We estimate that there is likely to be a small relative initial increase in demand for diagnostic testing if MCED screening were offered alongside current cancer screening programmes in the future. With a very large screening-eligible population and maximum theoretical uptake, a small percentage increase for each diagnostic modality could translate into a substantial increase in the absolute number of diagnostic procedures in the short term. Future reductions in diagnostic use from symptomatic presentations avoided due to detection by screening should moderate this impact in the longer term.
Activity is increasing year-on-year for most diagnostic modalities in our study under current standard-of-care practices in England [20,21,22]; as such, the estimated increase in diagnostic activity associated with MCED screening is small by comparison. For example, the maximum possible annual increases in demand for colonoscopy and gastroscopy in a steady-state scenario were predicted to be 2.99% and 1.83%, respectively, if all 18.9 million eligible people participated in MCED screening each year. This is in comparison to the estimated 6–7.5% annual increase in the number of endoscopy procedures between 2017 and 2019 [23]. The predicted annual 1% increase in demand for CT in the same maximum scenario is in comparison to a 6.8% increase in the annual number of CT scans between 2014/15 and 2018/19 [20]. The larger predicted increase in diagnostic demand after the initial introduction of a MCED screening programme (compared with the steady-state programme) is an expected short term impact driven partly by the underlying prevalence of undiagnosed cancer in the screening-eligible population. Endoscopy services in particular are under strain [20, 23, 24] and may come under further pressure from changes to current screening programmes, such as lowering the referral threshold for the faecal immunochemical test (FIT) [25]. Improvements to screening outlined in the NHS Long Term Plan [26], such as the rollout of targeted lung cancer screening, will also increase diagnostic activity, particularly the use of CT scans, in the short term [27]. However, as with MCED screening, the introduction of other screening approaches should reduce diagnostic activity related to symptomatic presentation in the longer term, as cancers are increasingly detected asymptomatically via screening.
The increase in diagnostic activity associated with MCED screening is predicted to persist, albeit to a lesser extent, in a long-term steady-state screening programme. If MCED screening were introduced in England in the future, more cancer types, including less common cancers for which single-cancer screening programmes are unlikely, would have the opportunity to be detected earlier, before symptoms appear. Once a screening programme has reached a steady state, the continued additional diagnostic activity will be largely driven by false positive test results. Even with a high PPV, some diagnostic activity, related to the investigation of people who are not diagnosed with cancer following diagnostic workup, will remain. Interestingly, recent real-world data on MCED test use in the US has shown that 9% of individuals with a CSD test result from an initial MCED test, but a negative initial confirmatory diagnostic test, went on to be diagnosed with cancer following a second MCED test within 10 months [28].
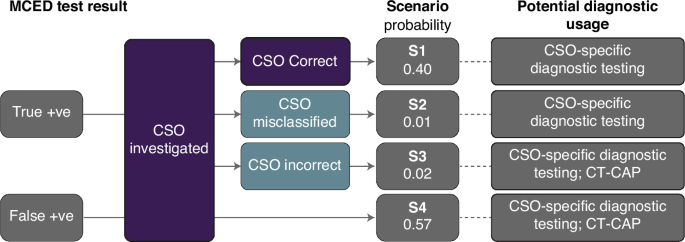
The benefits of MCED tests that predict a CSO (tissue type or organ) to streamline the diagnostic process have recently been explored. One modelling study predicted that a diagnostic workup based on a given CSO could result in a more efficient process than a non-directed workup, but also that continued investigation for cancers in locations other than the CSO is justifiable [29]. Both of these scenarios are incorporated into our model. A CSO-directed diagnostic process is also likely to be similar to the investigation of a patient presenting with site-specific symptoms of suspected cancer, and as such may be more easily incorporated into current clinical practice.
