
Remember me

We used clinical data from a prospective cohort study, Cambridge Translational Cancer Research Ovarian Study 04 [14] (CTCR-OV04), designed to investigate the mechanisms of treatment response in ovarian cancer. We obtained access to individual data from 597 women in this cohort with histologically confirmed HGSOC, enroled between September 2010 and September 2022. The patients, aged 66.9 ± 10.6 years were predominantly white (98.3%) with stage III/IV disease (85.6%) (Table 1).
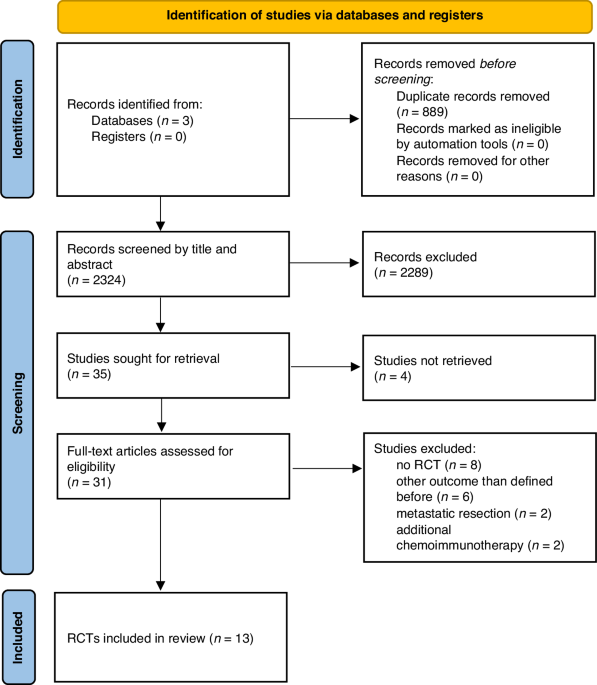
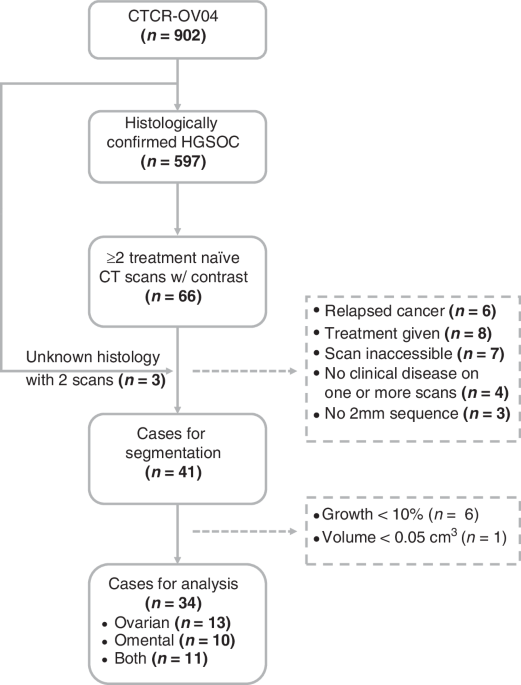
Table 1 Characteristics of all 597 HGSOC patients and the 34 patients with a growing lesion in either the ovaries/pelvis or the omentum.Sixty-six patients had multiple CT scans with contrast before treatment, making them suitable for modelling tumour growth kinetics. We included three more patients with multiple CT scans who had no confirmed histotype, resulting in a total of sixty-nine candidates for analysis. The reasons for multiple scans before treatment included re-staging to assess the extent of metastatic disease following a delay in the commencement of chemotherapy, confirmation of a suspicious lesion, or new symptoms that could be due to unobserved lesions in the first scan. We only considered those cases with at least two scans taken with contrast at a 2 mm slice thickness and clinically observed primary disease on both scans; forty-one cases satisfied these criteria (Fig. 1).
Fig. 1: Consort diagram showing the cases for volumetric analysis.
There were 34 cases that had two or more scans with clinically observed disease >0.05 cm3 and at least 10% growth in either the pelvis/ovaries or the omentum. Excluded cases are shown in the dashed boxes.
