We report one of the first comprehensive descriptions of population-based reference values for traditional time-domain and frequency-domain HRV measures and advanced measures of cardiac autonomic function. Cumulatively, these measures capture different aspects of the ANS. Moreover, we describe the distribution of these measures across different sexes and age-groups.
The KORA Study is a population-based cohort, which was designed to represent the age- and sex-stratified population in the South German region around the city of Augsburg [23]. Balancing resources, in a subset of the KORA F3 survey digital 12-lead 24-h Holter-ECGs were conducted. This subset was confined to an age-spectrum from 54 to 79 years aiming to reflect the part of the population, which is prone to develop cardiovascular conditions. It was thus unclear how the reported measures in our cohort would compare to prior findings, particularly because many of these reports were derived from in-patient cohorts with major cardiovascular conditions [13,14,15,16,17,18,19,20,21,22]. HRV description in non-diseased cohorts are rare. One of the largest studies in such individuals enrolled healthy individuals only who were not representative for the general population [34]. Also, the methodology of this study and the interpretation of the results raised concerns [35].
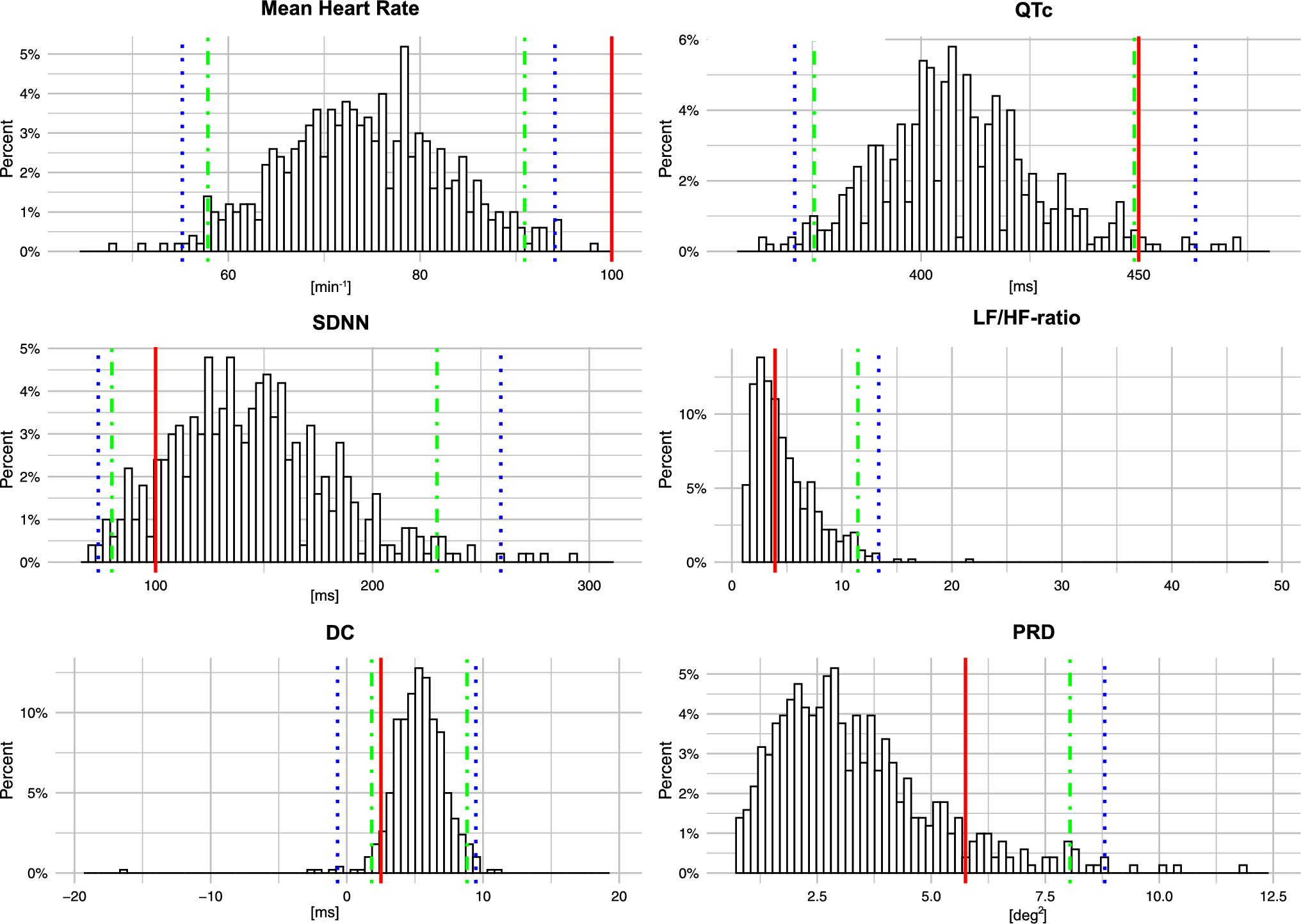
The Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology previously has proposed reference values for HRV measures. For the time-domain measure SDNN, the reference value is a mean of 141 ± 39 ms [12, 36]. Other sources report a mean of 166 ± 32 ms for SDNN [11, 18, 37,38,39,40,41,42,43]. Yet, many of these prior studies were small, partly relying on 14 healthy participants only [42]. In our study of over 500 participants, we report a mean SDNN of 145 ± 38.5 ms. Our findings are hence well in line with these previous reports.
