
Remember me
The study included 218 participants (65 CU, 115 MCI, 38 DEM). Based on visual read of late-phase amyloid PET, 123 were classified as amyloid-positive (Aβ +), 93 as amyloid-negative (Aβ–), and 2 as borderline. The borderline cases were excluded from stratified analyses but retained in models including the full cohort. Among Aβ+ participants, 11 were CU, 79 had MCI, and 33 had dementia. In the Aβ– group, 53 were CU, 35 had MCI, and 5 had dementia. Aβ+ participants were older and had lower MMSE scores than Aβ– participants (p < 0.001).
Mean age of the total sample was 70.9 ± 7.4 years, and 43.6% were women. Average education was 13.7 ± 4.1 years. Baseline MMSE was 25.7 ± 4.1, with lower scores in Aβ + (24.4 ± 4.5) than in Aβ– participants (27.5 ± 2.7). Centiloid values differed markedly between groups (Aβ + : 76.1 ± 32.1; Aβ–: –0.4 ± 12.6), consistent with amyloid status classification.
APOE genotype data were available for 140 participants (64%), of whom 47 carried one ε4 allele and 8 carried two. ARWMC ratings were available for 155 participants (71%) and averaged 6.1 ± 4.6 on the Wahlund scale (range 0–30). Compared with Aβ– individuals, Aβ+ participants were older, had fewer years of education, and showed lower MMSE and higher Centiloid values. Full demographic and imaging summaries are presented in Table 1.
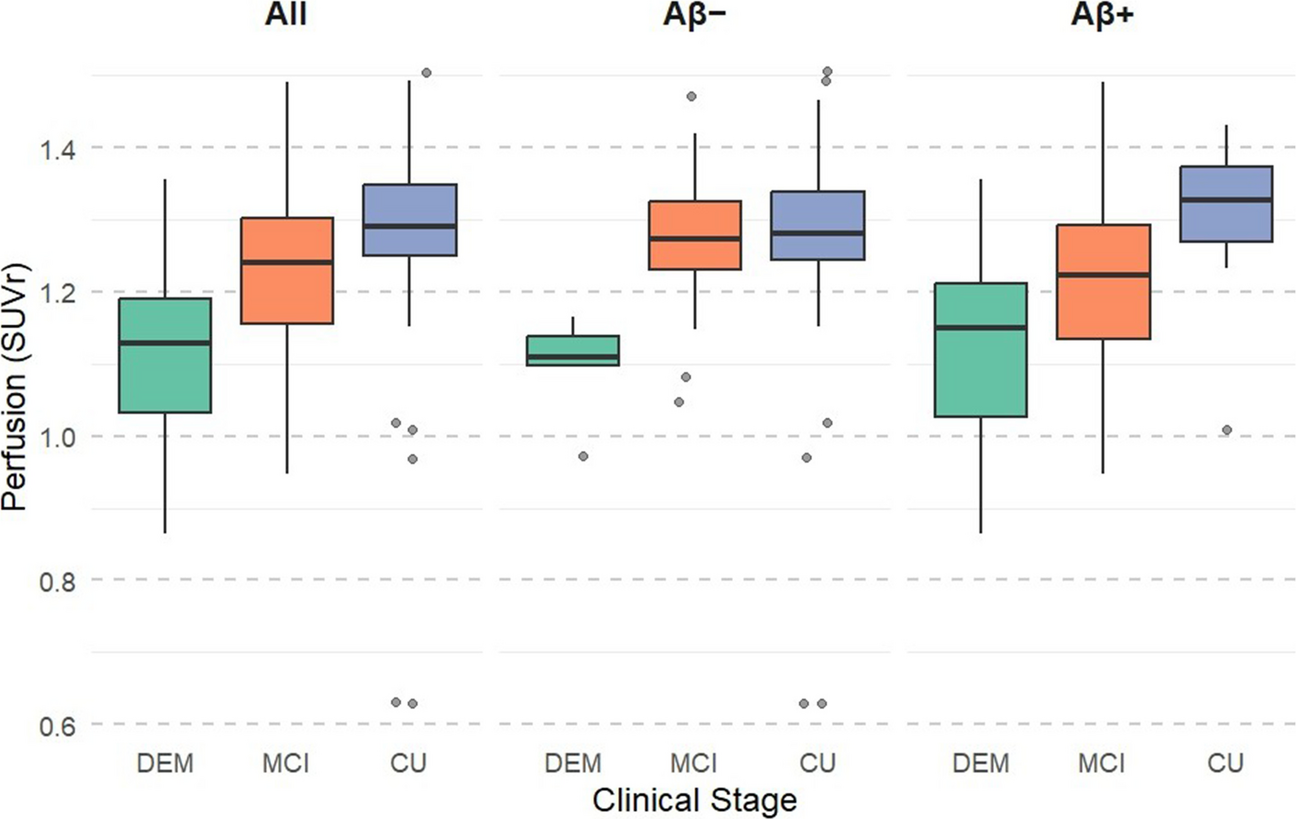
Perfusion differences across clinical groupsAcross the full cohort (CU: n = 65, MCI: n = 115, DEM: n = 38), descriptive statistics showed distinct mean perfusion values in each group: CU = 1.28 ± 0.13, MCI = 1.24 ± 0.11, and DEM = 1.13 ± 0.12. A one-way ANOVA revealed a significant overall difference in perfusion across clinical stages [F(2, 214) = 21.09, p < 0.001]. Post-hoc comparisons using Tukey’s HSD test indicated that participants with dementia had significantly lower perfusion compared with both CU (mean difference = –0.15, 95% CI [–0.21, –0.10], p < 0.001) and MCI (mean difference = –0.11, 95% CI [–0.16, –0.06], p < 0.001). Additionally, perfusion in MCI was significantly lower than in CU (mean difference = –0.05, 95% CI [–0.09, –0.002], p = 0.036).
