
Remember me

Retrospective population-based cohort, comprised by pregnant women and their offspring, between July 1, 2009 and December 31, 2021 (the cohort is planned to be periodically updated), which will be followed from 6 months pre-conception until end of pregnancy (delivery, stillbirth, spontaneous abortion, elective termination), death, loss of coverage. This cohort does not include pregnancy planners per design. Elective terminations performed outside the public health system are not included either as this information is not available in VID. Exclusion criteria: non-residents in the Valencia region, due to limitations in the follow-up of the prescriptions and events foreseen in the study; women without pharmaceutical benefits covered by the Spanish NHS (civil servant service insurance mutualities) due to the limitations to identify their pharmaceutical consumption since it is not available in VID.
SettingThe study was carried out in the Valencia region, Spain and, specifically, in the population covered by the Valencia Health System (VHS), the public health system that covers 97% of the population of the region, around 5 million inhabitants.
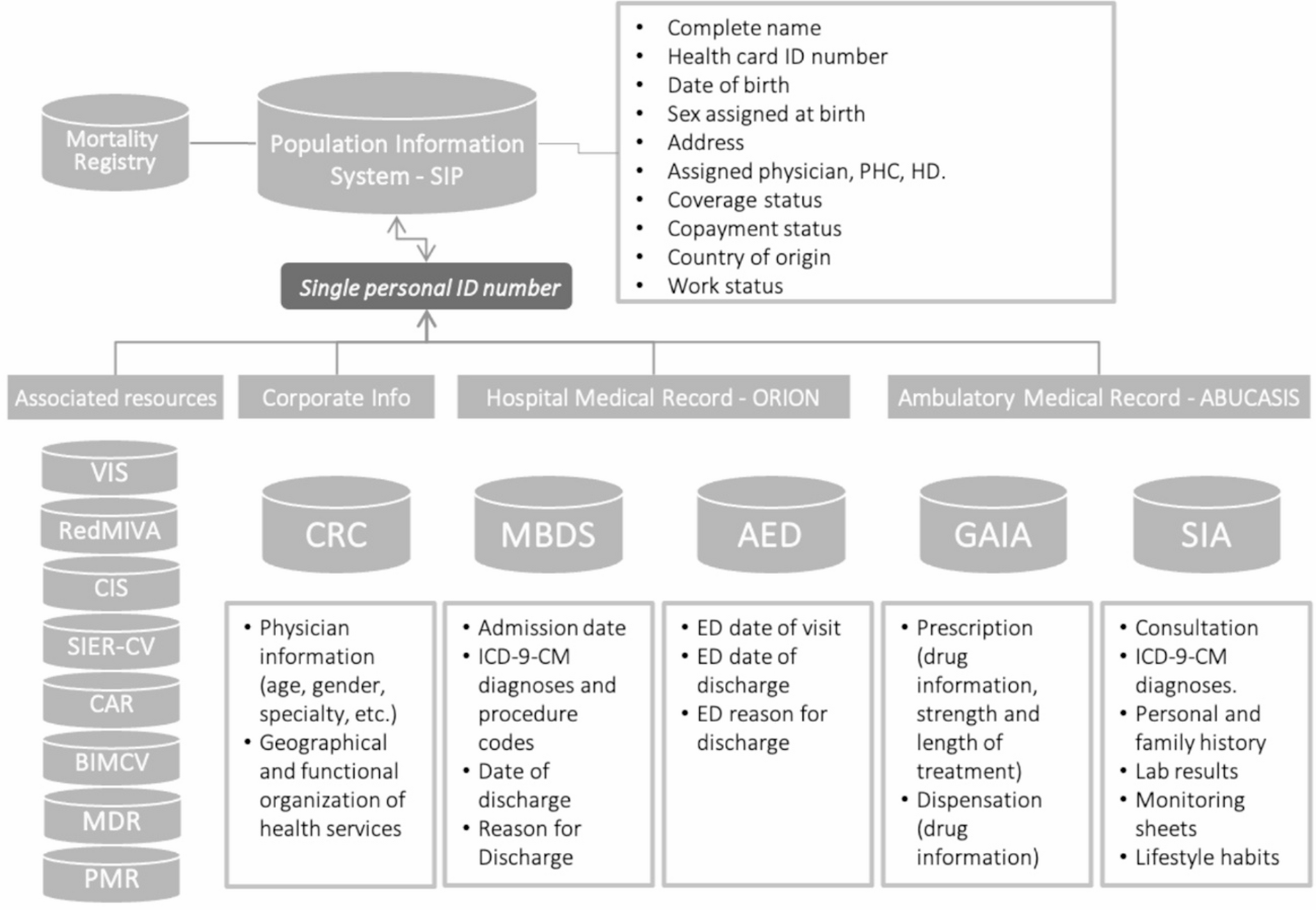
Data sourcesThe necessary information was obtained from VID for the time window January 1, 2009 to December 31, 2021. This way we obtained all the information (baseline-lookback period of 6 months, which allows to have also information of drug exposure available from preconception and throughout pregnancy) of all women included in the 2009–2021 cohort. The information was obtained specifically from: (1) Population Information System (SIP) that provides a unique patient identification number (included in all health information systems) and registers some sociodemographic characteristics (e.g., age, gender, country of origin, income, etc.), residence and coverage information (including the date of death); (2) Minimum Basic Data Set (MBDS) at hospital discharge that includes diagnoses and procedures under hospitalization coded by the International Classification of Diseases 9th revision Clinical Modification (ICD9CM) until 2015 and by the ICD10ES since 2016; in addition to key information for the present study such as gestational age and weight of newborns; (3) Ambulatory Information System (SIA), the electronic medical record available in all primary care centers and specialized outpatient care that includes information on patients regarding active diagnoses, personal and family medical history, laboratory results, lifestyle habits, results of diagnostic tests, etc., as well as health service utilization; and all the information on both prescriptions issued by primary care doctors and specialists and the prescriptions filled by the patients. (4) Electronic obstetric sheet (EOS). This is actually contained in SIA but we are briefly describing it separately giving its relevance in the pregnancy stage. EOS is mainly filled out by midwifes, containing information recorded at every prenatal visit from the first pregnancy-related appointment. It contains, among others, date of LMP and/or gestational age by ultrasound, maternal lifestyle factors during pregnancy, end of pregnancy and type of end, (e.g. spontaneous abortion, elective termination, etc.) with date of occurrence; (5) Accident & Emergency Department (AED) clinical record, which provides triage data, diagnoses, tests