
Remember me
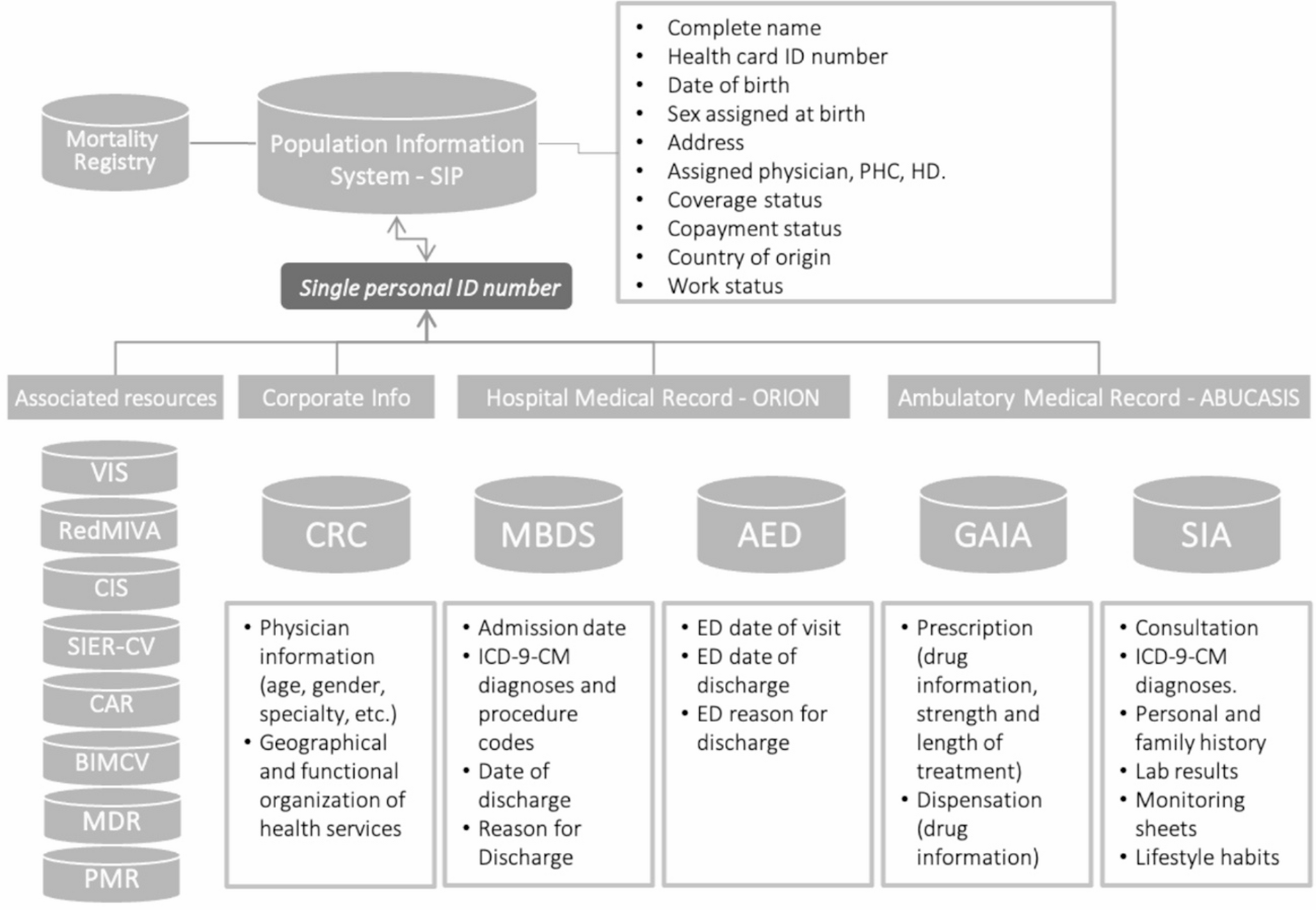

This was a population-based cohort study of all women giving birth at 22 or more gestational weeks between March 1, 2020, and March 31, 2023 (in Sweden) / July 22, 2023 (in Norway) identified in the Swedish Pregnancy Register [21] and Norwegian Birth Registry [22]. Exclusion criteria were: no valid personal identity number and lack of possibility to be followed in the national registers for 42 gestational weeks and 12 weeks postpartum (Fig. 1). Conception dates were estimated based on fetal ultrasonography or the last menstrual period. The first eligible date of conception was March 1, 2020, which was right before the start of the COVID-19 pandemic, and the last conception date with complete follow-up was March 18, 2022. The unique personal identity number was used to link national register data on exposure, outcome, and other covariates. The data sources are further described in the Online Supplementary Information.
