
Remember me



The training cohort included 212 patients (median age 51.8 years; range 18.2–86.7). 162 patients (76.4%) had AA, while 50 (23.6%) had IBMFS (Table 1). 51.9% of patients (110 of 212) had no historical normal complete blood count documented prior to presentation. TL testing by flow FISH was available for 116 patients (54.7%), chromosome breakage testing for 90 (42.5%) patients, and genetic testing for IBMFS-associated genes for 65 (30.7%) patients (Supplemental Table S3). 151 AA patients (93.2%) were treated with IST, and 85.7% (120 of 140 evaluable patients) achieved a partial or complete hematologic response at 6 months. Based on our diagnostic adjudication criteria for this study, 80.2% of AA patients (130 of 162) were further classified as having confirmed diagnosis of AA by virtue of hematologic response to IST or negative IBMFS genetic testing, while 32 were categorized as having a presumed diagnosis of AA based on expert evaluation and exclusion of other conditions (Supplemental Table S4).
Table 1 Clinical Characteristics of the Training Cohort.Of the IBMFS cases, 48 of 50 (96.0%) had a confirmed diagnosis (25 (50.0%) had telomere biology disorders (TBD), 8 (16.0%) had Fanconi anemia (FA), 5 (10.0%) had Diamond-Blackfan anemia (DBA), 3 (6.0%) had GATA2 deficiency, and 7 (14%) had other defined congenital syndromes), while 2 (4.0%) carried a clinical diagnosis of IBMFS without a genetic cause identified (Supplemental Tables S5). Of the IBMFS patients, 39 (78.0%) presented with hematologic manifestations, while 11 (22.0%) were diagnosed during evaluation or treatment of extra-hematopoietic features (e.g., pulmonary fibrosis in TBD, failure to recover blood counts after chemotherapy for solid tumor in FA). Three patients with IBMFS initially received IST for treatment of presumed AA without hematologic response before an eventual diagnosis of IBMFS—one based on a newly reported TUBB variant identified on re-analysis of prior whole-exome sequencing [36], one due to new clinical manifestations of TBD in the absence of an identified germline mutation, and the third was found to have genetically-confirmed GATA2 deficiency after GATA2 deficiency syndrome was described in the literature.
Clinical and laboratory features diverged sharply between AA and IBMFS groups (Tables 1–2, Fig. 1). The most striking differences between groups were in the acuity and severity of cytopenias (Fig. 1A–C): 118/162 (72.8%) of AA patients had acute-onset ( < 1 year) severe or very severe AA (SAA/VSAA), compared to only 1/50 (2.0%) IBMFS cases (p < 0.001). Conversely, chronic ( > 1 year) non-severe cytopenias (NSAA) predominated in IBMFS (39/50 [78.0%]) compared to AA (8/162 [4.9%]; p < 0.001).
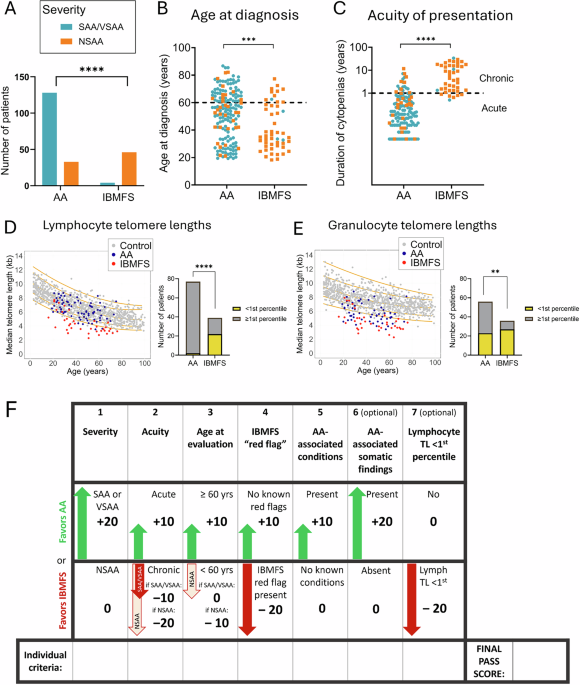
Fig. 1: Defining clinical characteristics of AA and IBMFS. The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.A Disease severity at presentation. Bar plot showing numbers of patients with severe or very severe aplastic anemia (SAA/VSAA, teal) and non-severe aplastic anemia (NSAA, orange) among those with AA and IBMFS. B Shown is the distribution of ages (in years) at the time of bone marrow failure diagnosis, with orange dots showing patients presenting with NSAA and teal for those presenting with SAA/VSAA. The dashed line marks the 60-year age, which was used for subsequent regression analyses. C Acuity of presentation, defined by the duration of cytopenias from the first abnormal CBC to diagnosis. Patients with AA typically presented acutely, defined as within 1 year of cytopenia onset, whereas those with IBMFS more often had a chronic course extending beyond 1 year. Disease severity is also indicated by orange (NSAA) and teal (SAA/VSAA) dots. The dashed line marks the 1-year threshold used to define acute versus chronic presentation. D,E Median telomere lengths in lymphocytes (D) and granulocytes (E) measured by flow-FISH analysis for 77 AA (blue dots) and 39 IMBFS patients (red dots) with available raw telomere lengths data. Telomere length distributions from healthy controls are shown for