
Remember me

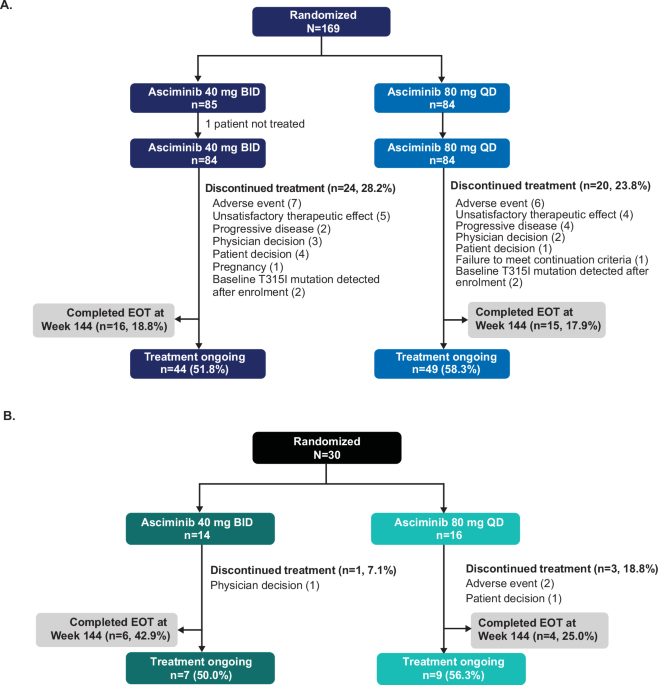


Overall, 169 patients who were not in MMR at baseline were enrolled in the main cohort between November 2021 and March 2023 and randomized to asciminib 40 mg BID (n = 85) or 80 mg QD (n = 84) (Fig. 1A). One patient in the 40 mg BID arm was not treated. At data cutoff (11 February 2025), after a median follow-up of 124.1 weeks (28.6 months), 31 patients (18.3%) had completed the end of treatment (EOT) visit at Week 144, and treatment was ongoing for 93 patients (55.0%); most patients who discontinued asciminib (17/44) did so before Week 24.
Fig. 1: Patient disposition. The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.A Main cohort; B Exploratory cohort. BID, twice daily; EOT end of treatment, QD once daily.
A total of 40 patients in the main cohort (16 in the 40 mg BID arm and 24 in the 80 mg QD arm) had their asciminib dose escalated to 200 mg QD, all except one due to not achieving MMR at Week 48. By data cutoff, 11 of these patients had completed the EOT visit at Week 144, and 24 were receiving treatment with the higher asciminib dose. Among the patients who discontinued treatment (n = 5), progressive disease was the most common reason (n = 2).
Patients were heavily pretreated, and most had discontinued their previous TKI due to resistance (Table 1 and Supplementary Fig. 2). Although the study arms were balanced in terms of age and race, there were differences across treatment arms in other categories (sex, ethnicity, number of previous TKI treatment lines, reason for discontinuation of last TKI, response level at baseline). Patient demographics and disease characteristics for the patients who had their asciminib dose escalated to 200 mg QD are presented in Supplementary Table 1.
Table 1 Patient demographics and disease characteristics (main and exploratory cohorts).The exploratory cohort of 30 patients already in MMR at baseline was randomized to asciminib 40 mg BID (n = 14) or 80 mg QD (n = 16). Patients in this cohort were similar to patients in the main cohort regarding age and sex; however, there was a larger proportion of patients who had received ≥5 previous treatment lines in this group compared with patients not in MMR at baseline (Table 1). Median time from initial diagnosis of CML was 4.5 years (range 1.3─21.2). At data cutoff, 10 of these patients (33.3%) had completed the EOT visit at Week 144 and treatment was ongoing for 16 patients (53.3%) (Fig. 1B). One patient in the 40 mg BID arm (physician decision) and three patients in the 80 mg QD arm discontinued treatment (AEs, n = 2; patient decision, n = 1).
Efficacy: primary endpointThe MMR rate at Week 48 for patients in the main cohort was 39.4% (95% CI: 31.9, 47.3); 43.4% (95% CI: 32.5, 54.7) in the 40 mg BID arm and 35.4% (95% CI: 25.1, 46.7) in the 80 mg QD arm (Table 2). Response rates over time (at Week 48 and Week 96) are detailed in Table 3. MMR rates at and by scheduled time points are presented in Supplementary Tables 2 and 3. Of note, the T315I mutation was detected in four patients after treatment start; although the sample for mutation testing was collected before patients received asciminib, treatment had already started by the time the results were available; these patients were excluded from efficacy analyses.