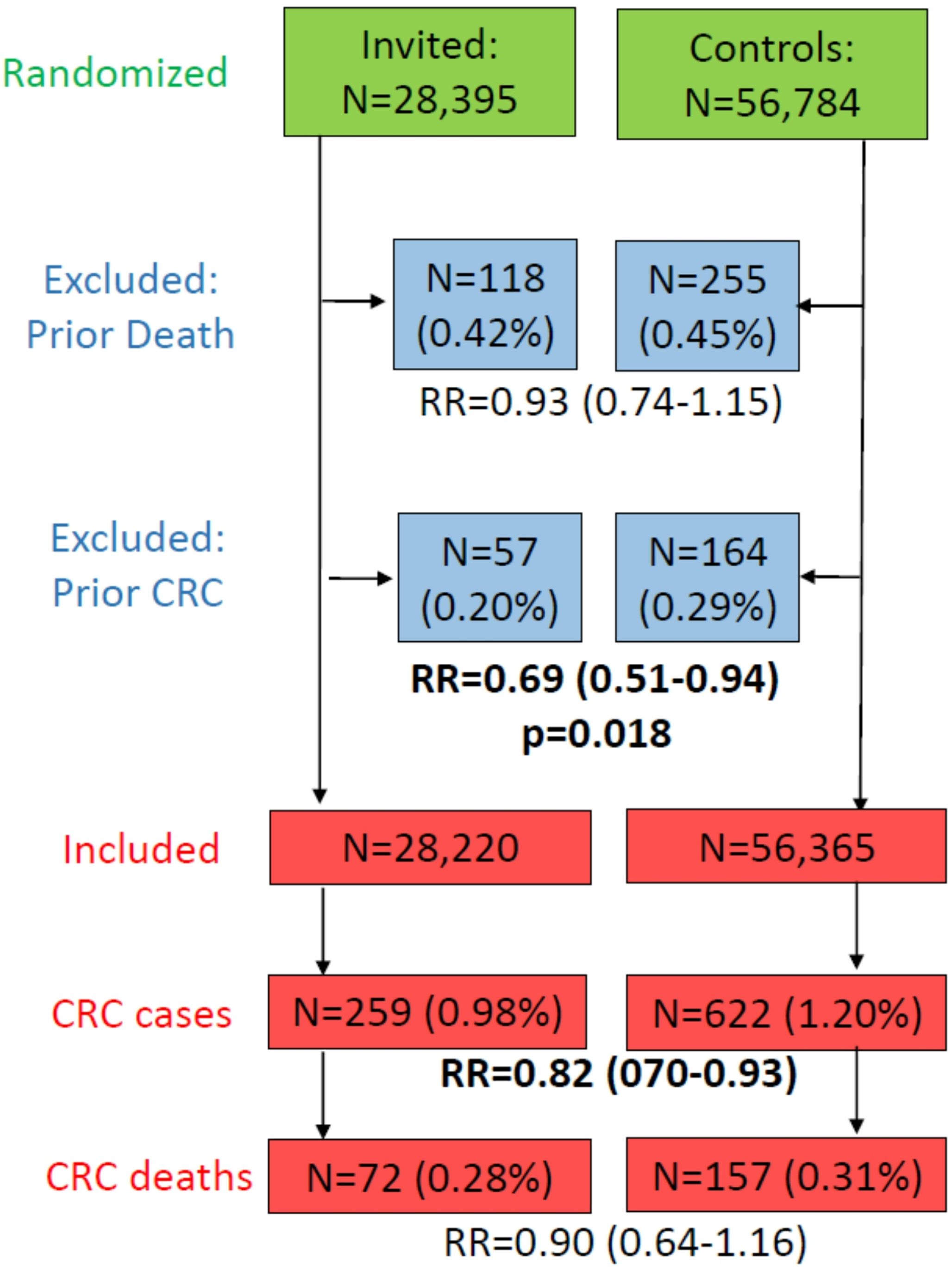
Fig. 1
Selection of the study population in a study of COVID-19 and venous thromboembolism (VTE) in pregnancy and postpartum. VTE venous thromboembolism, gw gestational week, wk week
ExposuresInformation on COVID-19 was identified from national infectious disease surveillance registers. COVID-19 infection during pregnancy and the postpartum period was defined as the first positive PCR test for SARS-CoV-2 between the date of conception and the date of delivery for the pregnancy period and between days 1–84 (12 weeks) after delivery for the postpartum period. The date of when the PCR test was performed, was used in the analysis as a proxy for onset of COVID-19 infection. Although limited by the absence of complete variant sequencing data, we identified four time periods when different variants of the SARS-CoV-2 virus were dominant: Index (1 March 2020–31 January 2021), Alpha variant (February 2021–June 2021), Delta variant (July 2021–December 2021), and Omicron variant (January 2022–March 2022) [23]. Testing strategies in Sweden and Norway [24, 25] are summarized in the Online Supplementary Information.
