
Remember me

We used personal identification numbers (PIN) to connect data from several Swedish registers, including the National Medical Birth Register (MBR), the Swedish Multi-Generation Register (MGR), the National Diabetes Register (NDR), the National Patient Register (NPR), the National Prescribed Drug Register (NPDR), the Health Insurance and Labour Market Studies register (LISA), as well as the Swedish emigration and death registers [16, 18,19,20,21,22].
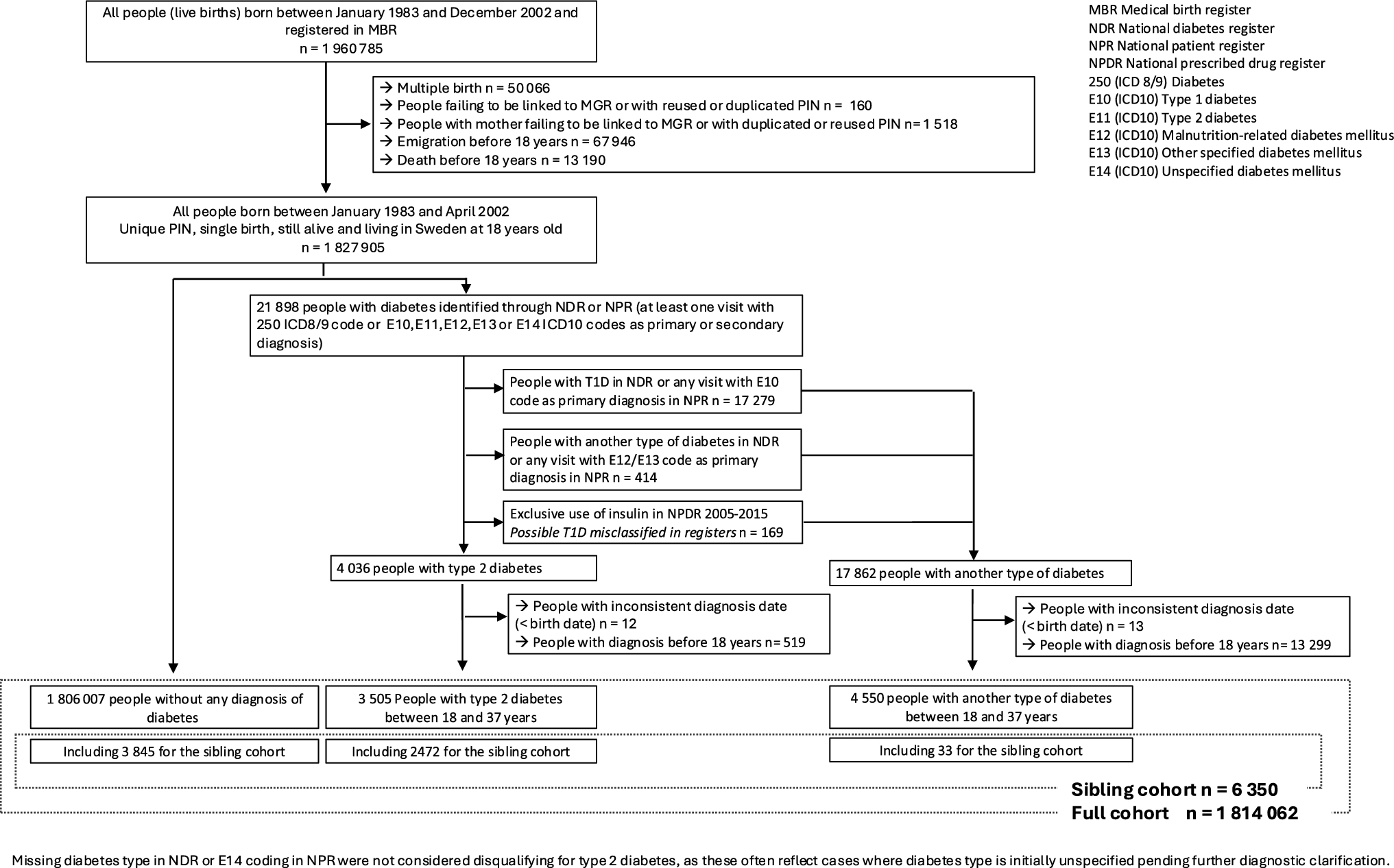
MBR, which has been created in 1973, compiles standardized data from perinatal exams for all births in Sweden, including the international classification of diseases (ICD) codes for certain maternal diagnoses [18]. Our study included all individuals born in Sweden and recorded in the MBR from 1983 to 2002 (1,960,785 live births). These years were selected because some early-life exposures were not documented in the MBR before 1983 (specifically maternal body mass index [BMI], maternal smoking, and family situation at childbirth), and because we set the starting age of follow-up to be 18 years (data availability for identification of diabetes cases ends in 2020). This implies that we could follow people to a maximum of age 37 (people born 1983). Thus, we focused on early-onset T2D (≤ 37 years) and excluded youth-onset cases (< 18 years) to minimize the risk of including T1D cases since previous studies indicated very low rates of youth-onset T2D in Sweden [13, 23].