We used CT scans to evaluate the growth kinetics of HGSOC as they contain information on disease burden in multiple sites; this enabled us to estimate the time interval between the initiation of lesions in different sites.
Scan segmentationWe applied a deep-learning algorithm called ovseg [15] on the CT scans to automatically segment lesions in the ovaries/pelvis and the omentum. Ovseg is a state-of-the-art segmentation framework that was designed and finetuned to segment lesions in HGSOC. It demonstrated performance comparable to a junior radiologist and achieved a Dice similarity coefficient of up to 71 +/− 12 for ovarian/pelvic lesions and 61 +/− 24 for omental lesions on external test data.
Although ovseg was trained on images acquired at a slice thickness of 5 mm, we used scans acquired at intervals of 2 mm as this provided a higher resolution and also expanded the number of suitable cases. Given this change in resolution, we revalidated the method by comparing the volumes obtained using the two slice thicknesses for 38 scans that had both resolutions available and a volume of at least 0.05 cm3.
Volume calculationWe calculated the total tumour burden in each disease site from the binary segmentation mask outputted by ovseg using:
$$_/}=\mathop\limits_^_}_^/}\cdot $$
Where \(_\) is the total number of voxels in the scan sequence, \(_\) is 1 if the voxel is part of a lesion and 0 otherwise, and \(\) is the volume of a voxel.
Doubling time calculationWe considered cases for doubling time calculations if they had at least 10% increase in volume between successive scans, and a minimum burden of 0.05 cm3 in either disease site; these requirements mitigated the chances of the results being skewed by artefacts.
We calculated the doubling time (TVDT) assuming an exponential growth model which provides the simplest way to capture the growth rate from two volume measurements.
$$\frac\frac}}=\alpha ;\alpha =\frac}}_/_$$
(1)
where α is the specific growth rate of the tumour, and V2 and V1 are the tumour volumes measured at a time interval of dt.
Gompertz model of tumour growthWe sought a model that could best estimate the time of initiation of the lesions at each disease site (ovarian or omental) from the available volumetric data. The constant growth rate assumption of the exponential model (Eq. (1)) makes it unsuitable for this task as tumour growth has been shown to decrease with size until it becomes almost negligible at extremely large volumes [16,17,18]. Instead, we used a Gompertz model as it has been found to better mimic preclinical [18,19,20] and clinical [21] tumour growth patterns rate (Eq. (3)).
$$V\left(t\right)= \,\,_\cdot \exp \left[K\left(1-^\right)\right] \\ \frac\frac}} = \,\,\beta K^$$
(3)
V0 is the initial volume, assumed to be a single cell (10−9 cm3), β is the decay constant, and \(K=\mathrm\frac_}_}\), where \(_\) is the carrying capacity of the tumour. We set \(_\) based on the maximal ovarian and omental volumes in our dataset.
The OV04 data consisted of two volume measurements, \((_,\,_)\) along with the time interval, \(\Delta t=_-_\), between the two scans. The time interval, \(_\), between initiation of the specific lesion and the first scan is unknown and thus needed to be estimated along with β (Eq. (4)).
$$V(\Delta t)=_\cdot \exp \left[K\left(1-^_+\Delta t\right)}\right)\right]$$
(4)
Here, the volume V is a function of the time interval Δt.
Population modellingWe used a nonlinear mixed effects model (NLME) to fit the data and estimate the time between tumour initiation and the first volume measurement in the two disease sites; this population approach to modelling enabled us to estimate the overall trend in growth kinetics while also accounting for inter-subject variability.