Table 2 MMR at Week 48 (main cohort).Table 3 Response rates over time (main cohort).The dosing arm populations were not balanced, with the 40 mg BID arm including a larger proportion of female patients and patients aged <65 years, as well as a lower proportion of patients who had discontinued their previous TKI due to resistance or who had received three or more previous TKIs (Supplementary Table 4). Given this imbalance, an ad-hoc statistical analysis using propensity weighting scores was conducted to investigate the numerical differences in MMR rates. Differences were not significant for MMR rates at Week 48 for patients treated with asciminib 40 mg BID or 80 mg QD (ad-hoc nominal p value, p = 0.763; Supplementary Table 5). Since MMR rates in ASC4OPT were numerically higher than those reported in the ASCEMBL study (43.4% vs 29.0% for asciminib 40 mg BID at Week 48) [8], a separate propensity weighting score analysis was conducted to investigate the differences between the MMR rates. As shown in Supplementary Table 5, no significant differences were observed between MMR rates in ASC4OPT and ASCEMBL.
Efficacy: secondary endpointsThe estimated median time to first MMR among those who achieved it was 22.7 weeks (13.1 weeks and 23.9 weeks for patients on asciminib 40 mg BID and 80 mg QD, respectively). MMR rates continued to increase throughout the study, reaching similar levels in both arms at Week 96 (45.8% and 41.5% for 40 mg BID and 80 mg QD, respectively) (Table 3). Figure 2 shows cumulative MMR rates; the median duration of MMR was not estimable for either dosing regimen (Supplementary Fig. 3).
Fig. 2: Cumulative response plot of time to first MMR (main cohort). The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Patients without RT-qPCR assessment at a certain time point are considered as non-responders at that time point. BID, twice daily; MMR, major molecular response; QD, once daily; RT-qPCR, reverse transcription quantitative polymerase chain reaction.
MR4 and MR4.5 rates at Week 48 were 17.0% and 10.3%, respectively (20.5% and 12.0% for patients on 40 mg BID, and 13.4% and 8.5% for patients on 80 mg QD, respectively); at Week 96, the corresponding values were 17.0% and 10.9%, respectively. (Table 3, and Supplementary Tables 6 and 8); data by scheduled time points are presented in Supplementary Tables 7 and 9).
At Week 48 and Week 96, BCR::ABL1IS ≤ 1% was achieved in 63.6% (66.3% on 40 mg BID and 61.0% on 80 mg QD) and 64.8% (62.7% on 40 mg BID and 67.1% on 80 mg QD) of patients, respectively (Table 3 and Supplementary Tables 10 and 11). At Week 48, the CCyR rate was 58.2% for all patients (60.2% and 56.1% for patients on asciminib 40 mg BID and 80 mg QD, respectively).
Among the 40 patients in the main cohort who received asciminib at the escalated dose of 200 mg QD, 17.5% had achieved MMR at Week 96.
In the exploratory cohort of patients already in MMR at baseline, the overall MMR maintenance rate at Week 48 was 93.3% (28/30 patients); 100% in the 40 mg BID arm and 87.5% in the 80 mg QD arm (Table 4). Two patients in the 80 mg QD arm discontinued treatment due to AEs before Week 48 and were counted as non-responders. At Week 96, MMR was maintained by 86.7% of patients (92.9% on 40 mg BID and 81.3% on 80 mg QD). The proportion of patients in MR4 rose from eight at baseline (3/14 on 40 mg BID and 5/16 on 80 mg QD) to 15 at Week 48 (7/14 on 40 mg BID and 8/16 on 80 mg QD) and 16 at Week 96 (7/14 on 40 mg BID and 9/16 on 80 mg QD); increases were also observed in MR4.5 rates (Table 4 and Supplementary Tables 12 and 13). Median duration of MR4 was not estimable.
Table 4 Response rates over time (exploratory cohort).Patient-reported outcomesCompletion rates for the MDASI-CML full questionnaire were high among patients in the main cohort, ranging from 90.9% to 94.7% at different time points. MDASI-CML Symptom and Interference Total scores decreased slightly from baseline (with decreases generally ≤0.5) and quickly at Week 4, denoting a small improvement in patients’ symptoms and slightly reduced interference with their daily life activities; no worsening in scores from baseline was noted at any timepoint up to Week 96 (Supplementary Fig. 4). Similar completion rates (88.9% to 100%) and results were observed for patients already in MMR at baseline, although the reduction in scores appeared larger for Interference Total scores (Supplementary Fig. 5).
SafetyIn the main cohort, median exposure to asciminib was 115.1 weeks (range 1.4‒154.6) for all patients, 114.9 weeks (range 2.6‒151.6) for patients on 40 mg BID and 115.2 weeks (range 1.4‒154.6) for patients on 80 mg QD. Most patients (76.8%) were exposed to asciminib for at least 96 weeks (75.0% with asciminib 40 mg BID and 78.6% with asciminib 80 mg QD).