OutcomeBased on previous validated register-based outcomes of VTE [26,27,28], VTE was defined as an in- or outpatient ICD-10 (International Classification of Diseases 10th revision) code of I26, I80, I81, I82, O223, O871, and O882 (Online resource eTable 2) in the pregnancy and national patient registers using the first record (exact date) identified during pregnancy or postpartum as the time of VTE. The specific codes for superficial vein thrombosis in pregnancy (O222) and postpartum (O870) were not included as our primary interest was in deep venous thromboembolism, which carries a higher risk of morbidity and mortality.
AnticoagulantsBased on Anatomical Therapeutic Chemical classification codes (ATC: B01AA, B01AB, B01AF; Online Resource eTable 3), prophylactic and therapeutic anticoagulants (date of filled prescriptions) up to 3 years before, during, and 12 weeks after pregnancy, were identified from national prescription registers [29, 30].
CovariatesOther characteristics were identified from the pregnancy and birth registers, Statistics Sweden/Norway [31, 32], and national vaccination registers [33] and included age at conception, early-pregnancy body mass index (BMI), early pregnancy smoking status (yes/no), region of birth (Scandinavia, Other European countries, Middle East/Africa, or other), education level (≤ 9 years, 10–12 years, and > 12 years), income (in tertiles), parity (nulliparous, multiparous), multiple pregnancy (yes/no), season of conception (March–April 2020, May–August 2020, September–December 2020, January–April 2021, May–August 2021, September-December 2021, January–March 2022), and COVID-19 vaccination status (at least one dose, yes/no).
Statistical analysesWe used Cox regression analysis to evaluate hazard ratios of VTE according to COVID-19 infection in pregnancy or the postpartum period, separately. The time axis was gestational age in days for the analysis of VTE during pregnancy with the start of follow-up from the estimated date of conception. The time axis in the postpartum period analysis was days from delivery with the start of follow-up on day 1 after delivery. COVID-19 infection was entered as a time-varying exposure, and participants could contribute to both unexposed and exposed follow-up time. The analyses were censored at the date of VTE diagnosis, when a person had been prescribed an anticoagulant within 2 weeks from testing positive for COVID-19, end of study period (date of delivery for the pregnancy analyses/day 84 after delivery for the postpartum period analysis), whichever occurred first, adjusting for anticoagulants up to 3 years prior the current pregnancy, and including anticoagulant use during the follow-up as a time-varying exposure. The sandwich estimator of standard errors was used to account for clustering individuals with several pregnancies during the follow-up. We further adjusted for maternal age, BMI, smoking, region of birth, education, income, parity, multiple pregnancy, and season of conception. Since we lacked sufficient information to impute missing values for education, income, BMI, and smoking, we handled missing data using a missing indicator in the adjusted models. In a sensitivity analysis, individuals with a history of anticoagulants up to 3 years prior to pregnancy were excluded. In secondary analyses, to evaluate whether there was a particular increased risk of VTE shortly after testing positive for COVID-19, we estimated the risk of VTE in the first 2, 4, 8, 12, and 16 weeks following COVID-19 infection. In these analyses, participants were considered unexposed again after the end of the specific risk window. Further, the risk of VTE by different periods of infection (Index, alpha, Delta, or Omicron) was assessed. Lastly, to study whether COVID-19-infected women not vaccinated against COVID-19 were at different risk of VTE compared with women with at least one dose of vaccine before COVID-19 infection, we stratified the analyses on vaccination status at COVID-19 infection.
The data from each country were analyzed separately and subsequently meta-analyzed using a random-effects model, with heterogeneity estimated using the I2 statistic. Results are reported as unadjusted and adjusted hazard ratios with 95% confidence intervals (CI). Analyses were conducted using SAS version 9.4 (SAS Institute) and Stata version 18 (Statacorp, Texas).
Comments (0)