PCa remains one of the most prevalent malignancies among men globally. While localized PCa remains treatable through surgery or radiotherapy, progression to CRPC markedly diminishes therapeutic efficacy and adversely impacts patient survival outcomes and quality of life. AR, a pivotal driver of CRPC pathogenesis, has emerged as a critical therapeutic target. This study conducted a bibliometric analysis of global CRPC-AR research from 2005 to 2024, systematically evaluating 3,149 publications. Our findings synthesize the current research landscape, evolutionary trends, and knowledge hotspots, providing a data-driven framework to guide future investigations into AR-targeted therapies for CRPC treatment.
4.1 Research status and trends
From the global trend in the volume of postings, the marked increase in CRPC-AR publications post-2015 (Fig. 2), peaking in 2021 (321 articles) with parallel citation surges, mirrors escalating clinical demands. CRPC, representing the terminal phase of PCa, poses formidable therapeutic challenges due to drug resistance and poor prognoses, driving intensive exploration of novel targets. The field entered an accelerated developmental phase following the 2012 Phase III trial validating enzalutamide’s survival benefits in mCRPC [13]. Subsequent therapeutic innovations of novel AR antagonists, RLT, and Poly (ADP-ribose) polymerase (PARP) inhibitors synergistically fueled academic productivity [14,15,16], as evidenced by co-citation bursts (Fig. 7D) and keyword bursts (Fig. 8B).
In terms of country distribution, the United States occupies a dominant position in CRPC-AR research, with the number of articles (n = 1,605) far exceeding that of other countries (Table 1). While China demonstrated substantial productivity (n = 592), its relatively limited academic impact (average article citations: 24.46) underscores the need for enhanced methodological innovation and high-impact clinical studies to bolster global scholarly influence. In addition, Canada, Japan, and the United Kingdom also made significant contributions. Collaboration network analysis (Fig. 3B) showed that the United States (TLS = 1,402) has the closest collaboration with other countries, which indicates its pivotal role in global CRPC-AR research. It is evident that countries other than China and the United States (e.g., Central America (including Mexico and the Caribbean), Africa, and Southeast Asia) have published comparatively fewer papers, indicating a lack of representative research achievements. This disparity may stem from several factors: significant gaps in national capabilities, insufficient research investment, uneven distribution of higher education resources, limited cultivation of scientific talent, technological barriers in research, weaker innovation capacity, inadequate international collaboration and exchange, and reduced output due to linguistic differences. Addressing this issue necessitates strengthening global cooperation and resolving geographical disparities in research funding, collaboration, and innovation. Key measures include: First, enhance academic exchange and dissemination through increased global sharing of knowledge, such as regularly organizing international conferences to present the latest research findings; second, foster partnerships in higher education by simplifying scholar visits and student exchanges and developing joint educational programs to cultivate scientific talent across nations; third, launch jointly funded international projects to encourage leading scientists from different countries to collaborate on solving key technological challenges in a mutually beneficial manner; fourth, countries with close ties should take a leading role in international cooperation, jointly advancing exchanges and collaboration in CRPC-AR research to drive sustained progress; fifth, utilize emerging technologies like artificial intelligence and big data to enable real-time data sharing and result validation online, thereby preventing redundant research and resource waste. Enhanced academic exchange among nations will significantly advance research outcomes, elevate research quality, foster consensus, and accelerate scientific progress.
The predominance of U.S. institutions in the top 10 rankings (8 out of 10, Table 2) reflects advantages in research infrastructure and funding allocation. The University of Washington, leading with 168 publications, exemplifies this through its synergistic partnerships with Dana-Farber Cancer Institute and Harvard Medical School (Fig. 4), which have catalyzed the integration of multicenter clinical trials with fundamental mechanistic investigations. U.S. institutions demonstrate unparalleled domestic and international collaborative engagement, a critical factor underpinning their scientific preeminence. This model highlights the transformative potential of institutional collaboration in bridging translational gaps. National institutions should follow the example of the United States to seek a higher level of cooperation and exchange, to learn from the experience of excellent institutions, and to jointly promote the further development of CRPC-AR research.