We excluded pregnancies with multiple births (50,066, 2.6%) and participants without linkages to the MGR or with system-identified duplicated or reused PINs (160, < 1%). Additionally, participants whose mothers were not identified in the MGR or had a duplicated or reused PIN were excluded (1518, < 1%). Participants that could not be linked to their fathers were retained in the study, considering paternal information missing.
The exclusion of participants who emigrated from Sweden or died before reaching 18 years of age (81,136, 4%) and those diagnosed with any type of diabetes before age 18 or without a reliable diagnosis date (13,843, < 1%) resulted in a final cohort of 1,814,062 individuals. For the sibling cohort, we included only sibling groups (born from the same mother) with at least one sibling affected by T2D (n = 6350). The population selection is summarized in Fig. 1. The study was approved by the Swedish Ethics Review Board (registration number: Dnr 2021–02881).
Fig. 1 Information on diabetes
Information on diabetesWe identified diabetes cases using available data from the NDR and the NPR until 2020. Additionally, we used the NPDR to enhance precision regarding diabetes type and onset date. The NDR, established in 1996, encompasses both primary and secondary diabetes care in Sweden, and was estimated to account for 87% of all individuals living with diabetes in the country in 2019 [24]. The NPR includes inpatient (hospital discharge) and outpatient specialist care data since 1964 and 2001, respectively [20].The NPDR, starting from 2005, records all prescribed medications dispensed in Sweden, categorized according to the Anatomical Therapeutic Chemical (ATC) classification [21].
We defined diabetes cases (n = 21,898) as participants with at least one record in the NDR or at least one visit documented in the NPR with a primary or secondary diagnosis code of “250” (ICD-8/ICD-9 code) or “E10-E14” (ICD-10 codes).
Cases were classified as T2D (n = 4036) if they had no record of another type of diabetes in NDR or NPR (primary diagnosis). To preserve sensitivity, missingness on diabetes type in NDR or E14 coding (“unspecified diabetes mellitus”) in NPR were not considered disqualifying conditions for T2D as these situations can occur when diabetes type is unspecified at early stage after diagnosis and additional diagnostic information is needed, especially in young adults. To ensure specificity, subjects with other types of diabetes formally recorded in NDR or NPR (i.e., E10, E12, E13) and individuals exclusively treated with insulin, for the whole follow-up period, according to data available from NPDR, were censored at the age of diagnosis (n = 17,862). Age of diagnosis was based on the first record in any of the registers.
Familial and sociodemographic factorsWe determined parental age (< 20 years, ≥ 20 & < 25 years, ≥ 25& < 30 years and ≥ 30 year) and family situation (two-parent, single-parent, or other situation) at birth using data from the MBR, and the highest parental educational level at birth (categorized as “Primary” for up to compulsory education [≤ 16 years old], “Secondary” for upper secondary education [16–19 years old], and “University” for college/university and further education) from the LISA register [22]. Additionally, the parental countries of birth were identified via the total population register and parents were categorized as Sweden or non-Sweden born, distinctly for the mother and the father. Finally, we identified parental diabetes cases (regardless of type) using the same registers as for study participants. For maternal history of diabetes, we additionally accounted for the information available in the MBR regarding pregestational and gestational diabetes diagnoses using ICD codes (ICD-8: 250; ICD-9: 250, 648A, 648W; ICD-10: O240-44) and self-report. Then, we combined all the information to identify the lifetime maternal and paternal history of diabetes. To examine maternal diabetes as a perinatal risk factor, we separately assess the T2D incidence in relation to maternal diabetes with a diagnosis before the participant’s birth (thus accounting for pregestational and gestational diabetes) from cases with a diagnosis after the participant’s birth.