Overall, 94.0% of these patients experienced any-grade AEs (94.0% on both 40 mg BID and 80 mg QD) and 37.5% of patients experienced Grade ≥3 AEs (32.1% on 40 mg BID and 42.9% on 80 mg QD) (Supplementary Table 14); the most frequent AEs are presented in Table 5. AEs led to treatment discontinuation in 12 (7.1%) patients (seven patients in the 40 mg BID arm and five patients on the 80 mg QD arm); these AEs were thrombocytopenia (n = 3), decreased platelet count (n = 2), neutropenia, splenomegaly, pericardial effusion, blurred vision, electrocardiogram QT prolonged, hyperlipasemia, cerebrovascular accident, headache, and cough (reported in one patient each). AEs leading to dose adjustment or interruption were reported in 57 (33.9%) patients (29 patients on 40 mg BID and 28 patients on 80 mg QD).
Table 5 Most frequent AEs (reported in ≥5% of all patients, main cohort).Among the 168 treated patients in the main cohort, pancreatic enzyme elevations were observed in 22 patients (13.1%) overall, 16.7% on 40 mg BID and 9.5% on 80 mg QD. Of these, there were two Grade 3 increased lipase (1.2%) and one Grade 3 hyperlipasemia (0.6%) events. Pancreatitis was not reported in this cohort. Eleven arterial occlusive events (AOEs) were reported (four on 40 mg BID and seven on 80 mg QD), of which four were Grade ≥3 (two in each arm).
One on-treatment death was reported in the 80 mg QD arm, caused by cerebrovascular accident on Day 11 in a 66-year-old female patient with concurrent type 2 diabetes mellitus, hypertension and a history of stroke two years before entering the study, who had been treated with losartan, bisoprolol, metformin and acetylsalicylic acid (as preventive therapy for stroke). The patient had previously received imatinib, nilotinib and dasatinib. This death was assessed by investigators as not suspected to be related to the study drug.
Among patients in the main cohort who received asciminib at 200 mg QD, 67.5% experienced at least one AE after dose escalation, with 10.0% reporting Grade ≥3 AEs. After dose escalation, the most common AE of special interest (AESI) was gastrointestinal toxicity (7/40 patients, 17.5%), with no Grade ≥3 events recorded. No AEs leading to discontinuation or deaths were reported for these patients.
Among patients in the exploratory cohort (already in MMR at baseline), median exposure to asciminib was 127.1 weeks (range 1.1‒151.1) for all patients, 127.1 weeks (range 77.7‒151.1) on 40 mg BID and 125.1 weeks (range 1.1‒146.0) on 80 mg QD; 90.0% of patients were exposed to asciminib for at least 96 weeks. Nearly all patients (96.7%) experienced any-grade AEs and 14 patients (46.7%, six on 40 mg BID and eight on 80 mg QD) experienced Grade ≥3 AEs (Table 6 and Supplementary Table 15). Two patients had AEs leading to discontinuation (Grade 3 acute pancreatitis and Grade 3 lipase increase, n = 1 each, both in the 80 mg QD arm) and nine patients had AEs leading to dose adjustment or interruption (five patients on 40 mg BID and four patients on 80 mg QD). Lipase increase was reported in four patients (13.3%) and amylase increase was reported in two patients (6.7%); of these, two increased lipase events were Grade ≥3 (6.7%).
Table 6 Most frequent AEs (reported in ≥10% of all patients, exploratory cohort).One death was reported in this cohort in the 40 mg BID arm, occurring on Day 552 of the study (52 days after the last dose of asciminib had been received). The patient was a 66-year-old male, and the cause of death was hypoxemic respiratory failure. This death was also assessed by investigators as not suspected to be related to the study drug.
BCR::ABL1 mutationsThe presence of BCR::ABL1 mutations was assessed at baseline in patients from the main cohort (Supplementary Table 16). Overall, 25 patients (14.8%) were identified as harboring a mutation before treatment with asciminib started. The most common mutation was Y253H (n = 6), followed by M244V and T315I (n = 4 each), and E255K and G250E (n = 3 each). Among patients with BCR::ABL1 mutations at baseline, 15/25 patients discontinued treatment (M244V and T315I, n = 4 each; E255K, n = 3); none of these patients had achieved MMR. Of the ten patients with BCR::ABL1 mutations at baseline still receiving treatment at data cutoff (Y253H, n = 6), seven had achieved MMR by Week 48 and one by Week 96, while the remaining two patients had BCR::ABL1IS < 1% at Week 84. Patients harboring Y253H (n = 2), F317L (n = 1), E255K (n = 1), and M244V/G250E (n = 1) mutations had their asciminib dose escalated to 200 mg QD (Supplementary Table 16).
Nine patients had newly emerging mutations detected post-baseline (M244V, n = 3; T315I, P465A, A68P/F317L, K294E, A433T, F359V, n = 1 each) (Supplementary Table 17). Of these, seven patients discontinued treatment, and two received asciminib at the increased dose of 200 mg QD.
All but one of the seven patients with an M244V mutation at baseline or emerging on treatment discontinued asciminib. On the other hand, all six patients harboring the Y253H mutation at baseline were receiving treatment with asciminib at data cutoff; four of these patients achieved MMR at Week 48, and the remaining two had BCR::ABL1IS < 1%.
Comments (0)