We found that HC users, both SARC and LARC types, have a significantly lower risk of anaemia compared to non-users of HC, ranging from 23% lower risk for users of oral contraceptives containing drospirenone and ethinylestradiol to 60% lower risk for users of desogestrel-only. By quantifying effect sizes, we demonstrate for the first time that on a population level, different HC products associate differently with iron balance in a product-specific manner.
Most of COCs, both those containing ethinylestradiol and natural oestradiol, were negatively associated with anaemia. Compared to COCs containing ethinylestradiol, natural oestradiol-containing COCs are associated with lower uterine bleeding, and some (dienogest and oestradiol) indicated for treatment of HMB [7]. Therefore, they are likely to offer better anaemia protection, as also supported by the present results. Notably, the effect size estimates for the natural oestrogen products were similar despite the difference in age profile of their users (Figure S2). This indicates that the effect is primarily attributable to the contraceptive itself, rather than any underlying variables. The lower risk of anaemia was not limited to combined oral contraceptives, but was also associated with the use of contraceptive vaginal rings.
Curiously, use of POCs, namely desogestrel-only was associated with the largest difference in effect size estimate compared to non-users, suggesting they offer the best protection against anaemia. This is somewhat surprising, as in contrast to combined oral contraceptives, POCs are associated with irregular bleeding, including amenorrhea and spotting. This suggests that, if well tolerated, their use does not need to be discontinued. Self-selection of long-time users with acceptable bleeding patterns or amenorrhea within this group is likewise possible, as women experiencing spotting throughout their cycle may decide to change HC type. However, single purchase of desogestrel POCs (signalling discontinuation of use) was not more common compared to other HC in the study population.
Interestingly, the use of LNG-IUD was associated only with a modestly (36%) reduced risk of anaemia compared to non-users, despite previous studies identifying LNG-IUDs as the most effective HC product in iron deficiency and anaemia prevention in healthy women [4, 17], as well as being used as first-line treatment for HMB. Our study is likely to underreport LNG-IUD use due to how Finland’s healthcare system is organized. Women using LNG-IUDs for contraception receive them often via prescription, while those with abnormal uterine bleeding receive the LNG-IUD used for therapeutic purposes directly from clinics. Moreover, starting from the mid-2010s, an increasing number of municipalities offer the first LARC free-of-charge, thus excluding these women from the study. Other LARCs (i.e. levonorgestrel and etonogestrel releasing implants) did not associate significantly with the risk of anaemia, likely due to a low number of implant users.
Our results contrast to previous, smaller studies on healthy women conducted in Italy and New Zealand [14, 15], as well as studies on Danish and Dutch whole blood donors [16, 17, 21], which found no associations between systemic HC use and iron deficiency and/or anaemia. However, our results complement previous population-level studies from low- and middle-income countries [10,11,12, 22, 23] by showing that the protective effect extends to populations in affluent countries. This was seen despite the likely differences in prescribing patterns and causes for anaemia. Additionally, our results suggest product-level differences.
It may be argued that the large number of users explain our significant results, as numerous users of a specific contraceptive preparation could act as a proxy for an established user base (i.e., women who have been using the product for multiple years without subjective side-effects and acceptable bleeding pattern), leading to lower odds of anaemia. Newer products, with a lower number and less established users, are more likely to be prescribed to younger women as their first HC, as opposed to women already satisfied with their HC. However, as the 95% CIs of the desogestrel-only POC, and COC containing drospirenone and ethinylestradiol, the two largest groups in comparison, do not overlap, we can be confident that their effect sizes actually differ, making this an unlikely sole explanation.
Decrease in volume of menstrual blood loss is likely the main mechanism for the decreased risk of anaemia in HC users. However, as there are differences even among the different groups, as well as the similarity in effect between fixed and sequential products, it is likely that some of the effect is caused by other mediating factors related to the hormone content. Additionally, some of the effect could be attributed to oestrogen-induced suppression of hepcidin, leading to higher iron absorption and reserves. Although previous studies have found that even short-term use of HC reduces the likelihood of anaemia, long-term use has been observed to further lower the odds. This suggests a cumulative effect of gradually improving iron stores [10, 12].
Despite our efforts to adjust for confounders, we recognise the limitations of this study. First, our study can only account for the HC purchases, excluding information on women who receive HC free-of-charge as part of municipal programmes available in around 70% of the 100 most populated municipalities in 2019. To account for this, we performed subgroup analysis excluding women less than 25 years-of-age, the age group most often included in these contraceptive programmes, which did not notably change results. Similarly, our study did not include data on anaemia diagnosis of women who only utilize private or occupational health care services. However, as results were similar in the crude model and the fully adjusted model, which accounted for socioeconomic group, it could be argued this loss of data decreases power, rather than precision. Second, a purchased HC product is not a guarantee of use. However, by requiring at least two subsequently redeemed prescriptions of the same product in one year window, we were able to control for primary non-compliance as well as minimise the risk of discontinuation of the prescribed HC. Thirdly, residual confounding due to unmeasured factors, such as genetic variance, smoking, diet, or iron supplementation, cannot be ruled out. The Finnish population is relatively genetically homogeneous, which limits the impact of variation in our cohort. By removing prevalent cases before start of follow-up we attempt to minimize residual confounding due to underlying predisposition to anaemia that could be caused by unmeasured risk factors. Prior diagnosis can be used as a proxy for underlying risk, as a clinically significant hereditary predisposition would likely have already manifested by adult age. Nevertheless, further studies with more ethnically diverse populations are warranted to examine confounding caused by varied genetic predispositions and lifestyle factors to anaemia.