In terms of authors, Antonarakis, Emmanuel S. emerges as the most prolific author (61 publications), with seminal contributions elucidating the therapeutic implications of AR splice variants, particularly AR-V7, in CRPC progression [17,18,19,20]. Scher, Howard I., the most cited author (2,651 citations), establishes clinical evidence through pivotal CRPC trials and provides a solid foundation for the clinical significance of AR in CRPC therapy [21,22,23,24]. Lotka’s Law analysis reveals a concentrated productivity pattern, with < 10% of authors contributing ≥ 3 publications (Fig. 5A), underscoring the necessity to cultivate larger, sustainable research collectives. The co-authorship network (Fig. 5B) demonstrates geographically constrained collaboration patterns, predominantly limited to intra-national and institutional partnerships. To accelerate innovation, researchers should prioritize cross-institutional and international partnerships, leveraging complementary expertise to address CRPC’s multifaceted fundamental and clinical challenges.
JCR and IF reflect journals’ scholarly influence. Among the top 10 journals by publication volume, 60% has JCR partition of Q1, while 40% exhibites IFs exceeding 5. The top 10 journals have at least 50 publications, and PROSTATE lead in productivity with over 150 publications. Notably, highly cited journals demonstrate superior JCR and IF metrics compare to high-output journals, even including globally recognized titles such as NEW ENGLAND JOURNAL OF MEDICINE, JOURNAL OF CLINICAL ONCOLOGY, and CELL. This suggests that researchers should improve the quality of their research and aim to publish their findings in high-level journals.
4.2 Intellectual structure evolution and research focus migration
The dynamic knowledge framework of CRPC-AR research exhibits distinct evolutionary phases, reflecting both scientific cognition shifts and alignment with evolving clinical demands. Through timeline co-citation clusters analysis, keyword bursts, and citation bursts (Figs. 7C-D and 8B), three developmental periods are delineated: an early phase (2005–2013) of conventional therapeutic exploration, an intermediate phase (2014–2018) of molecular mechanism research, and a contemporary phase ( 2019-present) period of integration of innovative therapies.
4.2.1 Early phase: foundation and limitations of conventional therapeutic strategies
During the nascent phase of CRPC research, therapeutic approaches primarily focused on optimizing ADT and evaluating combination chemotherapy regimens. Keyword burst analysis reveals predominant interest in “antiandrogen withdrawal,” “ketoconazole,” and “steroidal inhibitors” during this period (Fig. 8B), reflecting reliance on conventional hormonal manipulation. Ketoconazole, a CYP17 subfamily A, polypeptide 1 (CYP17A1) inhibitor, emerged as a second-line CRPC therapy by blocking adrenal androgen synthesis; however, its clinical utility was constrained by incomplete adrenal suppression, hepatotoxicity, and adrenal insufficiency [25, 26]. Paradoxically, many patients were able to benefit from abiraterone after ketoconazole application. The docetaxel-prednisone regimen became the frontline chemotherapy standard, showing superior survival benefits, pain control, and quality-of-life metrics compared to mitoxantrone-prednisone, although it was associated with a greater number of adverse events [27]. These studies laid groundwork while exposing therapeutic ceilings inherent to non-selective cytotoxic and adrenal-targeted approaches, motivating subsequent mechanistic investigations.
Initial preclinical studies demonstrated enzalutamide’s stronger AR-binding affinity and anti-androgen efficacy, inducing tumor regression in CRPC xenograft models while reducing serum PSA levels in 43% (13/30) of treated patients [28]. A pivotal advancement during this phase was Scher’s Phase III trial in 2012, which validated enzalutamide’s survival benefit in chemotherapy-pretreated mCRPC patients (median OS improvement: 4.8 months) [13]. This landmark study not only cemented second-generation AR antagonists as standard care but also definitively implicated aberrant AR signaling as the central driver of CRPC progression. These findings catalyzed subsequent investigations into AR pathway activation mechanisms, including aberrant receptor activation through genomic amplification, mutations, and post-translational modifications, laying the molecular foundation for precision therapeutic development.
4.2.2 Intermediate phase: molecular mechanistic Elucidation and exploration of resistance mechanisms
Advancements in molecular biology shifted research focus toward dissecting AR signaling pathway regulation, with “AR-V7” and “DNA repair” emerging as dominant themes. Antonarakis identified AR-V7 in circulating tumor cells (CTCs) of mCRPC patients – a splice variant lacking the ligand-binding domain that constitutively activates AR signaling under castrate conditions, suggesting it is probably a key mediator of enzalutamide and abiraterone resistance [29]. Notably, paclitaxel analogs were more effective than enzalutamide or abiraterone in AR-V7-positive mCRPC patients [30]. This discovery spurred the clinical implementation of AR-V7 detection assays (e.g., circulating tumor cell assay-based platforms) to predict therapeutic response heterogeneity [31].