To assess whether this pattern differed by amyloid status, we repeated the analysis separately for Aβ– (n = 93) and Aβ+ (n = 123) subgroups. Among Aβ– participants, perfusion differed significantly across clinical stages [F(2, 90) = 5.87, p = 0.004]. Post-hoc tests showed that participants with dementia had significantly lower perfusion compared with both CU (mean difference = –0.19, 95% CI [–0.32, –0.06], p = 0.003) and MCI (mean difference = –0.18, 95% CI [–0.31, –0.05], p = 0.005), with no significant difference between CU and MCI.
In the Aβ + group, perfusion also varied significantly by clinical stage [F(2, 120) = 9.63, p < 0.001]. Participants with dementia had lower perfusion compared with CU (mean difference = –0.16, 95% CI [–0.25, –0.06], p = 0.001) and MCI (mean difference = –0.09, 95% CI [–0.14, –0.03], p = 0.001). Again, no significant difference was observed between CU and MCI in this subgroup.
In addition to within-group analyses, we compared overall perfusion between Aβ + and Aβ– participants across the full cohort. Aβ+ individuals showed significantly lower mean perfusion (1.21 ± 0.12) compared with Aβ– individuals (1.27 ± 0.13), t(216) = 3.43, p = 0.0007. Detailed group means and ANOVA results are summarized in Supplementary Table S4. Figs. 1, 2 and 3
Fig. 1
Perfusion by clinical stage and amyloid status. Boxplots show early-phase PET perfusion values (meta-ROI SUVr) across diagnostic groups:CU, MCI, DEM. The left panel displays values for the full sample, while the middle and right panels show results stratified by amyloid PET status (Aβ − and Aβ +, respectively). Perfusion was lowest in the dementia group and progressively higher in MCI and CU, consistent with a decline in cerebral perfusion across the clinical continuum of cognitive impairment. This pattern was more pronounced in Aβ+ individuals
Fig. 2
Baseline relationship between perfusion and MMSE across amyloid subgroups. Scatterplots show the positive association between early-phase PET perfusion values and baseline MMSE in the full cohort (left), Aβ- (middle), and Aβ + (right) groups. Pearson correlation coefficients (r) and p-values are displayed in each panel. The association was strongest in the Aβ + group (r = 0.37, p < 0.001), but remained significant in both groups
Fig. 3
Predicted MMSE trajectories over time based on perfusion and amyloid status. Participants were stratified into low and high perfusion groups using a data-driven cut-off (Youden index) based on early-phase PET perfusion values. Cognitive trajectories (MMSE) were estimated using linear mixed-effects models adjusted for age, gender, and years of education. Solid lines represent Aβ+ individuals, and dashed lines represent Aβ− individuals. Shaded areas represent 95% confidence intervals. Individuals with higher perfusion showed slower cognitive decline, but this effect was evident primarily in the Aβ + group
Perfusion and cognitionThe relationship between perfusion, as measured by early-phase amyloid PET in AD-related meta-ROI regions, and cognitive function, assessed using the MMSE, was examined cross-sectionally using correlation analyses. Across the entire cohort, a significant positive Pearson correlation was observed (r = 0.39, p < 0.001), indicating that higher perfusion levels were associated with better cognitive performance.
This relationship was further supported by an exploratory linear regression (β = 12.83, SE = 2.04, p < 0.001), which explained a modest proportion of variance (R2 = 0.16), consistent with a moderate linear association.
When analyses were repeated within amyloid subgroups, the association was weaker in Aβ– participants (r = 0.26, p = 0.012) and stronger in Aβ+ participants (r = 0.37, p < 0.001). As a comparison, higher amyloid burden (Centiloid) was inversely related to baseline MMSE (r = –0.32, 95% CI [–0.43, –0.21], p < 0.001; see Supplementary Section 5).
In addition to cognitive performance, we also examined the biological relationship between perfusion and amyloid burden. Early-phase perfusion SUVr showed a modest but significant inverse association with Centiloid values (Spearman ρ = –0.26, p = 0.0001; Pearson r = –0.23, p = 0.0006), consistent with partially independent contributions of amyloid burden and perfusion. Linear regression indicated a negative slope between Centiloid and perfusion (β = –0.0006, p = 0.0006; Adj. R2 = 0.05), while classification analysis yielded AUC = 0.68 for distinguishing amyloid-positive cases (≥ 20 CL). These findings are illustrated in Supplementary Figure S1 and summarized in Supplementary Tables S13–S14.
