
Remember me

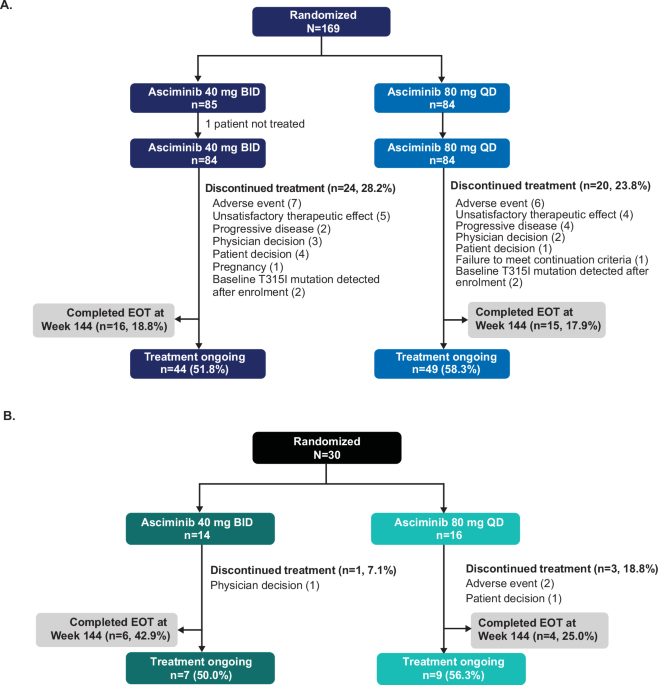


This pooled analysis stratified 216 patients by advanced age from VIALE-A and M14-358 in the venetoclax plus azacitidine cohorts (75–79 years, n = 120; 80–84 years, n = 75; ≥85 years, n = 21) and 87 patients treated with placebo plus azacitidine from the VIALE-A (75–79 years, n = 54; 80–84 years, n = 27; ≥85 years, n = 6) (Fig. 1). Baseline characteristics were largely similar across age groups, including ECOG performance status and cytogenic risk; baseline Grade 3/4 neutropenia was more prevalent in patients ≥85 years of age (Table 1).
Table 1 Patient baseline characteristics by age category.Efficacy outcomesCRc rates were higher with venetoclax plus azacitidine vs. placebo plus azacitidine across all age groups (75–79 years, 67% vs. 19%; 80–84 years, 68% vs. 22%; ≥85 years, 81% vs. 17%; Fig. 2A). The median time to best response of CRc was faster (75–79 years, 1.4 months [range, 0.8–38.7] vs. 3.0 months [0.8–6.3]; 80–84 years, 2.0 [0.9–46.2] vs. 2.3 [1.0–12.2]; ≥85 years, 1.1 [0.7–10.9] vs. 5.3 [5.3–5.3]) and median duration of response was longer (75–79 years, 25.6 months [95% CI, 16.5–35.4] vs. 15.5 months [1.2–not estimable (NE)]; 80–84 years, 30.2 [11.3–NE] vs. 10.4 [1.1–NE]; ≥85 years, 9.6 [5.8–NE] vs. 7.9 [NE–NE]) in the venetoclax plus azacitidine group compared with the placebo plus azacitidine group, respectively, across all age groups; however, the number of responding patients were small in some groups, particularly the placebo plus azacitidine older age groups (80–84 years, n = 6; ≥85 years, n = 1). MRD response rates in CRc responders were higher with venetoclax plus azacitidine compared with placebo plus azacitidine across all age cohorts (75–79 years, 27% vs. 7%; 80–84 years, 21% vs. 4%; ≥85 years, 29% vs. 17%; Fig. 2A).
Fig. 2: Efficacy outcomes.
CRc rates and MRD response rates by age category (A) and AML-CM group (B). AML-CM acute myeloid leukemia composite model, Aza azacitidine, CR complete remission, CRc complete remission + complete remission with incomplete hematologic recovery, CRi complete remission with incomplete hematologic recovery, MRD measurable residual disease, NE not estimable, Pbo placebo, Ven venetoclax.