For LF/HF-ratio as an example of a frequency domain measure of HRV, a relevant distribution difference by sex and minor distribution differences by age-group have been described [34, 43]. There, in the age-group > 50 years, which is closest to our current age distribution, the median LF/HF-ratio was 2.58 [1.64;3.57] in women and 3.08 [2.16;4.25] in men [34]. With a median LF/HF-ratio of 3.37 [2.36;4.53] in women and 5.15 [3.23;7.20] in men, values were markedly higher in our population-based study. The specific reasons for these differences remain incompletely understood. However, our analysis is based on a large, population-based cohort, whereas the respective prior values were based on relatively small subsets of volunteers.
Likewise for DC and PRD, population-based reference values are currently missing. For DC, we report a mean of 5.25 ± 2.4 ms in our unstratified cohort. DC has first been reported in 2006 in patients after an acute MI. In this initial description, the unstratified mean value was 5.6 ms [13]. For PRD, the population-based reference median in our study is 2.92 [2.06;4.14] deg2. Despite several reports on the clinical implications of PRD cut-offs [14, 19, 20, 22], the respective cohort median values had not been reported. Of note, the reported cut-off values for PRD and other measures were derived from diseased cohorts with a generally higher propensity of pathologic values. In our population-based cohort, concomitant conditions only occur with a population-based prevalence. Our cohort can thus be considered “healthier” and pathologic values occur less frequently.
The clinical applicability of measures depends on their stability in relevant strata of the population. Importantly, we have investigated differences in the distribution of traditional HRV measures and advanced measures of autonomic function across sex both in our unstratified cohort and an “apparently healthy” cohort subset without overt cardiovascular conditions. We observed some variability for the frequency-domain measure LF/HF-ratio, which is known to be affected by influencing factors including physiological, psychological, environmental, lifestyle, and genetic factors [44]. However, time-domain measures as well as the advanced marker DC and PRD, were distributed comparably in men and women, both in the unstratified cohort and in the “apparently healthy” subset. This is partly in contrast to a prior report suggesting these measures to be higher in men than in women [34]. Regarding age, our cohort covered individuals from 54 to 79 years. Time-domain and frequency-domain measures were quite stable across age-groups. However, DC constantly decreased with increasing age both in the unstratified cohort and in the “apparently healthy” subset. Whereas PRD appeared stable across age-groups in the unstratified cohort, in the “apparently healthy” subset a significant increase with increasing age was revealed. It has been suggested that a reduction of cardiac autonomic control during aging is particularly driven by a reduction in vagal tone leading to a predomination of sympathetic tone [45, 46]. Our results of an age-dependent decrease of parasympathetically mediated DC and reversely an age-dependent increase in sympathetically mediated PRD support these previous findings. Our “apparently healthy” cohort thus offer a slightly clearer view of physiologic aging, while the unstratified data may better reflect real-world clinical populations.
Cardiac autonomic tone is influenced by different ANS components. To examine, whether the selected measures tag independent aspects of autonomic tone, we systematically calculated correlations between them. We thereby noted that all parameters, especially DC and PRD, were not relevantly correlated, neither with other time- or frequency-domain measures nor among each other. We submit that this lack of correlation underpins the independent and incremental information provided by these measures.