reference (gray dots), based on published data from Johns Hopkins (n = 192) and Vancouver (n = 444), with percentile curves in orange (1st, 10th, 50th, 90th, and 99th percentiles, from bottom to top). To the right of each telomere length scatter plot are the corresponding summary analysis depicted in stacked bar plots showing the number of AA and IBMFS patients with telomeres <1st percentile in lymphocytes (D), and granulocytes (E). Statistical significance was determined using Fisher’s exact test for categorical variables (A,D,E) and two-sided Student’s t tests for continuous variables (B,C). p values are indicated as follows: **, p < 0.01; ***, p < 0.001; **** p < 0.0001 (****). F Schematic demonstrating the PASS score calculation. The PASS score is calculated by adding individual criteria contributions from seven clinical factors: (1) Cytopenia severity, with +20 points assigned for SAA/VSAA (defined as two or more of the following: absolute neutrophil count (ANC) < 0.5·103 cells/μL, anemia with an absolute reticulocyte count <60·103 cells/μL, platelets < 20·103 cells/μL), and 0 points assigned for NSAA (defined as having one or fewer severe cytopenias defined above). (2) Acute presentation, defined as cytopenias of 1 year or less in duration (or having no documented previous abnormal blood count with cytopenias presumed to be acute) are assigned +10 points. Chronic presentation, defined as cytopenias >1 year duration, are assigned either −10 points in patients with SAA/VSAA cytopenias, or -20 points in patients with NSAA cytopenias. (3) Patients being evaluated at 60 years and older are given +10 points, while those under 60 years at the time of evaluation are assigned 0 points in patients with SAA/VSAA cytopenias or −10 points in patients with NSAA cytopenias. (4) IBMFS red flag is assigned –20 points if any of the red flag conditions are present; patients are assigned +10 points if there are no red flags. IBMFS red flag is defined as having any of the following i) congenital abnormality, including abnormal thumb, or dysmorphic features, ii) Interstitial lung disease, avascular necrosis, or unexplained liver cirrhosis, iii) Mucocutaneous triad of nail dystrophy, skin hyperpigmentation, oral leukoplakia, iv) Unexpected hematologic toxicity with failure to recover blood counts after chemotherapy or radiation, v) Refractory warts or a history of non-TB mycobacterial infection, vi) Squamous cell cancer of the head and neck or anogenital region, vii) First-degree relative with a diagnosis of bone marrow failure or thrombocytopenia, MDS, AML, or one of the red flag conditions. (5) Presence of rare conditions etiologically related to AA or incompatible with IBMFS (“AA-associated conditions”) is assigned +10 points. Absence of these conditions is given 0 points. AA-associated conditions are defined as: i) Seronegative autoimmune hepatitis, ii) Treatment with immune checkpoint inhibitors, iii) Known diagnosis of immune dysregulation syndrome (e.g., CTLA4 haploinsufficiency), iv) History of eosinophilic fasciitis, v) History of thymoma, vi) History of Hodgkin’s lymphoma, vii) Patient previously tolerated cytotoxic chemotherapy without unexpected hematologic toxicity (e.g., historical treatment for breast cancer or lymphoma) non-contiguous to current episode of BMF. (6) Presence of clonal hematopoiesis with any one of the following AA-associated acquired somatic changes is assigned +20 points: PNH granulocyte clone ≥0.5%, acquired chromosome arm 6p loss of heterozygosity (6pLOH), acquired del(13)(q) as an isolated abnormality, and somatic mutation in BCOR or BCORL1 genes. Absence of these is given 0 points. (7) Median lymphocyte telomere lengths <1st percentile are given −20 points, while longer telomere lengths of 1st percentile and higher are given 0 points. Note: Of the seven individual score criteria, factors 1–5 are required to calculate the PASS score. Factors 6 and 7 are not required, but recommended when available and can be added later as they become available for greater diagnostic accuracy. Missing values are assigned 0.