For patients ≥75 years of age, median OS was 14.1 months (95% CI, 10.7–19.8) in the venetoclax plus azacitidine group and 8.5 months (95% CI, 6.0–10.7) in the placebo plus azacitidine group (Fig. 3), and improvement in median OS with venetoclax plus azacitidine was evident across age groups. In the venetoclax plus azacitidine vs. placebo plus azacitidine arms, respectively, median OS (95% CI) was 14.1 (10.2–24.9) vs. 8.5 (6.8–10.7) months for patients aged 75–79 years, 12.2 (8.0–21.8) vs. 10.1 (2.3–14.5) months for those aged 80–84 years, and 16.2 (9.3–20.5) vs. 2.6 (0.2–NE) patients aged ≥85 years. The proportion of deaths in patients treated with venetoclax plus azacitidine vs. placebo plus azacitidine was 74% (n = 89/120) vs. 96% (n = 52/54) for patients 75–79 years, 77% (n = 58/75) vs. 96% (n = 26/27) for patients 80–84 years, and 81% (n = 17/21) vs. 100% (n = 6/6) for patients ≥85 years (Supplementary Table S1). Rates of transfusion independence were higher in patients treated with venetoclax plus azacitidine vs. placebo plus azacitidine across all age cohorts (Supplementary Table S2).
Fig. 3: Overall survival by age category.
Overall survival for patients aged 75-79 years (A), 80-84 years (B), and ≥85 years (C). Aza azacitidine, NE not estimable, OS overall survival, Pbo placebo, Ven venetoclax.
Safety outcomesThe safety analysis set included 213 patients from M14-358 and VIALE-A receiving venetoclax plus azacitidine and 85 patients from VIALE-A receiving placebo plus azacitidine. The median number of venetoclax plus azacitidine treatment cycles was 7.0 (range, 1.0–46.0) for patients 75–79 years, 7.0 (1.0–45.0) for patients 80–84 years, and 8.0 (1.0–41.0) for patients ≥85 years. The median venetoclax dosing duration per cycle was 21.0 days (range, 1.0–39.0) for patients aged 75–79, 21.0 days (range, 1.0–36.0) for those aged 80–84, and 21.0 days (range, 10.0–34.0) for those aged ≥85. The most common grade ≥3 treatment-emergent AEs (TEAEs) by age group are noted in Table 2. In general, hematologic AEs occurred more frequently in the venetoclax plus azacitidine group compared with the placebo plus azacitidine group across all age cohorts.
Table 2 Most common grade ≥3 TEAEs (>20%) by age category.The proportion of patients who discontinued treatment due to TEAEs was similar between the venetoclax plus azacitidine group and the placebo plus azacitidine group across all age cohorts (Supplementary Table S3). Deaths due to TEAEs were similar between the venetoclax plus azacitidine group and the placebo plus azacitidine group across all age cohorts. Pneumonia was the most commonly reported fatal AE in the venetoclax plus azacitidine arm (9 [4%] vs. 2 [2%] in the placebo plus azacitidine group; Supplementary Table S4).
No differences in baseline mean or change from baseline were observed between the venetoclax plus azacitidine group and the placebo plus azacitidine group across age cohorts with regard to the PROMIS 7A Fatigue score (Supplementary Table S5) or EORTC QLQ-C30 global health status score (Supplementary Table S6).
Outcomes to venetoclax plus azacitidine in patients categorized by AML-CM scorePatient disposition and baseline characteristicsPatients from the phase 3 VIALE-A study were stratified based on AML-CM score as an alternative method to understand outcomes in potentially frail patients (full criteria, Supplementary Fig. S1). A total of 253 patients were in the venetoclax plus azacitidine group (Group A, n = 22; Group B, n = 172; Group C, n = 59) and 127 patients in the placebo plus azacitidine group (Group A, n = 10; Group B, n = 92; Group C, n = 25). Consistent with enrollment of patients ineligible for IC in VIALE-A, 91% of patients receiving venetoclax plus azacitidine and 92% of patients receiving placebo plus azacitidine were in Groups B or C, associated with poorer prognostic disease characteristics, adverse ELN risk, and other comorbidities. A total of 51 patients could not be categorized due to missing data.
Baseline characteristics were largely similar across AML-CM groups, including age and ECOG performance status. There were more patients with ELN intermediate and adverse risk and poor cytogenetics in Groups B and C (Table 3). All patients with pre-existing cardiac dysfunction, including ejection factor (EF) < 50% and stable angina at baseline had an AML-CM score of ≥5 and were in Groups B or C.