Healthy-user bias could further confound results, as it is possible that health-conscious women seek healthcare more often and are more likely to be prescribed HC [24]. Women prescribed HC are also more likely to attend other healthcare providers. As such, estimates may be underestimated. In addition, the loss of information on therapeutic use of LNG-IUDs is likely to result these women being classified as non-users of HC, which likely causes an underestimation of the overall effect sizes.
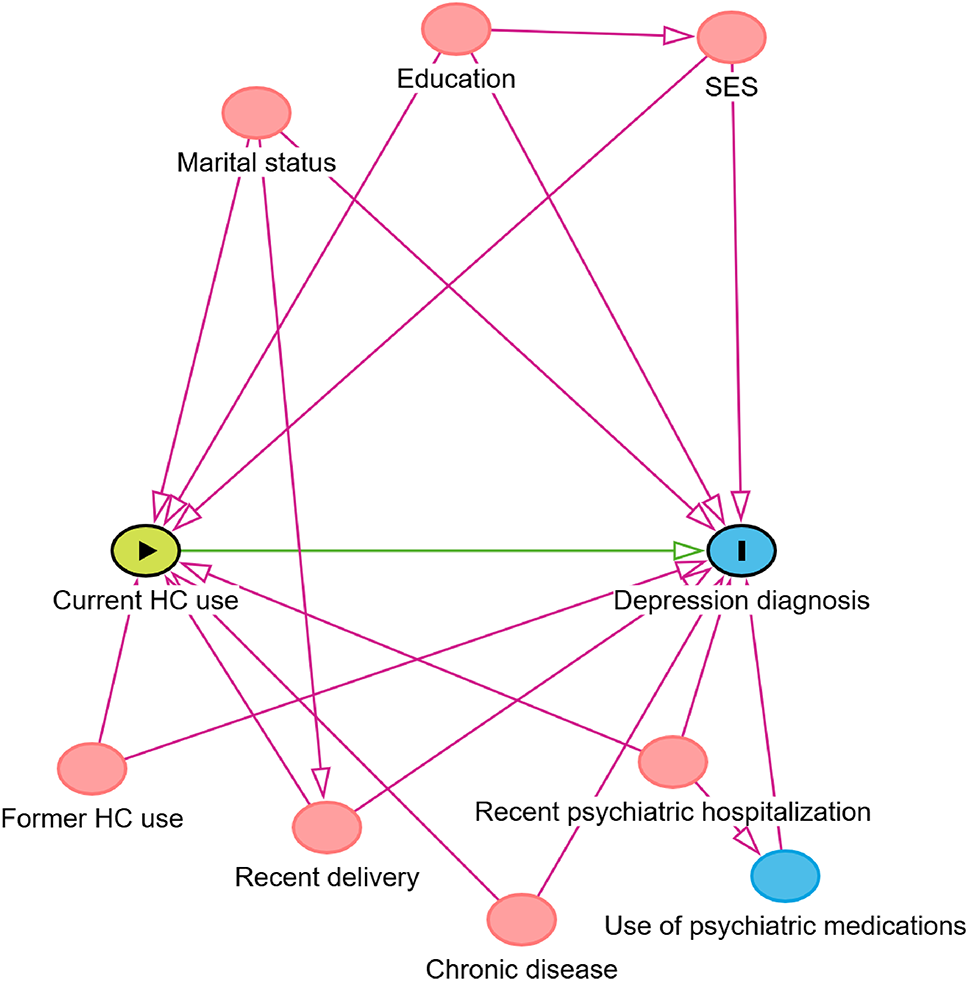
In addition to revealing sources of bias for transparency, the directed acyclic graph aids in understanding causality of the measured associations. In theory, if our DAG correctly defines the paths between the exposure and outcome, observed associations shown in Fig. 3 would be estimates of causal effects. However, remaining bias depends on non-included biasing paths, such as bias introduced by missing information of LNG-IUDs and unmeasured confounders, including smoking and blood donation [25].
To the best of our knowledge, the present study is the first to assess the associations between hormonal contraceptive use and anaemia on a nationwide scale. A key strength of our study was the use of Finnish national registry data, allowing for a highly representative sample including over half of the fertile-aged female population of Finland. This allowed for a study design with high statistical power, that also accounts for possible regional differences in prescribing patterns.
Use of HC have been associated with increased risk of breast cancer and thrombosis, risks that should be clearly communicated to patients to support informed decision-making based on individual risk that considers genetic factors, age and lifestyle choices [26, 27]. Potential adverse effects must be evaluated in the context of the benefits HC offer, including improved quality of life in women suffering heavy or painful menstruation, decreased risk of ovarian cancer, and reproductive autonomy as well as reduced maternal mortality. Our results add to the existing knowledge on health effects of hormonal contraception use and expand knowledge on prevention of iron deficiency anaemia as set out by the World Health Organization’s framework for accelerating anaemia reduction. Furthermore, results can help decision-makers when designing family planning programmes, reimbursement rights of hormonal contraception, and national care guidelines. They are also of value at grassroots level by physicians in primary care settings and specialist gynaecological practices to support clinical decision making.
In conclusion, use of hormonal contraception is related to reduced odds of anaemia in women of reproductive age. The benefits of hormonal contraception extend beyond that of contraception and should be considered by policy-makers to promote women’s health and gender equity.


Comments (0)