Table 2 Logistic Regression and LASSO Analysis Identifying Seven Clinical Variables for Inclusion in the PASS Model.AA patients were older at presentation (median 54.7 years; range 19.3–86.7) compared to IBMFS patients (median 37.4 years; range 18.8–72.4; p = 0.001) (Fig. 1B). Both groups had patients presenting at age ≥60 years, but presentation in the older age range was more common for AA (AA: 63/162 [38.9%] vs. IBMFS: 11/50 [22.0%]; p = 0.031).
Clinical stigmata or family history suggestive of IBMFS were present in 45 of 50 IBMFS patients (90.0%) versus 6 of 162 (3.7%) AA patients (p < 0.001, Table 2). A subset of AA patients (10 of 162, 6.2%) had conditions associated with AA (e.g., checkpoint inhibitor use, seronegative hepatitis) [41,42,43,44, 47]; these were absent in IBMFS patients.
Clonal hematopoiesis was identified by clinical testing in 142 patients (67.0% of the cohort). Somatic changes characteristic of AA were present in 52.5% of AA patients (85/162) (Tables 1–2) and included granulocyte PNH clones ≥0.5% in 43.0% (65/151) of evaluable patients, acquired 6pLOH in 13.7% (10/73) of evaluable patients, somatic mutations in BCOR or BCORL1 in 17.1% (18/105), and del(13)(q) as an isolated abnormality in 5.8% (9/154). These AA-associated somatic findings were rare in IBMFS (1 of 50 [2.0%]; p < 0.001).
Among patients with TL measurements, fewer AA patients had lymphocyte TLs <1st percentile for age (2/77 [2.6%]) compared to IBMFS (22/39 [56.4%], p < 0.001), of whom 17 had TBD and five had other IBMFS (Fig. 1D, Table 2). The two AA patients with TLs <1st percentile lacked TBD-associated germline variants or clinical features beyond BMF; one responded to IST, while the other had refractory AA and underwent BMT. Lymphocyte TLs above 10th percentile were found in 71.4% (55/77) of AA vs 17.9% of IBMFS patients (p < 0.001); of the seven IBMFS patients with lymphocyte TLs>10th percentile, two had FA, 1—DBA, 1—GATA2 deficiency and three had various other IBMFS. Granulocyte TLs were less discriminatory between AA and IBMFS, with 41.1% of evaluable AA patients (23 of 56) having granulocyte TLs <1st percentile compared to 75.0% (27 of 36) for IBMFS (p = 0.002) (Fig. 1E). Only 32.1% (18 of 56) AA patients had granulocyte TLs over 10th percentile.
Development and performance of the PASS model in the training cohortWe next performed the LASSO logistic regression on the seven candidate variables identified in our univariate analysis (Table 2). LASSO is a logistic regression technique that optimizes variable selection by adding a penalty for inclusion of too many variables that could lead to overfitting. LASSO retained all seven variables with the optimal penalty (λ 0.007). We assigned points ( ± 10 or ±20) based on LASSO coefficient direction, with positive values for factors associated with AA and negative values for those linked to IBMFS (Fig. 1F).