Pre- and perinatal factorsUsing data from the MBR, we examined maternal BMI (< 18.5 kg/m2[underweight], 18.5–25 kg/m2[normal], 25–30 kg/m2 [overweight], and ≥ 30 kg/m2 [obesity]), and maternal smoking (none, 1 to 9 cigarettes per day, and ≥ 10 cigarettes per day) at the time of enrollment in maternal health care (first trimester). Additional factors studied included the mode of delivery (C-section or vaginal), gestational age (categorized as extremely to very preterm [≥ 22 to < 32 weeks], moderate to late preterm [≥ 32 to < 37 weeks], early term [≥ 37 to < 39 weeks], full term [≥ 39 weeks]), size for gestational age (small [SGA] or large [LGA] for gestational age, defined as birth weight below -2 or above + 2 standard deviations for the sex-specific distribution of birth weight in people born at the same gestational age), birth weight (< 2500 g, ≥ 2500 g and < 3500 g, ≥ 3500 g and < 4500 g, ≥ 4500 g), and birth order [25, 26].
Additionally, we identified pre-eclampsia using ICD codes (ICD-8: 637; ICD-9: 642E-G; ICD-10: O14-O15) from the MBR, and maternal infections during pregnancy using infection-related ICD codes from the NPR, as detailed in supplementary Table S1.
Statistical analysesWe described the distribution of exposures and covariates using frequencies and proportions for categorical variables, and means and standard deviations (SD) or median and interquartile range (IQR) for continuous variables. We used Cox proportional hazards (PH) regression models to estimate the hazard ratios (HRs) and 95% confidence intervals (CIs) for the incidence of early-onset T2D in relation to early-life exposures. The follow-up period was calculated from the participants’ 18th birthday to the occurrence of diabetes, death, emigration, or April 21, 2020. The models used age as the time scale.
Missing values for categorical variables were treated as a separate category. For continuous covariates, the median value of the distribution was imputed for individuals with missing values, with an additional variable to indicate if the value was imputed or not. Overall, the percentage of missing values was low (ranging from 0 to 6%) except for maternal BMI (29%), which is due to the gradual introduction of the variable in the 1980s, as well as a complete lack of data for two consecutive years caused by an error in the data collection system rather than selective reporting of the mothers [18].
In the full cohort analysis, Cox models were conducted with a cluster-robust standard error to account for familial clustering among siblings born to the same mother. Each association between exposure and early-onset T2D was separately adjusted for sex and year of birth (Model 1). Then, all perinatal and familial factors were mutually adjusted for (Model 2) and finally (Model 3) we added adjustment for parental lifetime history of diabetes.
In the sibling analysis, we performed the Cox model with stratification on sibling groups for suitable exposures (sex, maternal BMI, diabetes, smoking and infection during pregnancy, pre-eclampsia, gestational age, birth weight, birth size, and mode of delivery), excluding exposures that were quasi-systematically concordant (family socio-educational background and parental lifetime history of diabetes) or systematically discordant (year of birth, birth order and parental age at childbirth) within siblings. Each association between exposure and early-onset T2D was separately adjusted for sex (Model 1). Then, all perinatal factors were mutually adjusted for (Model 2). Methods and interpretation of the sibling analysis are further detailed in the supplementary material.
Finally, we tested for an interaction between sex and perinatal exposures associated with early-onset T2D in the full and sibling cohort analyses, as sex-specific susceptibility to the intrauterine environment has previously been described, and sex differences have been observed in attributable risk factors for early-onset T2D [4]. To do so, we compared models with and without an interaction term, using the Likelihood ratio test.
We verified the PH assumption by plotting Schoenfeld residuals and performed stratified analysis if a violation was observed. All analyses were conducted using R, version 4.3.1.
Comments (0)