To the best of our knowledge, our study compared for the first time the clinical utility of [177Lu]Lu-PSMA RLT in younger patients relative to older subjects using a matched-pair design. We demonstrate that patients ≤ 65 years old achieve comparable efficacy to matched patients ≥ 70 years old, while younger individuals exhibiting an even more favorable safety profile. These findings support the use of [177Lu]Lu-PSMA RLT regardless of age, which may be of relevance given recent expansion of the indication spectrum.
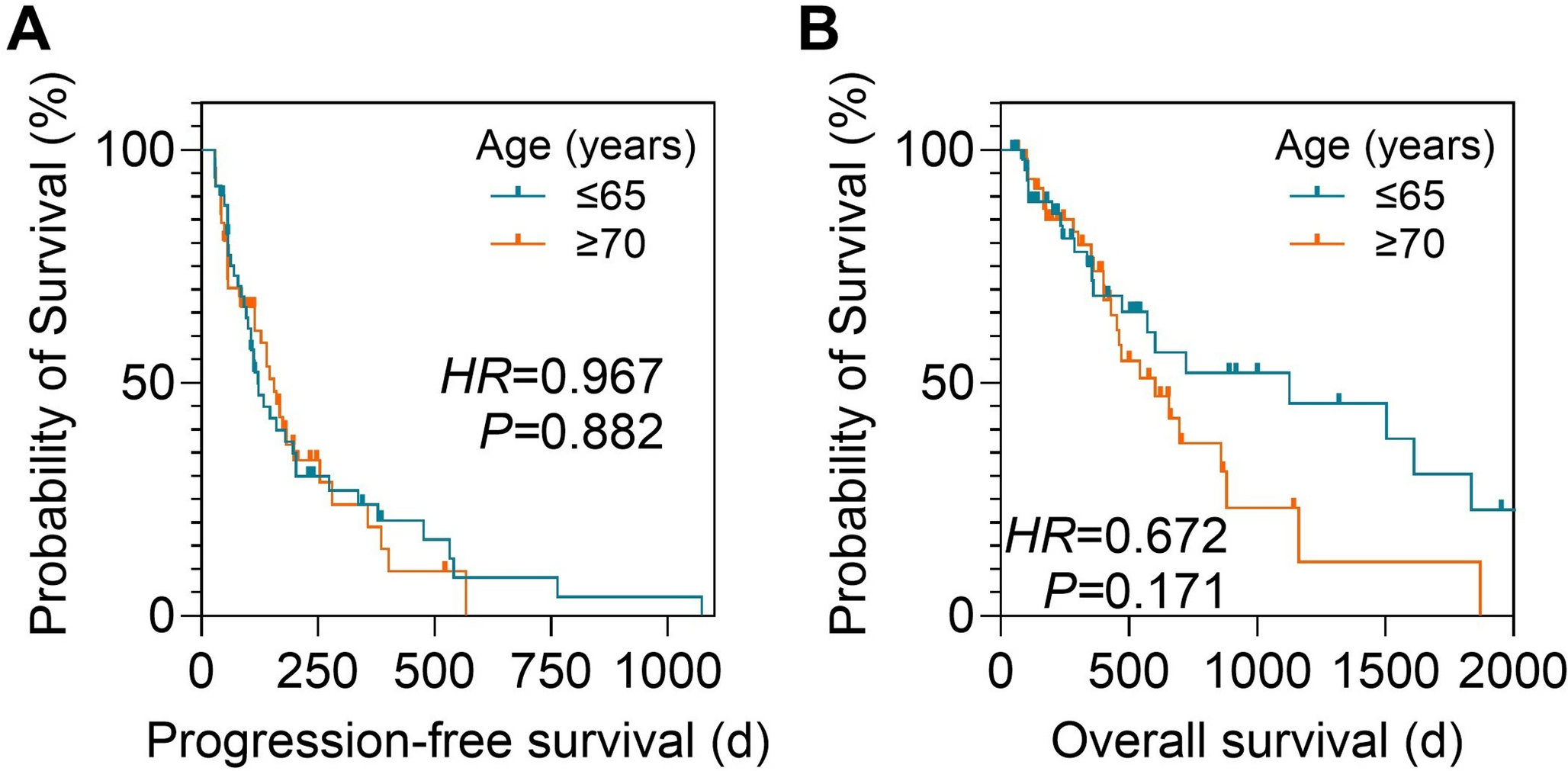
Evidence supporting an earlier use of PSMA-targeted RLT is accumulating rapidly [4,5,6]. The TheraP trial established superiority over the second-line chemotherapy cabazitaxel [4], the PSMAfore trial demonstrated utility in chemotherapy-naïve patients [5], and the PSMAddition trial reported on potential benefit even in a hormone-sensitive setting [6]. As RLT moves earlier in the treatment course, younger patients will increasingly receive this therapy. Yet previous reports have suggested that younger age might predict worse outcomes under RLT [8, 9]. However, these studies were not primarily designed to evaluate treatment efficacy in younger patients and lacked sufficient adjustment for key confounding factors, including Gleason score [8,9,10]. As a result, the reported outcomes may be driven more by underlying tumor aggressiveness than by age itself. Supporting this notion, the time from initial diagnosis to first RLT was also shown to be a significant determinant of outcome in that study [8, 9]. In line, we observed a trend toward higher ALT (P = 0.009) and more frequent hepatic metastases in patients ≤ 65 years (12% vs. 2%; P = 0.051), a known negative prognostic factor [21]. Nonetheless, performing a dedicated match-paired analysis we found no evidence of reduced treatment efficacy in younger patients, as PSA response after two cycles (P = 0.766), PFS (P = 0.882), and OS (P = 0.171) were comparable. Notably, the time from initial diagnosis to first RLT was also similar in both cohorts, also indicating comparable tumor aggressiveness after matching the cohorts.