Genomic profiling of CRPC has progressively matured during this phase. Dan Robinson identified genomic alterations in PIK3CA/B, RSPO, RAF, APC, β-catenin, and ZBTB16 among mCRPC patients [32]. The association between DNA repair deficiencies (e.g., BRCA1/2 and ATM loss/mutations) and CRPC progression has been increasingly elucidated. A Phase II trial demonstrated objective responses to the PARP inhibitor olaparib in 14 of 16 CRPC patients harboring DNA repair defects, highlighting its therapeutic potential [33]. Watson systematically classified AR inhibitor resistance mechanisms into three categories: reconstituted AR signaling (e.g., splice variants), AR-bypass signaling pathways (e.g., glucocorticoid receptor activation), and complete AR Independence mechanisms (e.g., neuroendocrine differentiation) [34]. These advances signify a shift from monotherapeutic AR targeting to multimodal pathway intervention while initiating mechanistic exploration of therapeutic resistance.
4.2.3 Contemporary phase: integration of innovative therapies and precision medicine implementation
Recent years have witnessed CRPC research entering the era of precision medicine. Keyword burst analysis identifies “lineage plasticity,” “membrane antigen,” and “radioligand therapy” as the most dynamic themes. Lineage plasticity—the phenotypic shift from AR-dependent adenocarcinoma to AR-indifferent neuroendocrine carcinoma following ADT—has been recognized as a critical resistance mechanism [35, 36]. This phenomenon provides critical insights into the epigenetic reprogramming underlying advanced PCa progression, enabling the development of phenotype-specific therapeutic strategies [37]. Notably, Ming Han demonstrated that FOXA2 knockout suppresses KIT signaling, thereby inhibiting neuroendocrine prostate cancer (NEPC) growth in human and murine models [38]. Zinc finger protein 397 (ZNF397), an AR coactivator, regulates lineage plasticity via the ten-eleven translocation 2 (TET2) axis. ZNF397 deficiency promotes a TET2-driven plasticity state, while TET2 inhibition reverses AR-targeted therapy resistance in ZNF397-deficient models [39]. These discoveries highlight actionable targets for intercepting lineage plasticity-mediated therapeutic escape.
Prostate-specific membrane antigen (PSMA), a transmembrane protein highly expressed in prostate epithelial cells, has emerged as a promising therapeutic target. While AR does not directly regulate PSMA, it indirectly modulates PSMA expression via binding to the FOLH1 gene enhancer [40, 41]. Clinical studies reveal that AR suppression upregulates PSMA expression, often correlating with metastatic castration-resistant progression and AR pathway reactivation, though specific mechanisms remain incompletely defined [42]. Martin K. Bakht identified HOXB13 as a critical upstream regulator of PSMA in both AR-positive and AR-negative PCa [43]. These insights have galvanized PSMA-targeted therapeutics. PSMA-targeted RLT exploits β-particle radiation to specifically eradicate PSMA-overexpressing tumor cells. A Phase III trial confirmed that Lutetium-177 (177Lu)-PSMA-617 significantly prolongs progression-free survival (PFS) and OS in mCRPC patients [14]. Concurrently, the clinical adoption of PSMA PET/CT imaging has enhanced patient stratification and treatment response monitoring [44, 45]. However, 177Lu-PSMA-617 demonstrates limited efficacy in PCa patients with hepatic metastases [46], likely due to low PSMA expression in liver lesions [43]. PSMA regulation and heterogeneity are influenced not only by AR signaling but also by tumor microenvironment dynamics, epigenetic modifications, and other pathways [43, 47]. Therefore, a comprehensive investigation into the molecular drivers of surface antigen modulation and intratumoral heterogeneity may refine precision strategies for PSMA-directed therapies and novel membrane antigen-based interventions [48].