and procedures performed in public emergency rooms; (6) Corporate Resources Catalog (CRC), includes information on both, geographical and functional organization of the provision of care in the region (distribution of hospitals, primary care centers, etc.) and health care professionals (including age, gender and specialty); (7) Metabolic diseases registry (MDR), which is actually a birth registry, including all live births of the region, from both public and private hospitals; (8) Perinatal mortality registry (PMR) which registers all perinatal deaths of the region, from the public and private health systems; (9) Vaccine information system (VIS); and 9) Congenital anomalies registry of the Valencia Region (CAR). See Fig. 1 for a graphic description of the Valencia Integrated database and associated registries.
Fig. 1
Valencia health system integrated database (VID) and their associated registries. Abbreviations: VIS, Vaccine Information System; RedMIVA, Microbiological Surveillance System; CIS, Cancer Information System; SIER-CV, Rare Diseases Information System; MDR, Metabolic Diseases Registry; PMR, Perinatal Mortality Registry; CAR, Congenital Anomalies Registry of the Valencia Region; BIMCV, Medical Image Bank; MBDS, Minimum Basic Data Set; AED, Accident & Emergency Department; CRC, Catalogue of Corporate Resources; GAIA, Pharmaceutical Module; SIA, Ambulatory Information System.
Adapted from: Sanfélix-Gimeno, BMJ Open 2015; Garcia-Sempere, Int J Epidemiol, 2020. [Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license].
Pregnancy cohort constructionAlgorithm to identify pregnanciesThe algorithm is developed using a hierarchical approach where records with available gestational age are prioritized, allowing an accurate assessment of the duration of pregnancy. If a pregnancy is identified in one step, the interval of that pregnancy (+ 40 days at the end) is blocked for subsequent steps. Therefore, only pregnancies not identified in a previous step are collected in each step.
The process starts with the collection of live births from the MDR, which records all live births with a high percentage of recorded gestational age (98%) and weight at birth (98%). However, there are errors or missing values for some of the mothers’ identifiers, so we were not able to retrieve all livebirths (linked to the mother) from this registry. Then some additional live births and most of the stillbirths are gathered from the PMR. Next, additional live births and stillbirths with birth defects are taken from the CAR. Then we use the MBDS to include elective, spontaneous and unknown abortions, as well as some live births and stillbirths that are missing from other registries. Then we collect additional data on live births, stillbirths and spontaneous abortions from the Electronic Obstetric Sheet (EOS), which is available in the SIA. Finally, for records from AED, pregnancies are retrieved using ICD-9 and ICD-10 codes. See Fig. 2. Given that pregnancies are identified sequentially, and pregnancy outcomes are determined based on the highest hierarchical source, following the order: MDR > PMR > CAR > MBDS > EOS > AED. In case of duplicates or discordant records in pregnancy outcomes, we applied a hierarchical reconciliation process. When conflicting outcomes were found across sources, the outcome recorded in the highest-ranked source (MDR > PMR > CAR, etc.) was prioritized.