Our study focused on the initial diagnostic test(s) to confirm or rule out cancer following MCED screening. Our model did not include procedures related directly to the staging of cancers once detected, nor did it include activity to support treatment decisions, such as planning for surgery or radiotherapy. However, it is acknowledged that patients who are diagnosed with cancer (regardless of the route to diagnosis, whether through screening or symptomatic presentation) are likely to have a biopsy and/or imaging, in addition to the initial diagnostic tests. In our study, biopsy was the primary diagnostic investigation for cervical, skin, lymphoid and haemopoetic cancers, but adding biopsy as a secondary modality for all cancers detected by MCED screening would increase demand for histopathology even further in the short term. Assuming no overdiagnosis, all cancers detected by MCED screening would present symptomatically in the future, so with the exception of some activity for false positive CSDs, these biopsies are not additional in the longer term. We expect almost all to require biopsy regardless of route to diagnosis. Cancers diagnosed by initial ultrasound or CT may also require a second interventional radiology procedure.
The magnitude of change in activity estimated in our study varied by diagnostic modality, with the greatest proportional increases in activity for colonoscopy, gastroscopy, and biopsy. The modelled increases in colonoscopy and gastroscopy are due in part to the greater prevalence of and relatively high sensitivity of the MCED test for gastrointestinal cancers [10]. The comparator for the estimated increase in demand for biopsies with MCED screening was biopsies related to diagnosed cancer, whereas the comparator for other modalities was all activity irrespective of indication. Therefore, the comparative increase in biopsies (as a primary diagnostic investigation) with MCED screening is likely to be an overestimate compared with other modalities.
Diagnostic investigations for people who receive a CSD result may have other impacts on health services. The diagnostic process may coincidentally identify precursor or pre-invasive lesions (unrelated to the CSD result) or incidental findings that require further investigation [30]. Whilst adding to diagnostic activity, the discovery of precancerous lesions has potential benefits for both individuals and health services. For example, identification and removal of colorectal polyps can prevent bowel cancer, thus reducing requirements for cancer diagnosis and treatment in future. The potential impact of precancerous lesions and incidental findings on the health service, such as the requirement for surveillance, and their optimal management is not yet known; however, results from the NHS-Galleri trial will provide crucial insights on this. A small number of patients might also incur harm from diagnostic investigations [31] after MCED screening, especially if they undergo two or more diagnostic procedures. However, the overall impact of this is likely to be relatively small.
In the event of a CSD result for which the recommended diagnostic tests are carried out, but no cancer is found, the point at which clinicians should cease diagnostic investigation and return individuals to usual care has yet to be established [32]; this will also impact diagnostic activity and clinical workloads. Some clinicians may therefore offer repeat CTs for surveillance in patients in whom no cancer is found after CSD result. This could mean that our predictions for CT use are underestimated. Previous research showed that 31% of individuals with a CSD result on both an initial and a repeat MCED test are diagnosed with cancer within six months, while none of those with a ‘no CSD’ (i.e. negative) result on repeat test were diagnosed with cancer in the subsequent 16.7 months [28]. In practice, it may be more efficient to repeat an MCED test, as has become routine practice with the Galleri test in the US.
Careful planning to manage the capacity of diagnostic services, especially endoscopy, histopathology and imaging, would be required prior to introduction of any MCED screening programme in the future. Phased rollout of MCED screening, either geographically or by age, could provide the opportunity to test the assumptions made in this modelling (e.g., multiple diagnostic tests for false positives) and validate the predicted additional diagnostic activity. The NHS, government, and cancer and health charities have proposed specific approaches aiming to increase and upskill the diagnostic workforce, increase and upgrade diagnostic equipment, and re-organise diagnostic services to meet increasing demand [20, 33, 34]. The results of our modelling study could support workforce and resource planning for implementation of MCED screening and other screening innovations in the NHS.
We did not explicitly model any interplay between MCED screening and current cancer screening programmes, or make any assumptions about impact on uptake. Whilst MCED screening is not intended to be a replacement, there is likely to be some degree of overlap, in addition to the detection of cancers in individuals who fall outside the age- or risk-based eligibility criteria. It is not yet possible to quantify any potential overlap, nevertheless, the impact on diagnostic demand is likely to be minimal if similar diagnostic modalities are used to investigate ‘positive’ results.
Strengths and limitations
This study applied an evidence-based model to routine NHS data, using a range of input parameters from previous clinical and modelling studies. Input was sought from a wide range of clinicians to ensure the diagnostic approaches in the model reflected current practice for diagnosing suspected cancer and to validate the model results.