Six-Transmembrane Epithelial Antigen of the Prostate 1 (STEAP1), a cell membrane-localized metalloproteinase transporter initially identified in PCa tissues, exhibits elevated expression in mCRPC [49, 50]. Prior studies suggest potential AR-mediated regulation of STEAP1 expression [51, 52]. These findings have propelled STEAP1-targeted therapies to the forefront of CRPC research. Vipul Bhatia demonstrated that combining a collagen-binding domain (CBD)-interleukin-12 (IL-12) fusion protein with STEAP1-directed chimeric antigen receptor (CAR) T-cell therapy reprograms the immunologically cold tumor microenvironment of PCa while enhancing host antitumor immunity [53]. Xaluritamig, a STEAP1-targeted XmAb 2 + 1 T-cell engager molecule, exhibits potent T-cell-mediated cytotoxicity against PCa cell lines in vitro and induces tumor regression in xenograft murine models [54]. William K. Kelly conducted the first dose-escalation study of xaluritamig monotherapy in mCRPC patients, providing clinical validation of STEAP1’s therapeutic potential [55]. Furthermore, STEAP1-targeted extracellular vesicle-based fluorescent probes have shown superior efficacy in fluorescence-guided surgery, reducing positive surgical margin rates and improving postoperative survival outcomes compared to conventional white light surgery [56]. However, the mechanistic interplay between STEAP1 and AR signaling remains incompletely characterized. Further preclinical and clinical investigations are warranted to fully elucidate STEAP1’s role as a novel therapeutic target in CRPC treatment.
Future investigations should prioritize molecular mechanisms and tumor heterogeneity based on current findings. Systematic exploration of epigenetic regulation (e.g., DNA methylation, chromatin remodeling) in neuroendocrine transdifferentiation may yield small-molecule inhibitors targeting plasticity nodes. Clinically, monitoring lineage plasticity-associated genetic alterations via circulating tumor DNA (ctDNA) or dynamic PSMA/STEAP1 expression profiling could refine therapeutic decision-making. Integrating single-cell sequencing and spatial transcriptomics could unravel spatiotemporal heterogeneity in PSMA/STEAP1 expression within tumor microenvironments, elucidating their crosstalk with AR signaling and immune modulation [57, 58]. In addition, targeting membrane antigens and using combination applications are promising. Such as PSMA RLT combined with PD-1/CTLA-4 inhibitors, or STEAP1 CAR-T combined with immune checkpoint blockade to overcome the immunosuppressive microenvironment. And explore PSMA and STEAP1 bispecific antibodies or dual-targeted radionuclide therapies, which can cover different subpopulations of tumor cells and achieve dead-end killing of PCa. Or develop nanocarriers or exosomes targeting PSMA/STEAP1 to optimize the delivery route and improve efficacy. These approaches hold transformative potential for overcoming resistance mechanisms and achieving durable responses in AR-targeted CRPC therapy.
Therapeutic targeting of the AR in CRPC has undergone transformative evolution over two decades. Following the limited efficacy of first-generation androgen receptor signaling inhibitors (e.g., bicalutamide) due to acquired agonist switching, second-generation agents established new standards: abiraterone acetate (CYP17 inhibition) and enzalutamide (AR antagonism) significantly prolonged survival in mCRPC while revealing other resistance mechanisms, such as AR splice variants (notably AR-V7) [29, 59]. Recent advances include expanded indications for next-generation AR inhibitors (darolutamide/apalutamide) in non-metastatic CRPC and metastatic hormone-sensitive disease [60, 61]. Mechanistic insights into resistance-conferring AR mutations (e.g., H875Y/T878A, F877L/T878A) and AR-V7 structural biology have accelerated novel therapeutic approaches [62]. Concurrently, the small molecule SC912 inhibits AR-V7 activity in CRPC by targeting the N-terminal domain of AR, thereby exerting its antitumor effect [63]. PARP inhibitor (Talazoparib) for homologous recombination repair-deficient populations, showing durable antitumour activity [64]. This evolution underscores a paradigm shift from broad androgen blockade toward molecularly tailored therapies addressing resistance mechanisms, with ongoing trials poised to further refine precision approaches.
Research on the treatment of advanced CRPC focuses on overcoming resistance mechanisms and developing novel targeted strategies. Resistance primarily involves alterations in the AR pathway (such as AR overexpression, AR-V7, and AR bypass pathways) and androgen pathway-independent alternative pathways, driving the development of combination therapies and novel inhibitors [65]. For AR resistance, novel strategies include non-classical AR binding site inhibitors, proteolysis-targeting chimeras, and selective AR degraders [66]. Additionally, miR-34a therapy targeting prostate cancer stem cells can reverse resistance [67], while microtubule-stabilizing cytotoxic agents (docetaxel and cabazitaxel) exert antitumor effects by inhibiting mitosis in AR-deficient PCa cells [68]. Future efforts should focus on optimizing personalized combination strategies by integrating biomarkers.