NLME assumes that all individuals belong to a single population, and that their individual model parameters, \(}}^}}\), are distributed normally around the population average, \(}}^}}\), with a variance matrix D (Eq. (6)). The observation, \(_^\), of individual i at time \(_^\); is a function of \(}}^}}\) with an added error term, \(_^\), that follows a standard normal distribution and is scaled by λ (Eq. (5)).
$$_^=f\left(_^;}}^}}\right)+_^$$
(5)
$$}}^}}= \,\, }}^}}+N(0,\,})\\ _^= \,\, N(0,1)$$
(6)
Normally, \(_^\) and \(f(_^;}}^}})\) would represent the measured lesion volumes and the expression for Gompertzian growth (Eq. (4)), respectively. However, we reformulated the expressions for \(_^\) and \(f(_^;}}^}})\) to facilitate convergence and used log-transformed parameters to ensure strictly positive values for β and t1. (Eq. (7)).
$$_^= -}\left(1-\frac}\frac_}^}}_}\right)\\ f(_^;}}^}})= \,\, ^\beta _\right)}^}+^\beta \right)}^}\Delta _^$$
(7)
Here, \(}}^}}=\ \, \beta \right)}^,\, \, \beta _\right)}^\}\), while f is a function of the time interval \(\Delta _^\). The first observation at \(_^\) for each patient corresponds to \(\Delta _^=0\). We estimated the parameters (\(}}^}},},\) and λ) by maximising a linearised approximation of the log likelihood [22] using the nlmefit package implemented in Matlab 2024 [23].
The NLME algorithm provides us with the fixed effects estimates of the log transformed parameters \(\beta \right)}^}\) and \(\beta _\right)}^}\); however, the variable of interest is the time since initiation of the ovarian or omental lesions, \(_\). We calculated the population level \(_^}\) using the formula, \(_^}=^\beta _\right)}^}-\beta \right)}^}}\). We then estimated the 95% CI of \(_^}\) from the standard errors of the transformed variables (Supplementary Note 1).
We compared the value of \(_^}\) estimated using Gompertzian growth against those from an NLME with exponential growth (Eq. (8)) where \(}}^}}=} \, \alpha \right)^,}\left(\alpha _\right)^\}}\).
$$_^ = \,\, }\frac_}^}}_} \\ f\left(_}^;}}^}}\right) = \,\, ^} \,_\right)}^}+^} \,\right)}^}\Delta _^}$$
(8)
Estimating the window-of-opportunity for screening in the OV04 datasetWe used the individual parameter estimates, \(}}^}},\) to calculate the \(_^\) for each of the 11 cases with growing lesions in both disease sites and identify the window of opportunity (WOO) for early detection; this is the interval between the earliest possible screen detection and the onset of metastasis. We estimated the time to metastasis (Fig. 2), \(}=_^-_^\), given by the interval between the initiation of disease in the primary (p) and secondary (s) disease sites. The primary site was not always the ovaries/pelvis as four cases were estimated to have disease initiated in the omentum first; we retrospectively found that these were cases of peritoneal cancer which is also classified as HGSOC [24].
Fig. 2: Tumour volume doubling times (TVDT) in HGSOC.
TVDT a by tumour site (24 ovary/pelvis and 21 omentum) and b by tumour site and tumour volume at diagnosis - above (red) and below (blue) the median volume.
We then calculated the WOO for screening between the point at which the designated primary site reaches the US or CA125 detection thresholds of 0.5 cm3 and 0.015 cm3 respectively and the time of initiation of disease in the secondary site. These detection thresholds were informed by studies on the size distribution of image-detected tumours [25, 26] and a model-based estimate of the tumour burden at CA125 detection [27, 28]. Although we used CT scans for characterising the growth kinetics of the tumours in this study, we used the US detection threshold in our simulations as screening is most likely to be done by ultrasound.
Estimating the window-of-opportunity for screening in an in-silico populationWe simulated a virtual population of 10,000 patients to identify how many people could theoretically benefit from screening, and what the WOO would be in these individuals. For each case, we assigned the primary disease site with probabilities \(_}/_}\) and then sampled the Gompertz decay rate β from the corresponding distribution, while keeping \(_^/}\) fixed. We used a value of 0.36 for pom as 4 out of 11 cases in our cohort were expected to develop omental disease first; the results were agnostic to the choice of pom. Next, we sampled the size at which metastasis is seeded, Vmet, from the Gompertz estimate of the primary tumour at metastasis in the 11 patients with growing lesions in both sites. Finally, we calculated the time, tmet, taken for the primary tumour to reach \(_}\) and the WOO between the primary tumour reaching the CA125/US detection limits and tmet.
Comments (0)