
Remember me
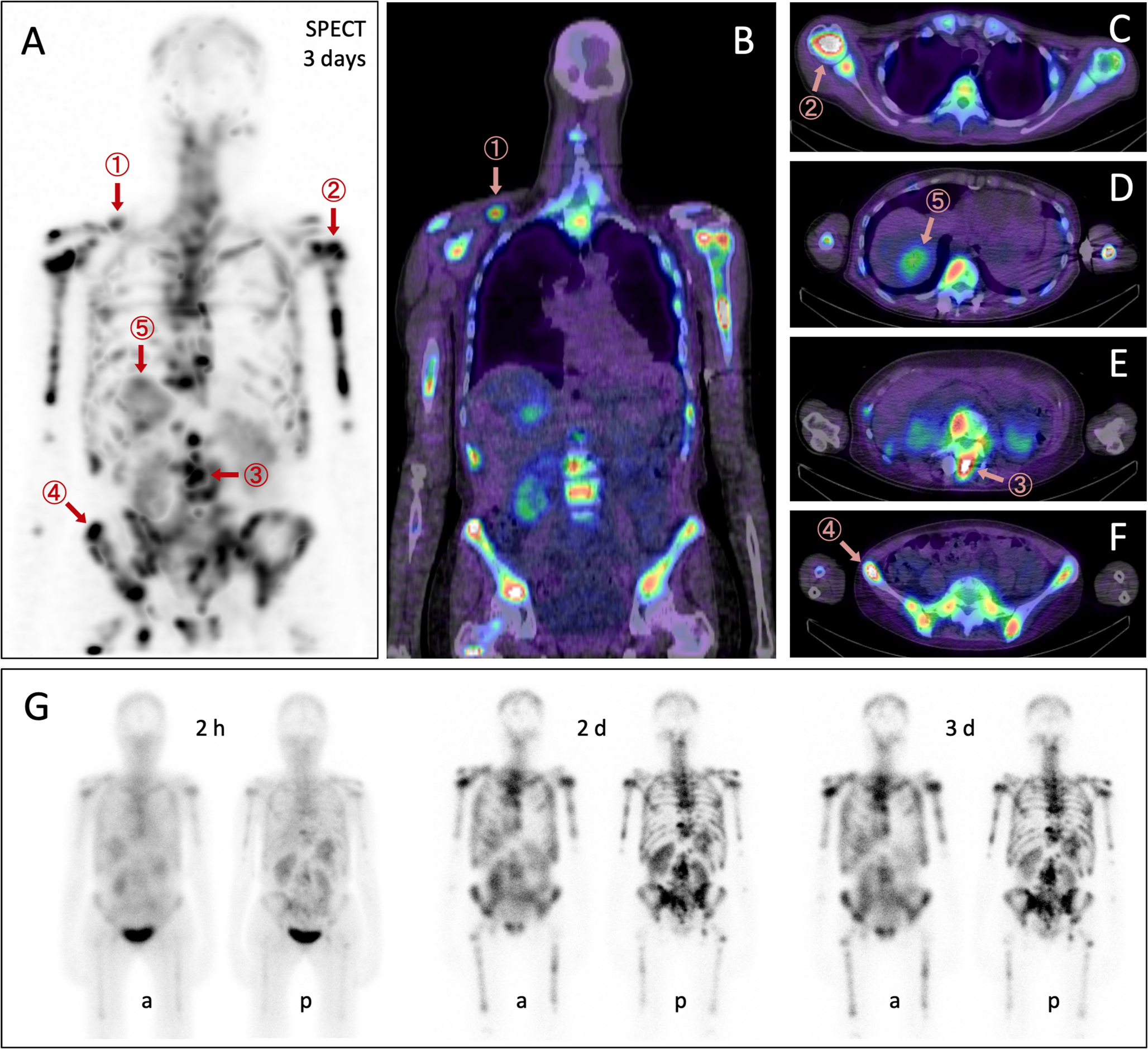
The final research sample comprised a total of 23 participants (median age 42 years; age range 17–61 years; 3 [13%] males and 20 [87%] females) (Fig. 1). Among them, 16 participants underwent [18F]FDG PET/CT imaging within 14 days. The pathological subtypes included papillary carcinoma (n = 22) and follicular carcinoma (n = 1). Among all patients, 5 cases (22%) were classified as high initial risk stratification, while the remaining 18 cases (78%) were categorized as intermediate initial risk stratification. The detailed baseline lymph node status (number and ratio) for the intermediate-risk group is provided in Supplementary Table 1. All subjects received neck ultrasonography (US) and chest computed tomography (CT) examinations following the standard imaging protocols. The median time interval between the conventional imaging and FAPI scans was 8 days (range, 2–36 days). During the follow - up period (median 15.5 months, ranging from 8 to 32 months) subsequent to undergoing [18F]AlF-NOTA-FAPI-04 PET/CT, their serum Tg and Tg-Ab levels were evaluated. Based on the PET/CT imaging and US results, histological findings were obtained from 7 participants. Six cases were confirmed to be malignant, while in the other case, no recurrent lesions were detected. Out of the 7 participants with histological outcomes, one participant underwent lymph node puncture biopsy followed by radiofrequency ablation, and six participants had cervical lymph node dissection, with one of them also having an additional abdominal wall mass excision. Six participants were classified as having positive malignancy by 131I whole - body imaging, US, or CT during the follow - up. Ten participants showed no evidence of malignant disease in PET/CT and standard-of- care imaging. For detailed information, please refer to Table 1.
