the patient’s condition. Instead, a timely surgical approach appears to be a good way of managing these high-risk patients effectively.
Our findings suggest that infections not only elevate mortality rates in individuals with significant comorbidities who are most susceptible but also impact patients in generally healthier conditions (OR 5.992). According to our results, the correlation between the Charlson Comorbidity Index (CCI) and mortality was not statistically significant (p = 0.62). Unlike the findings in literature, our results indicate that the CCI did not have a significant impact on mortality because it pertains to chronic diseases and comorbidities rather than the acute conditions that can coexist with fractures.
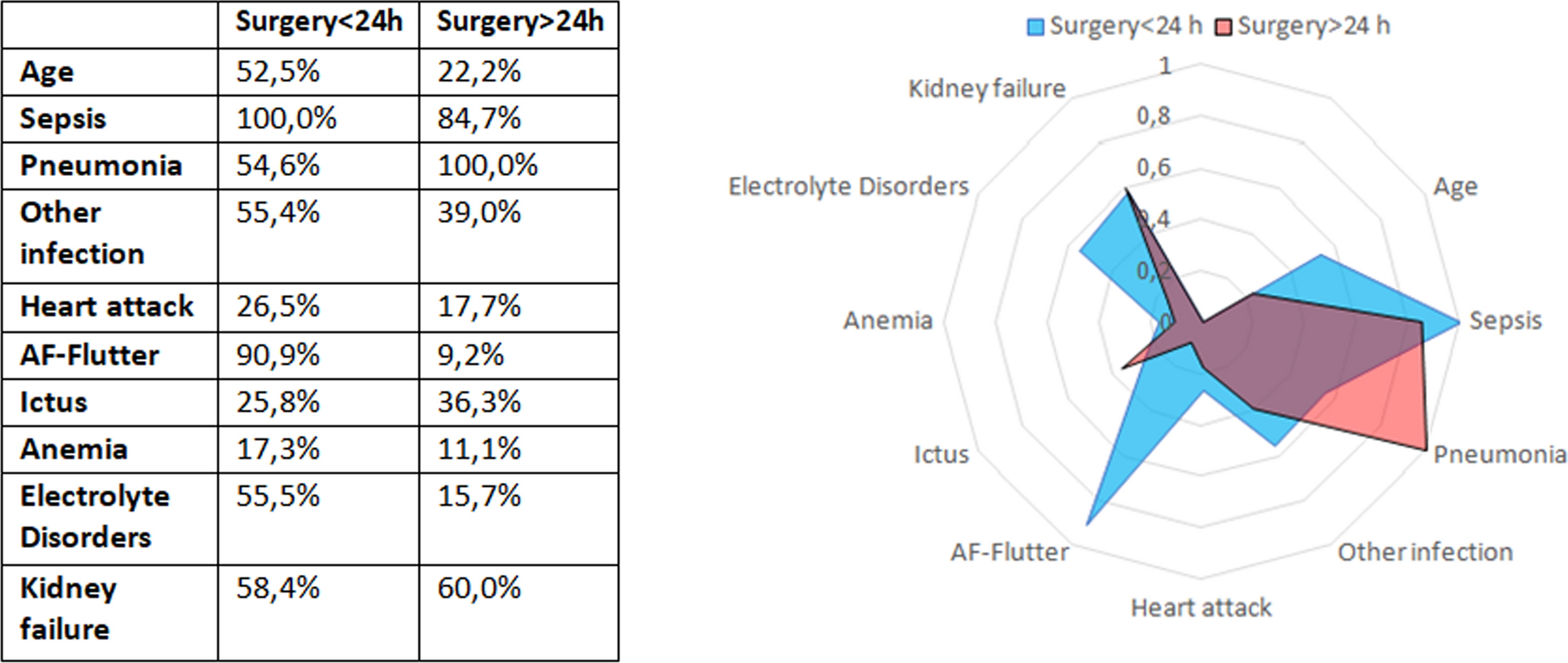
Conversely, acute events such as atrial fibrillation, flutter, and electrolyte depletion appear to destabilize patients’ conditions and seem to have a greater impact on their outcomes. In our study, neural network analysis revealed that sepsis (10%), acute infections (55.4%), electrolyte imbalances (55%), and atrial fibrillation and flutter (90%) had the greatest relative significance regarding the risk of mortality in patients treated within the initial 24 h.
Indeed, acute events were related to increased mortality risk, particularly in patients treated within 24 h. This observation suggests that the urgency of treating acute events necessitates immediate medical intervention to stabilize the patient before surgery. Stabilization is crucial to minimize intraoperative and postoperative complications, which can otherwise exacerbate the patient’s condition and increase the likelihood of mortality.
NHFS is a risk assessment system designed exclusively for patients with hip fracture. It determines the preoperative mortality risk within 30 days of a hip fracture and is also related to postoperative mobility and hospitalization rate [13]. NHFS association with mortality, similar to CCI, was not statistically significant, most likely for the same reasons we discussed above.
Our study did not extensively explore comorbidity as a risk factor for post-hip fracture surgery infections. Additionally, our focus was not on a specific type of infection, as it was not the primary endpoint of our study. Furthermore, rehabilitation, complications, and pharmacologic treatments after hospital discharge were not collected.
Study limitations
Several limitations must be acknowledged in this study. First, the retrospective design introduces potential biases, including selection bias and information bias, as data were extracted from existing medical records. This approach limits our ability to control for all potential confounders and restricts the ability to establish causal relationships. Second, the study focused on a limited number of perioperative complications such as surgical timing, in-hospital mortality, and a few complications, excluding other potentially influential factors such as postoperative rehabilitation, long-term functional outcomes, or specific comorbidities. These additional factors could have significantly impacted the results but were beyond the scope of this study.
Moreover, the sample population consisted primarily of older adults, which may limit the generalizability of our findings to younger individuals or those with different clinical characteristics. The variability in patient management protocols across the study sites also introduces another limitation. Inconsistent preoperative, intraoperative, and postoperative care across sites was not accounted for and could have influenced the outcomes.
Additionally, data on post-discharge outcomes, including long-term rehabilitation, functional recovery, or quality of life, were not collected. These factors are crucial for evaluating the comprehensive impact of surgical timing on patient health and recovery. Finally, although efforts were made to control for known variables, other unmeasured confounders, such as the type of surgical procedure or anesthesia used, may have influenced the results. Future studies with a prospective design, larger sample sizes, and more detailed data collection would help address these limitations and provide a deeper understanding of the relationship between surgical timing and patient outcomes in hip fracture surgeries.






Comments (0)