
Remember me
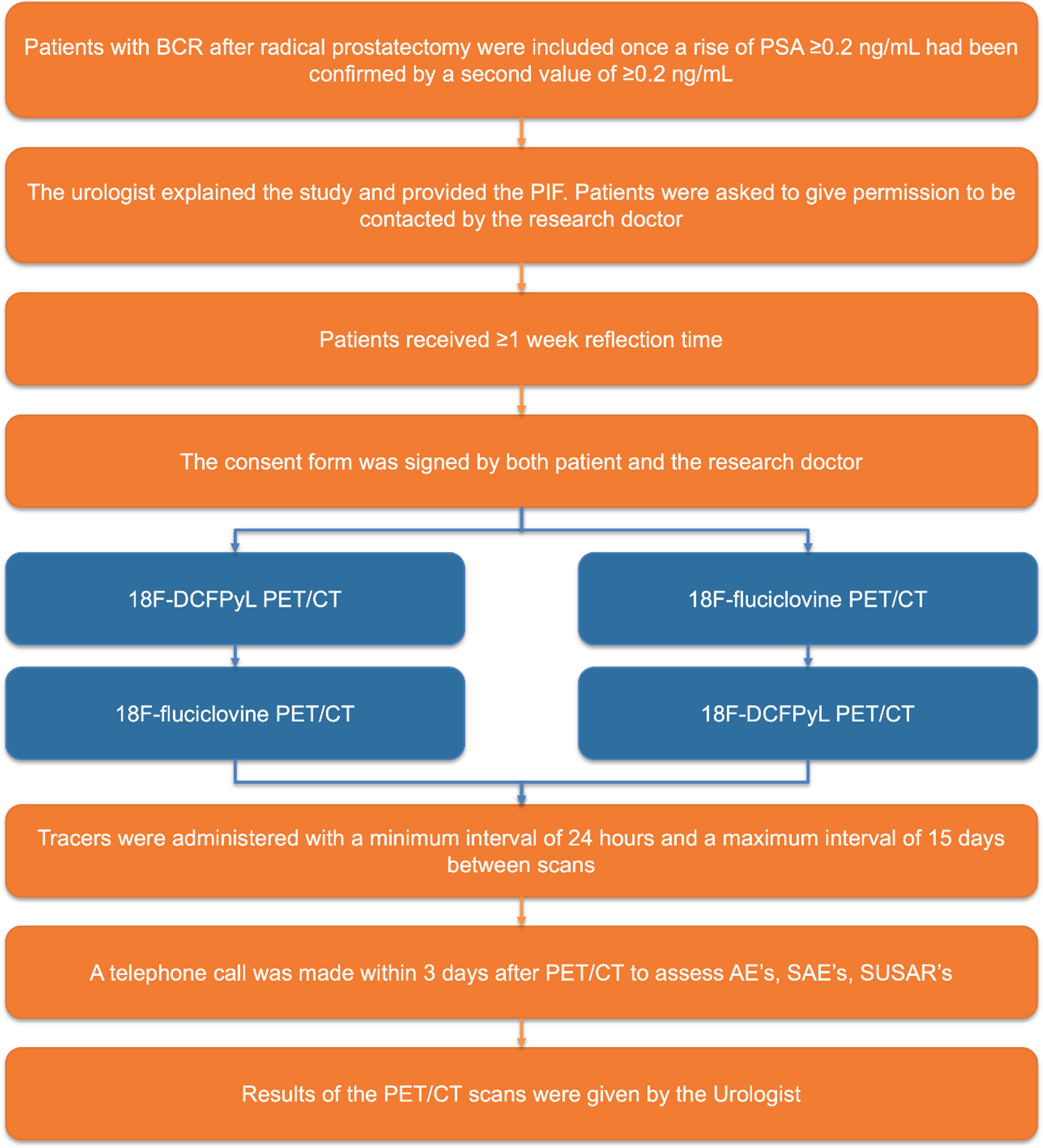
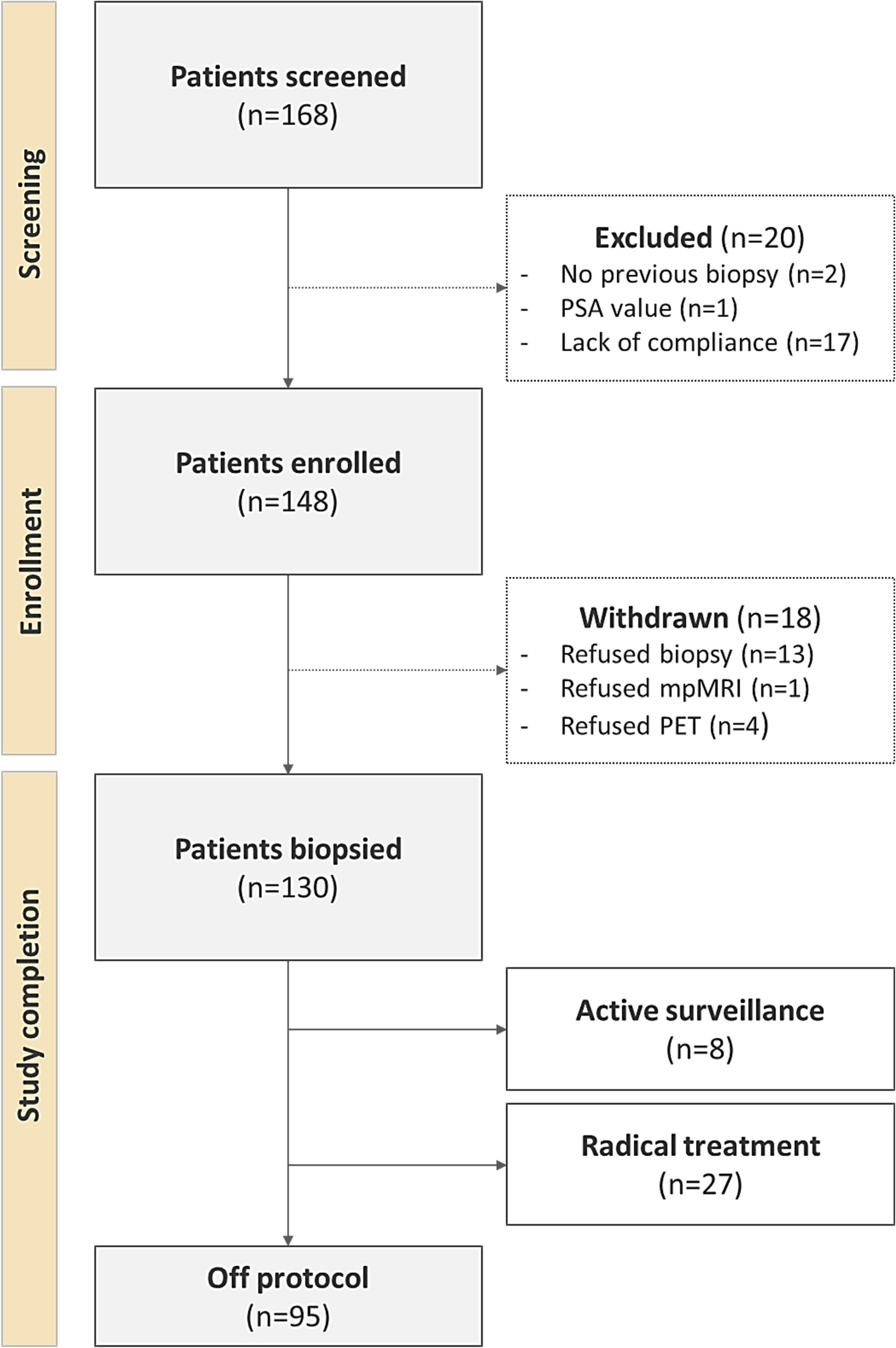
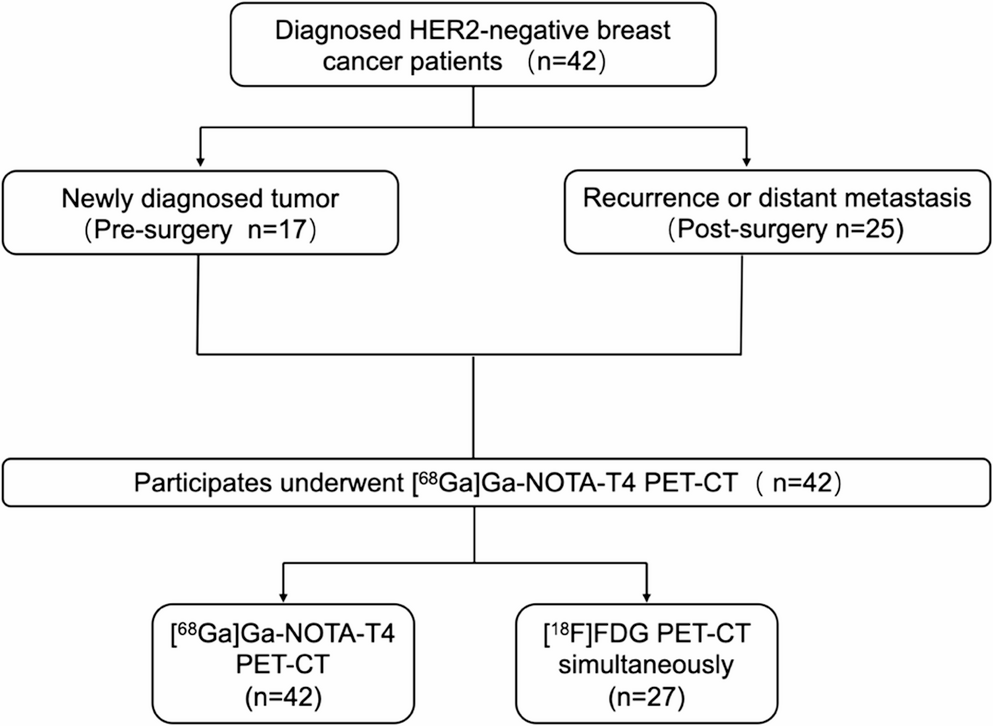
This prospective, single-center, open-label, non-randomized study was conducted at the Amsterdam University Medical Center (UMC). It was designed as a head-to-head comparison of the detection rates of two PET tracers in patients with BCR with low PSA levels (0.2-2.0 ng/mL), following RARP (Fig. 1). The study protocol was approved by the medical ethics committee of the Amsterdam UMC (reference number 2021.0149), and all patients provided written informed consent. Patients were enrolled between January 2022 and April 2024.
Fig. 1
Study chart. BCR = biochemical recurrence; PSA = prostate-specific antigen; PIF = patient information form; PET/CT = positron emission tomography/computed tomography; AE = adverse event; SAE = serious adverse event; SUSAR = suspected unexpected serious adverse reaction