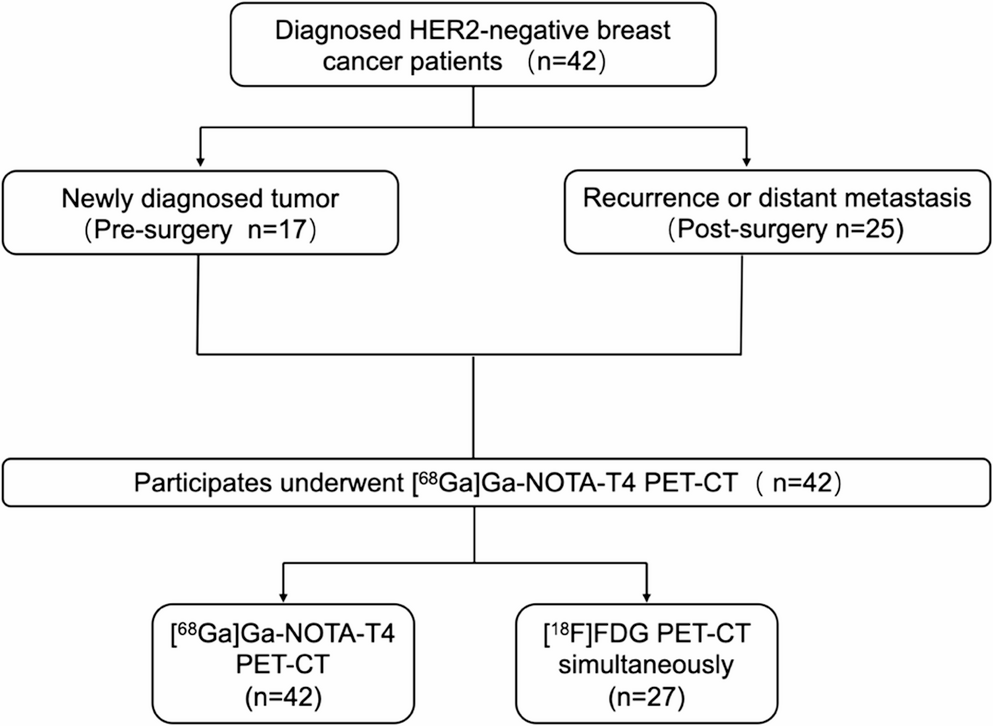
Fig. 1
Flow diagram shows participant selection details.
Table 1 Participant characteristicsAnalysis on the visualization of recurrent DTC lesions in [18F]AlF-NOTA-FAPI-04 PET/CT imagingIn 11 participants (64%), a total of 19 positive lesions were identified via [18F]AlF-NOTA-FAPI-04 PET/CT, all of which were confirmed to be malignant. The mean SUVmax and TBR were 5.23 ± 4.89 and 5.07 ± 4.62, respectively. Specifically, one case (5% of the total) was a local recurrence, which subsequently underwent radiofrequency ablation. The SUVmax and TBR for this case were 15.11 and 16.23, respectively. Cervical lymph nodes were present in seven lesions (37%), with mean SUVmax and TBR of 6.47 ± 4.21 and 6.12 ± 3.98, respectively. Pulmonary metastases were observed in five lesions (26%), and the average SUVmax and TBR were 3.01 ± 4.05 and 5.21 ± 6.12, respectively. It is worth noting that three of these pulmonary metastases showed no abnormal uptake, with diameters of 4.2 mm, 5.2 mm, and 5.2 mm, respectively. Detailed information on pulmonary lesions (size, location, SUVmax, etc.) has been provided in Supplementary Table 2. Splenic metastases were detected in four lesions (21%), with mean SUVmax and TBR of 2.64 ± 0.71 and 2.17 ± 0.52, respectively. The four splenic lesions exhibited significant enlargement on follow-up CT scans at 12 months, thereby confirming their metastatic nature. Additionally, there was one case (5%) of abdominal wall lesions, with SUVmax and TBR of 4.32 and 2.68, respectively (Fig. 2), and one case (5%) of mediastinal lymph node metastases, having SUVmax and TBR of 10.02 and 8.4, respectively. Remarkably, all seven metastatic cervical lymph nodes were small lesions, with a mean diameter of 5.9 ± 1.4 mm. These lesions were not detected by traditional imaging modalities such as US, CT and [18F]FDG PET/CT. Pearson correlation analysis revealed that the correlation coefficients of SUVmax and TBR for all FAPI - avid lesions with the lesion diameter were 0.241 and 0.308, respectively. The corresponding P - values were 0.335 and 0.214, respectively, indicating no significant statistical differences. The results of the visualization of recurrent DTC lesions in [18F]AlF-NOTA-FAPI-04 PET/CT are presented in Supplementary Table 3.