Longitudinal associations between perfusion and MMSETo assess how baseline perfusion relates to cognitive trajectories, longitudinal linear mixed-effects (LME) models were fitted using repeated MMSE scores as the dependent variable. Across the full cohort (Model 1a; 644 observations from 218 participants), higher baseline perfusion was associated with both higher initial MMSE (β = 10.24, p < 0.001) and a slower rate of decline over time (perfusion × time interaction = 4.54, p < 0.001). These effects remained significant after Holm–Bonferroni correction (Tables S5–S6).
When analyses were stratified by amyloid status, the association between perfusion and cognition was mainly evident among amyloid-positive individuals. In the Aβ + subgroup (Model 1c; 377 observations from 123 participants), higher perfusion predicted both better baseline cognition (β = 13.04, p < 0.001) and slower decline (perfusion × time interaction = 5.85, p < 0.001), whereas in the Aβ– subgroup (Model 1b; 258 observations from 93 participants), perfusion related only to baseline MMSE (β = 4.88, p = 0.03) and not to change over time (perfusion × time interaction = –0.48, p = 0.61; Tables S7–S8). Exact R syntax used for Models 1–3 is provided in Table S17.
Including additional biological covariates did not materially alter these associations.In Model 2, which incorporated MRI-based white matter lesion burden (ARWMC), perfusion remained strongly associated with both higher baseline MMSE (β = 13.96, 95% CI [9.25, 18.67], p < 0.001) and slower decline (perfusion × time interaction: 6.17, 95% CI [3.14, 9.20], p < 0.001), whereas ARWMC showed no significant association with cognition (β = 0.01, 95% CI [–0.12, 0.13], p = 0.901; Table S9).
In Model 3, which added APOE genotype, perfusion continued to predict both higher baseline cognition (β = 4.60, 95% CI [0.87, 8.34], p = 0.016) and slower decline over time (perfusion × time interaction = 3.55, 95% CI [1.03, 6.08], p = 0.006). APOE ε4 homozygosity was associated with lower MMSE scores (β = –2.51, 95% CI [–4.55, –0.46], p = 0.017), whereas heterozygous ε4 carriers did not differ significantly from non-carriers. In this smaller subset, the effect of education did not reach significance, likely reflecting reduced statistical power rather than a true absence of association (Table S10).
To test whether the effect of perfusion on cognition differed by amyloid status, we fit an interaction model including perfusion, amyloid positivity, and their interaction term, along with time, age, sex, and education (Table S11; 644 observations from 218 participants). Perfusion was significantly associated with higher baseline MMSE (β = 6.06, p = 0.046), and amyloid positivity with lower MMSE scores (β = –2.11, p < 0.001). The three-way interaction between perfusion, amyloid status, and time was significant (β = 7.16, p = 0.002), indicating that higher perfusion predicted slower cognitive decline over time, particularly in Aβ+ individuals. Although the two-way perfusion × amyloid term did not reach significance (β = 7.45, p = 0.062), the direction was consistent with the subgroup-specific models, supporting a stronger perfusion–cognition association in the amyloid-positive group.
Perfusion and amyloid burden were only modestly correlated (Spearman ρ = –0.26, p = 0.0001; Table S12), indicating partially independent biological contributions. A logistic model using perfusion SUVr to classify amyloid positivity (≥ 20 Centiloids, visual read–consistent threshold) achieved an AUC = 0.68, suggesting limited discriminative accuracy (Table S15). When Centiloid values replaced perfusion as the continuous predictor (Table S13), higher amyloid burden predicted both lower baseline MMSE and faster decline (Centiloid × time: β = –0.02 [–0.03, –0.01], p < 0.001). The Centiloid model showed a slightly better overall fit (AIC = 3410 vs. 3431; ΔAIC ≈ –20; Table S14), yet perfusion exhibited a stronger standardized association with MMSE slope, consistent with complementary rather than redundant predictive value.
In an exploratory extension of this model including continuous Centiloid values and their interaction with perfusion, both perfusion and Centiloid independently predicted baseline MMSE (β = 10.1, p = 0.019; β = –0.016, p = 0.015, respectively). A significant three-way interaction (perfusion × Centiloid × time: β = 0.072, p = 0.041) indicated that the protective effect of higher perfusion on cognitive decline was strongest in individuals with greater amyloid burden (Table S16).
InFinally, Cox proportional-hazards analysis indicated that higher baseline perfusion was associated with a markedly reduced risk of cognitive decline (≥ 3-point MMSE decrease; HR = 0.10 [0.02–0.43], p = 0.0018), while higher Centiloid values predicted increased risk (HR = 1.013 [1.009–1.018], p < 0.0001). Education was protective (HR = 0.90, p < 0.001) (Table 2).
Table 2 Linear Mixed–Effects Models (1a-3): Fixed Effects Summary
Comments (0)