To evaluate model performance, we next applied the PASS score to our training cohort of 212 patients (Fig. 2A-E, Table 2). The score demonstrated excellent diagnostic discrimination, with an area under the ROC curve AUC of 0.990 (95% confidence interval [CI]: 0.982–0.999) (Fig. 2A). Calibration analysis showed strong agreement between predicted and observed probabilities (Fig. 2C) and the Brier score showed good calibration and high predictive performance at 0.035.
Fig. 2: The PASS model performance in the training cohort. The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.A The ROC curve, showing the sensitivity (true positive rate) on the Y-axis against the false positive rate (1 − specificity) on the X-axis for scores generated with the PASS model in the training cohort. The red dots correspond to labeled scores in the training cohort. Ideal discrimination allows perfect sensitivity without false positives (upper left quadrant). The dashed diagonal line indicates no discrimination between true and false positives (random). The PASS score shows an excellent area under the curve (AUC), indicating near-perfect diagnostic performance. Blue arrow points to the score of 30, and red arrow to the score of 0, which were chosen as score thresholds for PASS. B A plot demonstrating the PASS score performance characteristics (plotted on the Y-axis) across a range of score thresholds (on the X-axis). Plotted are the PPV (light blue), specificity (dark blue), NPV (light green), and sensitivity (dark green). The dashed vertical lines are shown at a score of 30 (demarcating scores with 100% PPV and specificity for AA), and at a score of 0 (demarcating a threshold below which the probability of an AA diagnosis starts to sharply fall and IBMFS diagnosis is more likely). C This panel shows a calibration plot comparing predicted probability of AA derived from a logistic regression model (PASS score as predictor) on x-axis with observed frequency of AA on the y-axis. Each point represents a bin of rounded predicted probabilities, annotated with average PASS score and sample size. The dashed diagonal line indicates perfect calibration. The shaded blue region reflects a LOESS-smoothed fit with 95% confidence interval. Green and red annotations highlight regions of systematic underestimation and overestimation, respectively. The model performs well at the extremes, where very low and very high predicted probabilities align with observed outcomes. Arrow points to the region of the plot corresponding to the threshold of 30. D Distribution of AA and IBMFS diagnoses across the range of PASS scores (on X-axis), demonstrating excellent separation between the two diagnostic categories, with high specificity for AA for positive PASS scores of 30 and higher. E Proportion of AA and IBMFS diagnoses across the range of PASS scores, showing that lower scores are strongly enriched for IBMFS while higher scores are enriched for AA, with near-complete separation at thresholds above 20.
The positive predictive value (PPV) and specificity for AA increased with higher PASS scores (Fig. 2B). In the training cohort, scores ≥30 were associated with a 100% PPV for AA and predicted response to IST, with 88.0% (103 of 117) of evaluable patients responding at 6 months, compared to 65.3% (17 of 26) for scores <30 (p = 0.004). PPV for IBMFS increased with lower scores (Fig. 2B, D, E), with 86.8% of patients (46 of 53) with scores <0 having IBMFS. Among patients with intermediate scores (0 to 20), the majority (82.6%, 19 of 23) had AA; of those treated with IST, 72.2% (13 of 18) responded at 6 months.
Incorporating the most sensitive threshold for PNH clone detection including clones <0.5% and recalculating the score as new laboratory findings (e.g., AA-associated somatic changes) emerged later in the disease course resulted in an AUC 0.992 (95% CI 0.985-0.999), slightly improving sensitivity from 0.840 to 0.877 while retaining 100% PPV for AA for scores ≥ 30 (Supplemental Fig. S2). Because this improvement was small, we retained the more conservative PNH clone threshold of ≥0.5% to maximize diagnostic specificity, given prior reports of very small PNH clones in rare IBMFS patients [35].