Clinical interpretability of both HRV measures and of advanced measures of cardiac autonomic function is of great importance. It is critical if measure-specific cut-off values confer a quantifiable risk for outcomes and if the prevalence of such cut-off values is influenced by concomitant conditions. For the time-domain measure SDNN, a value ≤ 100 ms is predictive of sudden cardiac death (SCD) in patients following a MI [11]. Likewise, DC ≤ 2.5 ms has been associated with increased mortality in post-MI patients [13]. Finally, as a quantification of impaired sympathetic function, PRD ≥ 5.75 deg2 is the only measure that has been established as a SCD risk marker in patients with ischemic and non-ischemic cardiomyopathy [14, 21, 47]. However, such clinically established cut-off values derived from selected, pre-conditioned cohorts including post-MI cohorts might not be generalizable to a population-based cohort. Accordingly, for SDNN and PRD, only around 1 in 10 participants exhibited values exceeding and undercutting the clinically established cut-off values, respectively. Interestingly, for DC only 5.2% of participants fell below a DC cut-off of 2.5 ms. In our cohort it remains unclear if DC as a marker is more sensitive to subtle parasympathetic impairment, or if our results reflect that DC showed a significant age-dependency with lower values in older age-groups.
As mentioned, cut-off values for SDNN, DC, and PRD have been associated with increased mortality and partly (PRD) also for SCD [11, 13, 14]. Ideally, a predictor of SCD-risk should be independent of other influencing factors. To test the stability of our measure distributions in the context of possible influencing factors, we describe the propensity of cut-off values for SDNN, DC, and PRD depending on the presence of hypertension, MI, stroke, and diabetes mellitus, as well as the intake of betablockers, a commonly prescribed cardiovascular drug that is supposed to interact with the ANS. Given that no established cut-off for LF/HF-ratio has been published, we investigate the propensity of values below or above the overall cohort’s median. Both SDNN and DC were significantly modified by all three constellations, namely presence of hypertension, intake of betablockers or history of either stroke, MI or diabetes, with a higher propensity of pathologic values in the concomitant risk groups. Importantly, PRD was not significantly influenced by the three constellations, rendering it a very stable marker of cardiac autonomic function. This fact might be considered important for clinical applicability. Future research will need to investigate if SDNN, DC, and PRD, and eventually LF/HF-ratio, predict SCD and mortality more generally also in the general population rather than in specific subgroups that already are at an increased risk of events.
Limitations
Some considerations are required when interpreting our data. First, our selected cohort is a subset KORA F3 study for which selection bias cannot fully be ruled out. However, this cohort is among the largest investigations to report reference values for ECG-based measures. The cohort is derived from the general population and consequently, it is not enriched for high-risk patients with severe cardiovascular conditions. Such conditions only occur at a population prevalence, which renders it difficult to investigate HRV measures in high-risk strata of the population. Also, the age range of our cohort was confined to 54 to 79 years. We hence cannot sufficiently adjudicate the generalizability to younger and older age groups. Similarly, the cohort comprises participants of German nationality. Although not suggested by prior data, HRV measures might be distributed differently in other geographic regions or in individuals of other descent. We report a comprehensive selection of traditional and advanced measures. However, numerous other measures exist which were not available in our cohort [48]. Methodologically, our measures were derived from standard 12-lead Holter ECGs recorded under ambulatory conditions with a resulting high activity level compared to severely diseased in-patients. A head-to-head comparison of measures across such very different underlying circumstances requires careful individual interpretation. It will be important to analyze if pathologic measures obtained on a population level can also be interpreted similarly to those under clinical conditions.
In conclusion, we present one of the first and one of the largest cohorts to establish population-based reference values for traditional HRV measures and for advanced measures of cardiac autonomic function. The markers DC, quantifying cardiac parasympathetic tone, and PRD, quantifying cardiac sympathetic tone, have not previously been described and quantified in the population. We demonstrate that traditional HRV measures and advanced measures of cardiac autonomic function are largely independent of sex. PRD is a marker that is particularly stable across age and is not relevantly modified in the context of cardiovascular conditions. It will be a future research questions to test, whether our tested measures including DC and PRD are predictive of clinical outcomes in the general population.


Comments (0)