Fig. 2
A 37-year-old female with PTC after total thyroidectomy and two courses of 131I adjuvant therapy(cumulative activity: 11.1 GBq), managed with TSH suppression. Elevated Tg was detected 8 months post-131I adjuvant therapy. (a–d) [18F]FDG PET/CT demonstrated no pathological uptake. (e–h) [18F]AlF-NOTA-FAPI-04 PET/CT identified a 8.1-mm nodule with intense tracer uptake (SUVmax = 4.3) in the anterior abdominal wall (arrows), with no other lesions detected. Ultrasound (US) suggested bilateral cervical lymphadenopathy. Surgical resection of the abdominal nodule and selected lymph nodes (right level VA, left level II) confirmed metastatic carcinoma in the abdominal lesion but no malignancy in the lymph nodes.
We analyzed associations between FAPI- SUVmax and six clinicopathological parameters: Tg-Ab level, Tg-Ab, suppressed-Tg level, suppressed-Tg, TSH level, and risk stratification of recurrence. Univariate analysis revealed no significant associations between FAPI- SUVmax and any of the investigated parameters. Continuous variables (Tg-Ab level, suppressed-Tg level, TSH level) showed weak Spearman correlations with FAPI-SUVmax (ρ = −0.12 to −0.21, P > 0.47). Binary variables (Tg-Ab, suppressed-Tg) demonstrated no significant differences in FAPI-SUVmax between groups (Mann-Whitney U test, P = 0.34–0.62). Risk stratification also showed no FAPI-SUVmax variation (Kruskal-Wallis H test, P = 0.73) (Supplementary Table 4).
Comparative analysis of uptake in histopathological benign versus malignant lesionsFive participants underwent paired [18F]AlF-NOTA-FAPI-04 and [18F]FDG PET/CT imaging, followed by surgical resection. A total of 16 lesion histopathological findings were obtained. In total, there were 4 malignant lesions, consisting of 3 metastatic cervical lymph nodes and 1 abdominal wall metastasis. All these malignant lesions demonstrated FAPI - avidity. One of the cervical lesions exhibited mild [18F]FDG uptake, with SUVmax and TBR of 3.5 and 1.45, respectively. The remaining 11 lesions were reactive hyperplasia of cervical lymph nodes. None of these 11 lesions showed [18F]AlF-NOTA-FAPI-04 uptake, and 6 of them had ambiguous [18F]FDG uptake (Fig. 3). In FAPI imaging, the median SUVmax for pathologically negative and positive lesions were 1.2 and 4.7 (P = 0.004), respectively, and the median TBR were 0.9 and 4.0 (P = 0.006), respectively. In contrast, in [18F]FDG imaging, the median SUVmax for pathologically negative and positive lesions were 2.1 and 2.2 (P = 0.23), respectively, and the median TBR were 1.3 and 1.3 (P = 0.099), respectively (Table 2). It is noteworthy that in Participant 1 (Fig. 4) (who underwent paired FAPI and FDG imaging) and Participant 18 (who underwent FAPI imaging alone), two metastatic lymph nodes were pathologically confirmed in the left cervical region level II and the right supraclavicular region, respectively, whereas [18F]AlF-NOTA-FAPI-04 imaging demonstrated only one abnormal uptake focus at the corresponding sites.
Fig. 3
A 20-year-old female with PTC post-total thyroidectomy and two courses of 131I adjuvant therapy (cumulative activity: 11.1 GBq), under TSH suppression. Elevated Tg was noted 2 years post-131I adjuvant therapy. (a–d) [18F]FDG PET/CT detected a hypermetabolic lymph node (SUVmax = 6.1) in the right level II cervical region (arrows). (e–h) [18F]AlF-NOTA-FAPI-04 PET/CT showed no tracer avidity at the corresponding site (SUVmax = 1.3). Pathological examination of resected lymph nodes (right level II, left levels II and III) confirmed reactive hyperplasia.