Patient populationEligible patients were adult men (≥ 18 years) with histologically confirmed PCa who had undergone RARP, with or without an extended pelvic lymph node dissection (ePLND). Only patients with a PSA level between 0.2 and 2.0 ng/mL were included. BCR was defined as a PSA level ≥ 0.2ng/mL on two consecutive measurements or a rising PSA [3]. Key exclusion criteria included histopathological lymph node positivity (pN1) after ePLND, prior salvage therapies, ADT and other concurrent malignancies.
For all patients, comprehensive clinical, biochemical, radiological, and pathological information was collected. Clinical variables included age and clinical tumor stage assessed by digital rectal examination (DRE). Biochemical data comprised PSA at initial diagnosis, most recent PSA at the time of performing PET/CT, and PSA recurrence dynamics (e.g., PSA nadir, PSA level at recurrence, PSA doubling time). Histopathological variables encompassed the percentage of positive biopsy cores (with targeted cores pooled and reported as one positive biopsy core within systematic sets), International Society of Urological Pathology (ISUP) Grade Group after biopsy and RARP [14]. Additional variables included histopathological TNM stage post-surgery and surgical margin status. Imaging data comprised PET/CT specifics, including date, radiopharmaceutical, injected dose (MBq), scan trajectory, reconstruction parameters and imaging findings. Risk stratification was performed according to the European Association of Urology (EAU) classification system [3].
Adverse events (AEs), serious adverse events (SAEs), and suspected unexpected serious adverse reactions (SUSARs) were monitored and recorded according to the protocol-defined criteria.
Imaging procedureAll patients underwent both [18F]Fluciclovine and [18F]DCFPyL PET/CT scans using standardized protocols. The interval between scans ranged from a minimum of 24 h to a maximum of 15 days. Scans were performed and interpreted in a non-fixed order and the identity of the administered tracer was not blinded due to the open-label design.