Table 3 Patient baseline characteristics by fitness per AML-CM score.Efficacy outcomesIn the analysis based on AML-CM scores, CRc rates were higher with venetoclax plus azacitidine vs. placebo plus azacitidine across all groups (Group A, 77% vs. 50%; Group B, 67% vs. 26%; Group C, 58% vs. 28%; Fig. 2B). The median time to first response of CRc was faster with venetoclax plus azacitidine vs. placebo plus azacitidine across Groups A (1.2 months [range, 0.8–5.1] vs. 4.2 months [0.8–26.8]), B (1.3 [0.8–9.5] vs. 3.0 [1.0–13.2]), and C (1.1 [0.8–19.7] vs. 2.6 [1.1–11.2]). Median duration of response was longer with venetoclax plus azacitidine compared with placebo plus azacitidine across all groups (Group A, 25.1 months [95% CI, 11.1–NE] vs. 9.4 months [1.0–NE]; Group B, 17.1 [9.7–23.6] vs. 13.5 [5.0–15.5]; Group C, 17.8 [7.4–25.8] vs. 8.5 [3.5–NE]; Fig. 2B).
Median OS was longer with venetoclax plus azacitidine vs. placebo plus azacitidine across all groups (Group A, 38.8 months [95% CI, 17.6–NE] vs. 17.7 [9.1–28.8]; Group B, 14.2 [10.7–19.3] vs. 8.6 [6.1–11.4]; Group C, 10.2 [3.4–17.2] vs. 6.6 [2.6–12.8]; Fig. 4). The proportion of deaths in patients treated with venetoclax plus azacitidine vs. placebo plus azacitidine was 54% (n = 12/22) vs. 90% (n = 9/10) for Group A, 77% (n = 133/172) vs. 97% (n = 89/92) for Group B, and 90% (n = 53/59) vs. 100% (n = 25/25) for Group C.
Fig. 4: Overall survival by fitness based on AML-CM score.
Overall survival for patients likely to benefit from IC (A), less likely to benefit from IC (B), and likely to benefit from palliative care or a clinical trial (C). AML-CM acute myeloid leukemia composite model, IC intensive chemotherapy, Aza azacitidine, NR not reached, OS overall survival, Pbo placebo, Ven venetoclax.
Safety outcomesThe safety analysis set included 249 patients receiving venetoclax plus azacitidine and 126 patients receiving placebo plus azacitidine. The median number of venetoclax plus azacitidine treatment cycles was 13.0 (range, 2.0–44.0) for Group A, 7.0 (1.0–45.0) for Group B, and 5.5 (1.0–46.0) for Group C. In the venetoclax plus azacitidine group, the median venetoclax dosing duration per cycle was 23.9 days (range, 16.4–29.0) for Group A, 23.7 days (range, 2.0–30.0) for Group B, and 23.0 days (range, 1.0–29.0) for Group C. In the placebo plus azacitidine group, the median number of treatment cycles was 10.0 (range 1.0–45.0) for Group A, 4.0 (1.0–34.0) for Group B, and 3.0 (1.0–28.0), for Group C, and the median dosing duration per cycle was 27.6 days (range 22.9–28.7) in Group A, 26.8 (2.0–32.2) in Group B, and 24.4 (2.0–29.5) in Group C. The most common grade ≥3 TEAEs by AML-CM score are noted in Table 4. In general, hematologic and gastrointestinal AEs occurred more frequently in patients treated with venetoclax plus azacitidine compared with placebo plus azacitidine across all AML-CM groups.
Table 4 Most common grade ≥3 TEAEs (>20%) by fitness per AML-CM score.In the safety set (venetoclax plus azacitidine, n = 249 and placebo plus azacitidine, n = 126) there were 22 deaths within 30 days of the first dose of study drug (Supplementary Table S7). One patient died from disease progression and 21 died due to AEs. All deaths from AEs occurred in patients from Groups B and C which are noted to have higher rates of baseline comorbidities and higher risk of mortality. Of the deaths due to AEs, 16 (6%) occurred in the venetoclax plus azacitidine arm (AML-CM Group B, n = 8; AML-CM Group C, n = 8) and 5 (4%) in the placebo plus azacitidine arm (AML-CM Group B, n = 2; AML-CM Group C, n = 3).
Comments (0)