Our matching criteria (Gleason score, PSA and previous chemotherapy) were selected based on known prognostic significance and established in a previous study [9, 10]. Thus, both age groups were comparable to a large extend with only minor differences in baseline characteristics, e.g., lower eGFR and higher ALT at baseline in patients ≥ 70 years old. Another relevant prognostic factor under PSMA-targeted RLT is the PSMA-expression in the metastases which can be quantified by whole-body tumor segmentation on PSMA PET/CT [8, 22]. In this regard, Seifert et al. demonstrated that high PSMA expression on [68Ga]Ga-PSMA PET/CT before treatment initiation is linked to a prolonged overall survival in RLT patients [22]. We were unable to include PET-based biomarkers in our analysis, as imaging modalities, e.g., different [68Ga]Ga and [18F]F labeled tracers, for baseline staging were inconsistent in our cohort. Nonetheless, future studies should investigate whether PET-based PSMA-expression is comparable between both groups and may also evaluate whether improved patient selection for RLT is independently linked to baseline PET regardless of age.
Regarding safety, [177Lu]Lu-PSMA RLT was well tolerated across both age groups. Of note safety profile in patients ≤ 65 years old was even favorable when compared to patients ≥ 70 years old with smaller declines in Hb and platelets, translating in fewer cases of anemia or further underscore the favorable safety profile in younger individuals [2, 3]. For instance, Schweigert et al. reported on grade 3 anemia in 6% (versus 4% in younger patients in our cohort) and grade ≥ 3 thrombocytopenia in 3% (versus none in younger patients in our cohort). Of note, relative to our study, Schweigert and coworkers dichotomized their patient cohort using a cut-off of 80 years, while we conducted a dedicated matched-pair comparison focusing on by far younger patients (≤ 65 years), thereby ensuring a broader application of our results in clinical practice. Moreover, in our cohort, all patients with grade 3 toxicities already demonstrated with pre-existing functional impairments at treatment initiation. This is in line with previous studies, focusing on the prediction of adverse events under [177Lu]Lu-PSMA RLT, also reporting on an increased rate of adverse events in patients with impaired kidney or bone marrow function [23, 24]. Another potential side effect of therapies including radiation in general are second malignancies [25]. With earlier application of RLT, the risk of second malignancies especially in younger patients with potentially longer remaining life expectancies might gain relevance [7]. Of note, there had been no reports of any second malignancies in younger patients in our study, albeit the small number of patients and limited follow-up period might have limited interpretability for this question.
In a younger patient cohort concerns about health-related quality of life gain even greater importance, as individual expectations for daily functioning may be even higher in this patients group [26]. As part of the VISION trial, Fizazi et al. assessed relevant quality of life aspects applying well-established questionnaires such as The Functional Assessment of Cancer Therapy (FACT) scale and the EuroQol 5-dimension 5-level (EQ-5D-5 L) under [177Lu]Lu-PSMA RLT compared to the standard of care (SoC) [26, 27]. These instruments enable quantification of functional aspect of everyday life which might be of more relevance in a younger population, including mobility, social functioning and daily activities [26]. This study demonstrated superior quality of life under RLT compared to SoC undermining its well tolerability [26]. These results, together with our findings of strong efficacy and good tolerability in patients ≤ 65 years, further support RLT as a meaningful option for younger subjects.
Some limitations have to be mentioned. Due to the single-center, retrospective trial design, our results need further external validation. We observed a trend toward longer overall survival in younger patients; however, statistical significance was not reached, likely due to the small sample size. Future studies should therefore include a larger patient cohort. Moreover, data about radiographic response was not available in our cohort due to varying follow-up imaging modalities. In addition, patients in our analysis received either [177Lu]Lu-PSMA-I&T or [177Lu]Lu-PSMA-617. However, comparable results in both dosimetry and outcome analysis between both tracers support the feasibility of a pooled analysis [11, 28]. Notably, a subanalysis stratifying patient into the [177Lu]Lu-PSMA-I&T and [177Lu]Lu-PSMA-617 cohorts (with five patients in each age group receiving both radiopharmaceuticals) demonstrated results comparable to those of the pooled analysis (Supplemental Tables 1 & 2, Supplemental Fig. 1 & 2). Nonetheless, future prospective trials should ideally use a single standardized agent to enhance comparability.

Comments (0)