4.3 Strengths and limitations
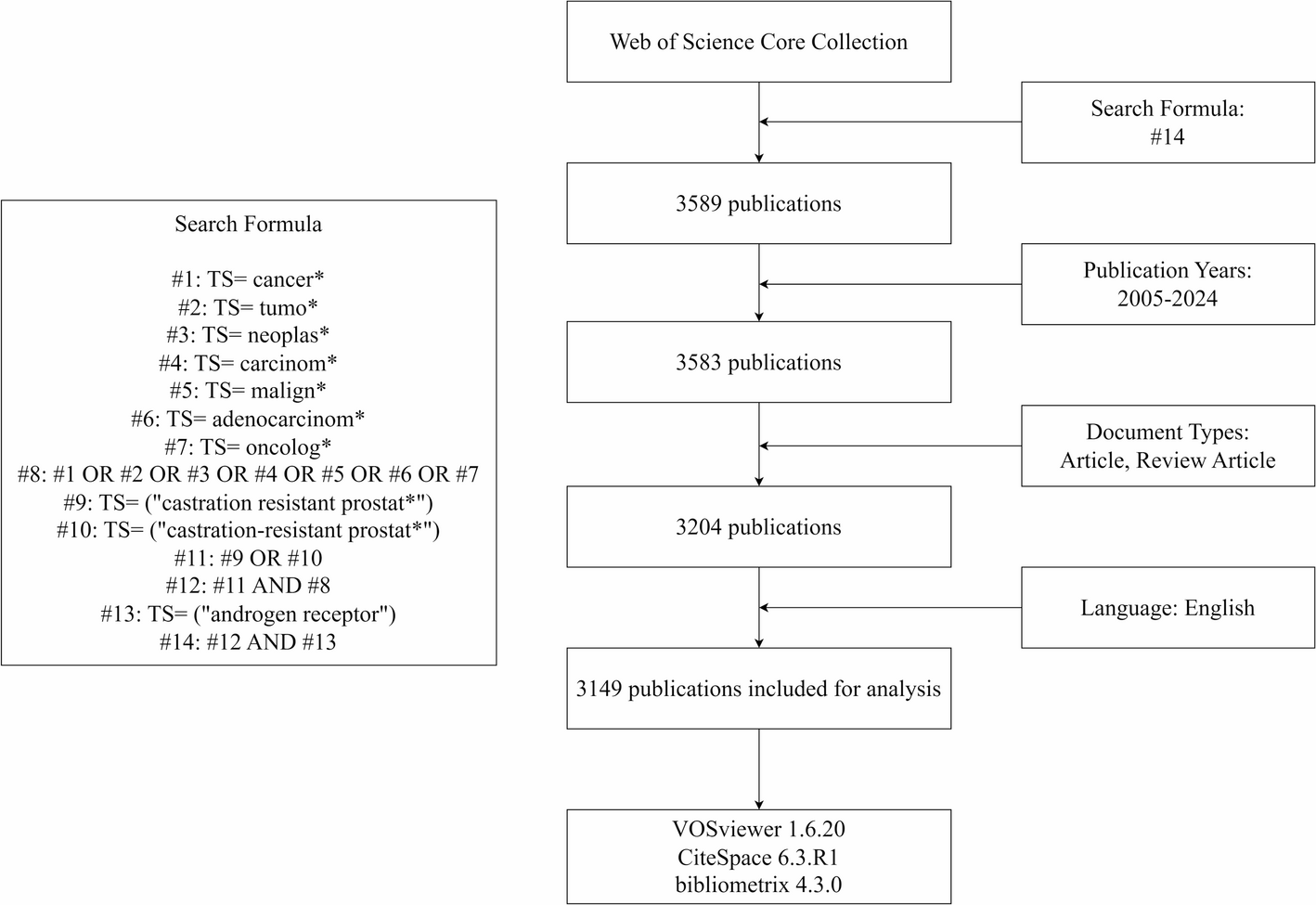
To explore the development trend and research hotspots in CRPC-AR research, this study employs a well-established bibliometric methodology to systematically evaluate research trajectories and emerging frontiers in CRPC-AR investigations. However, it is undeniable that there are some limitations. First, we only retrieved the literature from WoSCC, an authoritative database, which would result in the omission of information from other databases, thus not fully reflecting the research trends in the field. Second, we excluded non-English literature, which may affect the evaluation of related publications. Third, due to the limitations of database updates and the software’s algorithms, the intensity of emerging hotspots’ bursts is relatively small and difficult to find, which may lead to the neglect of research in some emerging fields.

Comments (0)