Fig. 2
Cohort construction flowchart*. Abbreviations: MDR, Metabolic Diseases Registry; PMR, Perinatal Mortality Registry; CAR, Congenital Anomalies Registry of the Valencia Region; MBDS, Minimum Basic Data Set; EOS, Electronic Obstetric Sheet; AED, Accident & Emergency Department; LB, Live birth; SB, Stillbirth; ET, Elective termination; SA, Spontaneous Abortion. Only pregnancies not identified in a previous step are collected in each step. * Only pregnancies not identified in a previous step are collected in each step
Pregnancy period definitionIn order to adequately estimate the pregnancy period (and therefore, the exposure period), an accurate definition of the conception date, as well as of the end of pregnancy date is of utmost importance. Start of pregnancy was defined as the conception date, end of pregnancy was defined as occurrence of spontaneous abortion, elective termination, stillbirth or live birth.
Date of conceptionThe following criteria was used to define conceptional date: (1) From gestational age (mainly calculated by ultrasound) available in the MDR, PMR, CAR, MBDS, EOS and AED. Currently this information is available in 97.5% of deliveries) (2) In the remaining deliveries, if weight is available it was estimated from the date of delivery (minus 40 weeks when the child’s weight is greater than 2.5 kg, and using a linear regression model in the case of lower weight children), this approach has been previously used by our group [35]; (3) In the case of stillbirths, gestational age as defined by ultrasound was available in the 97.4% of pregnancies. (4) In pregnancies that have ended in abortion, gestational age was used when available (50.4% of the cohort). Regarding elective terminations, gestational age is present in 9.6% of pregnancies. If information on gestational age was not retrieved, it was imputed using the median gestational age derived from the type of end of pregnancy.
End of pregnancy dateThe date in which the pregnancy ended was defined as follows: (a) In the case of live birth: date of birth registered in MDR, PMR, CAR, MBDS, EOS or AED (b) In the case of stillbirth: the date in which the fetal death was registered (the date of occurrence of the death) in the PMR, CAR. MBDS, EOS or AED; (c) In the case of elective terminations: date in which the procedure was registered in the MBDS or AED; (d) In the case of spontaneous abortion: date in which the diagnostic code for spontaneous abortion was registered in the MBDS or AED, or that type of end was registered in EOS.
Drug exposure informationObtained from the pharmaceutical module (GAIA) of the ambulatory medical record. It contains all the information on both, prescriptions issued by primary care doctors or specialists and the prescriptions filled by the patients, including active ingredient, pharmaceutical presentation (dose, type of pharmaceutical forms, number of forms), dosage (prescribed dose and cadence), prescription and dispensing dates, etc. See supplementary Table 1 for a detailed description of prescription and dispensing data available.
OutcomesPregnancy and neonatal outcomesIt is important to note that the PREGVAL cohort is not a birth cohort, but a pregnancy cohort (with its limitations, not including pregnancy planners), and thus, it retrieves data not only on livebirths but also on pregnancies which ended in stillbirth, spontaneous abortion or elective termination. Among live births, we considered the following outcomes: (a) Congenital anomalies: Retrieved from the congenital anomalies registry. All diagnoses have been validated, so there is a low likelihood of misclassification in information obtained from this registry. Information of birth defects diagnosis is collected from livebirths and stillbirths; (b) Low birth weight: Defined as birth weight under 2500 gr regardless of gestational age; and (c) preterm birth: Defined as birth before the 37th gestational week.
Long-term outcomesGiven that we are able to link the mother and offspring, follow-up from birth and along the lifecycle is feasible, to assess postnatal outcomes including (neuro) developmental disorders, among others.
CovariatesA wide range of key factors that are related to relevant pregnancy outcomes and can confound the association with drug exposure are available, as follows: (1) Concomitant medications during pregnancy: Information is available for primary and specialist care, and it includes: active ingredient, pharmaceutical presentation (dose, type of pharmaceutical forms, number of forms), dosage (prescribed dose and cadence), prescription and dispensing dates, etc. (see supplementary Table 1); (2) Sociodemographics: maternal age, income level (copayment, which is based on personal income), risk of social exclusion as determined by a composite index; (3) Chronic comorbidity (See supplementary Table 2); (4) Pregnancy-related diseases (see supplementary Table 2); (5) Laboratory data, available for primary and specialist care. (6) Lifestyle habits: smoking, alcohol consumption, recreational drug abuse, sedentary behaviour (See supplementary Table 2). These variables were ascertained by diagnoses codes (which in our case are active diagnosis codes, that for chronic conditions, once they are activated remain activated); (7) Previous medication use: Availability of information as in the item “medications during pregnancy” (see supplementary Table 1). The time window can be extended backwards at least three months; (8) Use of health services previous to conception date or during pregnancy: visits to the emergency room, primary care, specialized care-identifying the specialty, hospitalizations); (9) Healthcare system: Basic Health Zone, Health Department.
Comments (0)