Fig. 4
A 57-year-old female with PTC following total thyroidectomy and two courses of 131I adjuvant therapy (cumulative activity: 9.62 GBq), under thyroid-stimulating hormone (TSH) suppression. Elevated Tg-Ab were observed 12 months post-131I adjuvant therapy. (a–d) [18F]FDG PET/CT showed no abnormal uptake. (e–h) [18F]AlF-NOTA-FAPI-04 PET/CT revealed a 4.1-mm high uptake lymph node (SUVmax = 5.1) in the left level II cervical lymph node region (straight arrows). Subsequent bilateral neck dissection confirmed two metastatic lymph nodes at this location. The three FAPI-avid foci (curved arrows, h) within the left thorax and upper mediastinum have been identified as inflammatory lesions: one in the left inferior pulmonary lobe and two at the left sternoclavicular joint.
Table 2 Comparative uptake in pathologically verified lesions: malignant versus benign cohortsComparison of [18F]AlF-NOTA-FAPI-04 and [18F]FDG uptake in recurrent lesionsBased on the histopathological and clinical follow-up findings, a total of 16 lesions in 6 participants who underwent [18F]AlF-NOTA-FAPI-04 and [18F]FDG PET/CT scans were confirmed to be malignant. Among these, 3 pulmonary lesions and 1 metastatic cervical lymph node exhibited no uptake of either tracer, while 12 lesions showed FAPI - avidity. [18F]FDG PET/CT failed to detect 12 lesions; specifically, only 2 lesions had uptake, with one being a cervical lymph node and the other a mediastinal lymph node. The median values of SUVmax and TBR for the 12 aforementioned FAPI - avid lesions were 3.5 and 2.8, respectively, both of which were higher than the measured values in [18F]FDG imaging (SUVmax = 2.0 and TBR = 1.2), with the P-values being 0.002 and 0.001, respectively. In 4 cases of cervical lymph node metastases, the median values of FAPI parameters were higher than FDG (SUVmax: 6.0 vs. 2.2; TBR: 6.4 vs. 1.2), but without statistically significant differences (both P = 0.0625). For the two pulmonary lesions, the average SUVmax were 1.5 and 0.5, respectively, and the average TBR were 2.3 and 0.7, respectively. In the case of one abdominal wall metastasis, the SUVmax were 4.3 and 2.3, respectively, and the TBR were 2.6 and 1.3, respectively. The median SUVmax of 4 splenic metastases were 2.6 and 1.9 (P = 0.37), respectively, and the mean TBR were 2.1 and 1.1 (P = 0.12), respectively. For 1 mediastinal lymph node metastasis, the SUVmax were 10.02 and 8.4, respectively, and the TBR were 8.4 and 1.5, respectively (Table 3).
Table 3 Comparison of [18F]AlF-NOTA-FAPI-04 and [18F]FDG uptake in recurrent lesionsComparison of diagnostic efficacy of paired [18F]AlF-NOTA-FAPI-04 and [18F]FDG imagingIn total, 16 participants underwent paired [18F]AlF-NOTA-FAPI-04 and 18F-FDG imaging, with histopathological or clinical follow-up results available for 30 lesions. For [18F]FDG PET/CT, the recurrent DTC lesions had a total of 2 true positives, 7 false positives, 7 true negatives, and 14 false negatives. In contrast, for [18F]AlF-NOTA-FAPI-04 PET/CT, there were 12 true positives, 2 false positives (comprising 1 benign bone lesion and 1 case of arthritis), 12 true negatives, and 4 false negatives (including 3 pulmonary metastases and 1 cervical lymph node metastasis). Based on the lesion analysis, the diagnostic efficacy of the two imaging modalities was evaluated. The lesion sensitivity of [18F]AlF-NOTA-FAPI-04 PET/CT (75% [12/16] versus 13% [2/16]; P = 0.002), specificity (86% [12/14] versus 43% [6/14]; P = 0.125), and accuracy (80% [24/30] versus 27% [8/30]; P < 0.001) were all higher than those of [18F]FDG PET/CT. However, no significant statistical difference was observed in terms of specificity. When considering participant - based analysis, there was significant difference in sensitivity ([18F]AlF-NOTA-FAPI-04 PET/CT: 100% [7/7 vs. 18F-FDG PET/CT: 14% [1/7]; P = 0.003) between the two imaging methods. Nevertheless, there were no evidence indicating a difference in specificity (78% [7/9] versus 89% [8/9]; P = 1) and accuracy (88% [14/16] vs. 56% [9/16]; P = 0.56) (Table 4).
Table 4 Diagnostic performance of [18F]AlF-NOTA-FAPI-04 and [18F]FDG PET/CT
Comments (0)