This model could be updated in future with sensitivity estimates for new or improved MCED tests, and revised assumptions based on evidence from MCED use in real-world settings and in large, randomised, controlled clinical trials such as the NHS-Galleri trial.
Some carefully considered decisions and assumptions were made in order for our model to function, given the lack of data on MCED screening in England. However, people with CSD test results may be investigated differently in a real-world clinical scenario.
Our study focused on the initial diagnostic test conducted following a CSD test result, accounting for the greater number of tests required when a cancer signal is detected but no cancer is subsequently diagnosed [10]. In practice, some individuals for whom a cancer signal is detected and cancer is subsequently diagnosed, may undergo more than one diagnostic test to achieve resolution, which may increase diagnostic activity more than is estimated here. Similarly, some early stage cancers may also be more difficult to diagnose and require a greater number of diagnostic procedures to achieve resolution than late stage cancers. In addition, our model assumed that people for whom no cancer is found during the first diagnostic procedure (i.e. for an incorrect CSO prediction or a false positive result) would undergo a CT-CAP as a second diagnostic procedure, after which no further investigations would be undertaken. However, more than two diagnostic procedures may be carried out in some of these cases.
The type of diagnostic procedure used for people with a CSD MCED test result could also be different in real-world clinical practice than in our model. Our estimates are based on how diagnostic tests are used to investigate cancer in symptomatic people under current standard-of-care in the NHS, but the diagnostic tests used to investigate asymptomatic people referred from an MCED screening programme may differ. We modelled change in activity for broad categories of diagnostic modalities, which was necessary in order to use NHS diagnostic activity statistics; our study, therefore, may miss some nuanced effects of MCED screening by modality. Other tests, such as FIT for colorectal cancer, may also support diagnostic decision making following the detection of a cancer signal with an MCED test; however, it is not yet clear how other diagnostic or triage tests might fit into diagnostic pathways for MCED screening.
MCED screening will ‘re-route’ some cancers from symptomatic diagnostic pathways (including emergency presentations, urgent suspected cancer referrals and GP referrals) [35], due to more cancers being diagnosed before symptoms occur. However, in the steady-state screening programme scenario, we did not directly account for the fact that annual MCED screening would result in some cancers being diagnosed in earlier years, thus reducing diagnostic activity from symptomatic presentation in subsequent years. In practice, the overall impact of MCED screening on diagnostic demand (at steady-state) will be a combination of reduced activity from symptomatic presentation and some increases in activity associated with apparent false positive results and repeat testing.
The CSD rate and PPV used to estimate the number of cancers found by the MCED test in this study implicitly account for any overdiagnosis, as these values come from real-world, prospective cohort studies. However, the interception model used to estimate the proportion of each CSO detected by the MCED test assumes no overdiagnosis. This is due to the low likelihood of overdiagnosis considering the test’s preferential detection of more aggressive (cfDNA-shedding) cancers. However, these CSO proportions could differ if the MCED test led to overdiagnosis in certain cancers.
The screening-eligible population size is based on adults aged 50–79 years in England in 2022. We do not define a specific timepoint at which a MCED screening programme might be rolled out and reach steady-state. The population of England is projected to increase and to age: between 2022 and 2032, the screening-eligible population is projected to increase by approximately 5%, from 18.9 million to 19.9 million [36]. With a growing and aging population, the number of cancer cases is projected to rise. A small increase in age-standardised cancer incidence rates (~1%) is also predicted over a similar timeframe [37]. Our model does not attempt to build in an inflationary increase in the number of people undergoing diagnostic testing following a CSD result at a future time point, but an increase in absolute numbers is expected.
Finally, participation rates in this study did not account for known sociodemographic differences in screening participation. For example, participation in breast and bowel cancer screening in England is lower among people in more deprived socioeconomic groups [38,39,40]. Little is currently known about how sociodemographic factors might affect participation in MCED screening compared with current screening programmes, but any differences could be minimised if known barriers to participation are addressed.


Comments (0)