PASS Score validation in external BMF cohortsWe next assessed the performance of the PASS score in four independent external validation cohorts of adult BMF patients: (1) 270 patients from the French national reference database (RIME) [51], (2) 247 patients from a published dataset from the NIH/USP [10], (3) 121 patients from MDA, and (4) 78 patients from UTSW. The four cohorts had different prevalences of IBMFS patients, reflecting variations in referral practices and patient recruitment: IBMFS comprised 10.7% (29 of 270) in the RIME cohort, 17.8% (44 of 247) in the NIH/USP cohort, 7.7% (six of 78) in the UTSW cohort, and 42.9% (52 of 121) in the MDA cohort. Similar to the training dataset, the most common IBMFS across all validation cohorts were TBDs, comprising a median of 65.5% (range 50–100%) of IBMFS diagnoses (Supplemental Table S6A-D), reflecting TBDs being the most common IBMFS in adults.
Across these cohorts, clinical presentations of AA and IBMFS were consistent with the training dataset (Supplemental Tables S7–S10). Most IBMFS patients presented with NSAA: 69.0% in RIME, 90.9% in NIH/USP, 83.3% in UTSW, and 94.2% in MDA. The majority of AA patients presented with acute-onset cytopenias—97.9% in RIME, 98.0% in NIH/USP, 88.9% in UTSW, and 91.3% in MDA. Most AA patients had severe or very severe cytopenias (SAA/VSAA), observed in 84.2% in RIME, 69.5% of NIH/USP, 61.1% of UTSW, and 84.1% of MDA patients. In contrast, IBMFS patients were more likely to have lymphocyte TL <1st percentile, and few or no IBMFS patients exhibited AA-associated somatic alterations. IBMFS “red flags” were present in 82.8% in RIME, 52.3% of NIH/USP, 83.3% of UTSW, and 80.8% of MDA patients with IBMFS.
Application of the PASS score to the four datasets demonstrated excellent discriminatory performance (Fig. 3 A-L, Table 2), with ROC AUCs of 0.977 (95% CI: 0.968–0.987) in all combined cohorts (Fig. 3M), and ROC AUC of 0.985 (95% CI: 0.974-0.997 RIME), ROC AUC of 0.969 (95% CI: 0.948–0.990 NIH/USP), ROC AUC of 0.979 (95% CI: 0.957–1.0 MDA), and 0.955 (95% CI: 0.898–1.0 UTSW) in the cohorts analyzed separately (Fig. 3A, D, G, J). The combined calibration plot showed strong agreement between predicted and observed probabilities (Fig. 3O) and Brier scores showed strong predictive performance at 0.044.
Fig. 3: The PASS model performance in four external validation cohorts. The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Panels are grouped by cohort: A–C: RIME, D–F: NIH/USP, G–I: MDA, J–L: UTSW, and K-O: combined cohort. A,D,G,J,K ROC curves showing sensitivity (Y-axis) versus false positive rate (X-axis) for PASS scores in each validation cohort. Red dots indicate labeled scores from the training cohort. The dashed diagonal line represents random classification; ideal discrimination lies in the upper left quadrant. Across all cohorts, the PASS model demonstrates excellent diagnostic performance, with high area under the curve (AUC), reflecting strong separation between AA and IBMFS. B,E,H,K Distribution of AA and IBMFS diagnoses across PASS scores. AA diagnoses cluster at higher scores, with only AA diagnoses scoring at 30 and higher, and IBMFS clustering at lower scores. C,F,I,L Diagnostic performance metrics across score thresholds, including PPV (light blue), specificity (dark blue), NPV (light green), and sensitivity (dark green). Vertical dashed lines mark thresholds of 0 and 30, which delineate low and high likelihood of AA, respectively. Scores ≥30 yield 100% PPV and specificity for AA, while scores <0 are associated with a sharp decline in AA probability and increased likelihood of IBMFS. These patterns were consistent across all three validation cohorts. N Proportion of AA and IBMFS diagnoses across the range of PASS in the combined validation cohort. Lower PASS scores were predominantly associated with IBMFS, while higher scores were enriched for AA, with near-complete separation achieved at thresholds above 20. O Calibration plot for the combined validation cohorts, comparing predicted probability of AA (X-axis) with observed frequency (Y-axis). The dashed diagonal line indicates perfect calibration. A LOESS-smoothed fit with 95% confidence interval is shown within the blue shaded region. The model demonstrates good calibration across the full range of predicted probabilities, with close alignment between predicted and observed frequencies, particularly at the high scores where discrimination is strongest.