For [18F]Fluciclovine, patients fasted for 4 h prior to tracer administration. The [18F]Fluciclovine tracer was produced and delivered by GE Healthcare. A standard activity of 370 MBq (± 10%) was injected intravenously while the patient was positioned on the PET/CT scanner bed. PET imaging commenced 3–5 min post-injection (target 4 min). Acquisition was performed from mid-thigh to skull base at 3 min per bed position, resulting in a total scan time of approximately 24 min. Scans were performed in accordance with the procedure guidelines [15].
[18F]DCFPyL was synthetized via direct radiofluorination at an on-site cyclotron facility. Whole-body PET was performed 120 min (± 15 min) after intravenous injection of 330 MBq [18F]DCFPyL. Imaging was acquired from mid-thigh to the base of the skull at 4 min per bed position. The total acquisition time averaged 30 min. No fasting was required and no diuretics were administered prior to imaging. Scans were conducted in line with the imaging guidelines for PSMA PET/CT [16].
For both tracers, PET was performed using an European Association of Nuclear medicine Research LTd (EARL) calibrated hybrid Philips Ingenuity TF scanner and combined with a low-dose CT (30–120 mAs; 120 kV). All images were corrected for decay, scatter, random coincidences and photon attenuation. Images were reconstructed using the EARL specifications on the quantitative reads of clinical PET/CT studies [17].
Image evaluationA nuclear medicine physician initially reviewed both PET/CT scans on-site, without blinding to clinical data. Therapeutic decisions were based on the combined clinical and imaging findings. These decisions were typically made in consultation with a multidisciplinary team consisting of urologists, radiation oncologists, nuclear medicine physicians and medical oncologists. Scan interpretation was in line with the PROMISE criteria [18]. A lesion was considered positive when focal uptake was visually higher than surrounding background activity and not attributable to physiological uptake or benign processes. Supportive anatomical substrate on low-dose CT was used when applicable. No minimum lymph node size threshold was applied and small nodes were scored as positive if uptake was clearly focal and exceeded local background. Equivocal findings were scored as negative.
For study analysis, all PET/CT scans were anonymized and independently evaluated by three nuclear medicine physicians. Readers were blinded to clinical information and to the results of the other scan. A mix of [18F]DCFPyL and [18F]Fluciclovine scans was presented to the readers in random order. Scans from the same patient were not read consecutively. Each reader assessed the presence of PCa in predefined anatomical regions, including the prostate bed (miTr), pelvic lymph nodes (miN1), extra-pelvic lymph nodes (miM1a), bone lesions (miM1b), and other organs (miM1c). These sites were scored as positive or negative for suspected BCR. Discrepancies between the three readers were resolved by consensus, defined as majority agreement (≥ 2 of 3 readers). Only the blinded independent readings were used for the analysis. The original on-site interpretations, conducted with knowledge of all clinical information, were not incorporated or analyzed for the study outcomes.
OutcomesThe primary outcome was to compare the per-patient detection rates of [18F]Fluciclovine and [18F]DCFPyL PET/CT, independent of follow-up data. Secondary outcomes included detection rates across anatomical regions, detection rates stratified by PSA level (i.e., 0.2–0.5, 0.51–1.0, and 1.01–2.0 ng/mL), and the assessment of inter-observer agreement.
Statistical analysisSample size was calculated using a one-sided McNemar test (α = 0.05, power = 80%), requiring 50 patients to detect a 30% difference in detection rates between tracers. Baseline characteristics were summarized descriptively. Detection rates were reported on a per-patient basis (≥ 1 PET-positive anatomical region) and per-region basis (i.e., prostate bed, pelvic lymph nodes, extra-pelvic lymph nodes, bone, visceral). Positivity was defined by PET-positive findings regardless of pathology or imaging/clinical follow-up. Paired comparisons between tracers were performed using McNemar’s test. To control for multiplicity, hypothesis testing was limited to the primary and region-specific endpoints.
Detection rates were also summarized by PSA level at PET/CT. These subgroup analysis were exploratory and are presented descriptively. Inter-observer agreement for each tracer was assessed using Fleiss’ kappa, interpreted according to the Landis and Koch classification: 0.00 (poor), 0.01–0.20 (slight), 0.21–0.40 (fair), 0.41–0.60 (moderate), 0.61–0.80 (substantial), and 0.81–1.00 (almost perfect) reproducibility [19]. Bootstrapped 95% confidence intervals were computed for Fleiss’ kappa statistics to estimate inter-observer agreement uncertainty.
A p-value ≤ 0.05 was considered statistically significant. All analyses were performed in RStudio (version 4.4.3).
Comments (0)