Threshold-based analysis revealed that scores ≥30 had a positive predictive value (PPV) of 100% for AA across all validation cohorts (Fig. 3C, F, I, L). In contrast, scores below 0 were predominantly associated with IBMFS patients, yielding a PPV of 81.6% for IBMFS across all datasets. Analyzed separately, PPVs for IBMFS with PASS < 0 were 77.4% in RIME, 75.5% in NIH/USP, 94.0% in MDA, and 57.1% in UTSW, delineating a subset of individuals warranting further evaluation for IBMFS. Most, but not all, patients with intermediate scores (0–20) had AA: 85.7% across all cohorts, and individually—84.8% in RIME, 91.5% in NIH/USP, 66.7% in MDA, and 88.2% in UTSW (Fig. 3B, E, H, K, N). These findings may help identify patients who could benefit from IBMFS evaluation or re-evaluation, particularly in patients going to BMT and in cases of IST-refractory disease.
The effect of TL and somatic alteration components on PASS performanceBecause TL measurement by flow-FISH and somatic genetic testing results may be delayed or unavailable in some settings, we examined the effect of availability of these score components on PASS performance.
Among 928 patients, 457 (49.2%) had available TL measurements (Supplemental Table S11). In PASS, TL <1st percentile lowers the score, whereas TL ≥1st percentile or unavailable testing has no effect. Comparing within the subset of patients with available TL data, omission of TL shifted scores upward in patients with very short TL, increasing sensitivity for AA at PASS ≥ 30 but reducing sensitivity for IBMFS at PASS < 0 (Supplemental Figure S3). Despite this shift, discrimination remained strong without TL (ROC AUC 0.955) compared with PASS including TL (ROC AUC 0.974), with preserved calibration. PPV for AA at PASS ≥ 30 remained high without TL (98.8% vs. 100% with TL), while PPV for IBMFS at PASS < 0 was modestly increased (88.2% vs 83.8% with TL). In the full 928-patient cohort, PASS omitting TL had ROC AUC 0.9703, with 99.5% PPV for AA at PASS ≥ 30.
When TL was excluded, three of 181 IBMFS patients (1.7%) (all with TBD) had PASS ≥ 30 and were classified as AA (MDA074, NIH316, and USP022) (Supplemental Table S12). Detailed review demonstrated that in one patient NIH316, a notation of “abnormal cutaneous findings” was not included as IBMFS red flag due to insufficient descriptive detail in the published NIH/USP dataset. Prospective classification of this feature would have revised the no-TL PASS to the intermediate range (PASS = 20). Another patient (USP022) likely had concurrent AA in the setting of a germline TERT variant of uncertain significance. This patient presented with acute-onset NSAA, a 6% PNH clone, absence of IBMFS red flags, TL <1st percentile, and a TERT c.2154 C > A (p.Asp718Glu) variant of uncertain significance. The no-TL PASS was 30, whereas incorporation of TL appropriately reclassified the patient into intermediate category (PASS = 10), reflecting diagnostic uncertainty.
Somatic testing was available in 90.6% of patients (841/928) (Supplemental Table S13). Inclusion of the somatic component increased sensitivity for AA at PASS ≥ 30, while discrimination remained excellent whether the somatic component was included or omitted (ROC AUC 0.981 vs. 0.977, respectively)(Supplemental Figure S4). Omission of the somatic component led to modest redistribution of AA patients into lower and intermediate score ranges. PPV for AA at PASS ≥ 30 remained 100% regardless of somatic inclusion, whereas PPV for IBMFS at PASS < 0 was modestly reduced when somatic data were omitted.
A total of 419 patients (45.1% of 928) had evaluable TL and somatic data (Supplemental Table S14). Omission of both components resulted in a greater decline in discrimination than omission of either alone (ROC AUC 0.943 vs. 0.973 when both were included), though calibration remained good. Importantly, PASS retained high PPV for AA at PASS ≥ 30 (99.1%) even when both components were unavailable (Supplemental Fig. S5).
Together, these results demonstrate that TL and somatic components improve PASS precision and help resolve diagnostically ambiguous phenotypes, while PASS maintains robust discriminatory performance and excellent predictive value for AA when these data are unavailable.
Comparison of PASS to prior diagnostic modelsWe next compared the diagnostic performance of PASS to NIH-ML [10] and RIME recursive partitioning models [51] (Table 3). We limited this analysis to patients with available PNH flow cytometry to ensure that patients could be analyzed using the RIME model. The NIH-ML model could be compared only for the NIH/USP cohort using published predictions from the NIH-ML manuscript [10], because the NIH-ML algorithm is not publicly available.
Table 3 Comparison of PASS to Prior Predictive Models.Comparing the three models in the NIH/USP cohort, both PASS and NIH-ML showed similarly excellent discriminatory performance (PASS 0.970 [95% CI 0.948–0.992], NIH-ML ROC of 0.941 [95% CI 0.889–0.992]. However, PASS had stronger PPV for AA: PASS PPV for AA was 100% (147/147) for PASS ≥ 30, whereas the NIH-HL model failed to issue a prediction for 4 IBMFS patients (9.1% of 44), and misclassified another 4 (9.1%) of IBMFS patients as AA (Supplemental Table S15).
PASS outperformed the RIME model in all except the RIME derivation cohort, where performance was comparable (Table 3). In all five cohorts combined (N = 865), PASS demonstrated ROC 0.980 (95% CI 0.972–0.988), PPV for AA ≥ 30 = 100% 598/598), and Brier 0.037, compared with ROC AUC 0.865 (0.830–0.899), PPV for AA 96.8% (667/689), and Brier 0.075. 22 of 127 (17.3%) of IBMFS patients were misclassified as AA by the RIME model (Supplemental Table S16), compared to 0 for patients with PASS ≥ 30.
Inter-operator reproducibility and the development of the clinical calculator toolTo assess inter-operator reproducibility, three hematology-oncology clinicians independently applied the PASS to 20 randomly selected patients from the training cohort. Inter-observer agreement, measured using Fleiss’ κ (a statistic accounting for agreement expected by chance), was 0.875, indicating near-perfect agreement and good reproducibility across independent raters. Minor variability was observed in exact point totals, reflecting inherent limitations of retrospective clinical data abstraction; however, agreement on categorical diagnostic classification remained uniformly high, demonstrating the real-world robustness and flexibility of PASS scoring, with consistent assignment to AA, IBMFS, or intermediate categories across raters.
To support clinical implementation, we developed an open-access PASS clinical calculator (Fig. 4, available at https://pennmedicine.shinyapps.io/passcalc/). This tool allows users to input clinical variables and returns the calculated score along with its interpretation for three patient subgroups based on score thresholds ( ≥ 30, 0–20, and <0). The score can be recalculated as additional variables emerge during the disease course. To assist with interpretation, the tool also displays the corresponding score distributions for AA and IBMFS patients in the combined training and validation cohorts.
Fig. 4: PASS score calculator. The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Shown are screenshots of the web-based PASS calculator, showing its use for a hypothetical patient case. A Calculator disclaimer. B Required clinical inputs that are typically available at the time of initial evaluation. C Score components for somatic genetic testing and telomere length assessment, which may not be immediately available and are not required for calculator use; however, inclusion of these components is recommended once available to optimize diagnostic performance (see text). D Calculator output displaying the total PASS score and corresponding diagnostic interpretation, along with a summary table of entered variables and assigned point values, and the distribution of PASS scores among 928 patients with bone marrow failure included in this study. The calculator is available at https://pennmedicine.shinyapps.io/passcalc/.
Comments (0)