Study Design
ONWARDS 1, 4, and 6 were randomised, multinational, open-label, active-controlled, parallel-group, two-armed, treat-to-target phase 3a studies in adults (≥ 18 years) with T1D or T2D. Detailed methodologies for each study have been published earlier [10, 14, 15], and key study characteristics are presented in Table 1. Multiple sites across India participated in the studies, including nine sites each in ONWARDS 1 and 4 and six sites in ONWARDS 6. Inclusion and exclusion criteria for each study are provided in Supplementary Table S1. At randomisation, all participants received a glucometer (Accu-Chek®, Roche Diabetes Care) for self-monitoring their blood glucose levels, and a continuous glucose monitoring (CGM) device (Dexcom G6, Dexcom). The study included participants from the Indian population, with its regional focus being Asia. The use of CGM devices adhered to manufacturer specifications, ensuring data integrity under prevailing Indian climatic conditions, including temperature variations. CGM data collection was double-blinded in ONWARDS 1 and 4, while in ONWARDS 6 it was open.
Table 1 Key study design features of ONWARDS 1, 4 and 6ONWARDS 1 was a 78-week study, comprising a 52-week main phase followed by a 26-week extension phase and a 5-week follow-up period. The study enrolled insulin-naïve adults with T2D who were randomised (1:1) to receive either icodec or once-daily glargine U100 [10]. ONWARDS 4 was a 26-week study with a 5-week follow-up, enrolling adults with T2D previously treated with a basal-bolus insulin regimen. Participants were randomised (1:1) to icodec or glargine U100, both in combination with aspart (2–4 daily injections) [14]. ONWARDS 6 was a 52-week study consisting of a 26-week main phase, a 26-week extension phase, and a 5-week follow-up, enrolling adults with T1D previously treated with a basal-bolus insulin regimen. Participants were randomised (1:1) to icodec or degludec, both in combination with aspart (2–4 daily injections) [15]. In ONWARDS 1 and 4, background non-insulin glucose-lowering medications were allowed, except for sulfonylureas and glinides, which were to be discontinued at randomisation. In ONWARDS 1, icodec was started at 70 U per week, compared to glargine U100 at 10 U per day, with weekly dose adjustments targeting pre-breakfast glucose of 80–130 mg/dL. In ONWARDS 4, switching from daily basal insulin to icodec, the icodec dose was calculated as seven times the prior daily basal insulin dose, with a one-time additional 50% dose in the first week only. In ONWARDS 6, the icodec dose was also calculated as seven times the prior daily basal dose. Participants who had been on twice-daily basal insulin, once-daily glargine U300, or had an HbA1c < 8.0% received a one-time additional 50% dose in the first week only; other participants received a one-time additional 100% dose in their first week only. The insulin titration schedule for ONWARDS 1, 4, and 6 is detailed in Supplementary Table S2. This exploratory subgroup analysis included all Indian participants from the ONWARDS 1, 4, and 6 studies.
Outcomes
The primary endpoint was the change in HbA1c from baseline: assessed at week 52 for ONWARDS 1, and at week 26 for both ONWARDS 1 and 6, corresponding to the end of main study phases. Additionally, as part of a pre-specified analysis, changes in HbA1c from baseline were assessed at week 78 in ONWARDS 1 and at week 52 in ONWARDS 6. Changes from baseline in fasting plasma glucose (FPG) were analysed at week 52 and week 78 in ONWARDS 1, week 26 in ONWARDS 4, and at weeks 26 and 52 in ONWARDS 6. Weekly insulin dose was analysed at weeks 50–52 and 76–78 in ONWARDS 1, weeks 24–26 in ONWARDS 4, and weeks 24–26 and 50–52 in ONWARDS 6.
Continuous glucose monitoring endpoints were evaluated at weeks 48–52 and 74–78 in ONWARDS 1, weeks 22–26 in ONWARDS 4, and weeks 22–26 and 48–52 in ONWARDS 6. CGM evaluations included the proportion of time above range (TAR; > 180 mg/dL), time in range (TIR; 70–180 mg/dL), and time below range (TBR; < 54 mg/dL). The numbers of clinically significant hypoglycaemic events (level 2; glucose level < 54 mg/dL confirmed by a blood glucose meter) and severe hypoglycaemic events (level 3; hypoglycaemia with severe cognitive impairment requiring external assistance for recovery) or combined clinically significant or severe hypoglycaemia were reported. Safety endpoints, including hypoglycaemia and other adverse events (AEs), were collected throughout the treatment and 5-week follow-up periods, extending to week 83 in ONWARDS 1, week 31 in ONWARDS 4, and week 57 in ONWARDS 6. Additional assessments included the proportion of participants achieving HbA1c < 7.0% and changes in body weight from baseline, analysed at weeks 52 and 78 in ONWARDS 1, week 26 in ONWARDS 4, and weeks 26 and 52 in ONWARDS 6.
Statistical Analysis
Demographic data were summarised descriptively. The analyses were based on the full analysis set (FAS, all randomised participants) unless specified otherwise, with missing values imputed by multiple imputations. Efficacy endpoints were assessed during the ‘in-trial’ period (randomisation to last contact, withdrawal, or death) using an analysis of covariance (ANCOVA), with variations in the model’s configuration across the three studies. CGM parameters were evaluated during the ‘in-trial’ period using an analysis of variance (ANOVA) model for TIR and TAR and a negative binomial regression model for TBR. Safety endpoints (hypoglycaemia and AEs) were summarised descriptively using the safety analysis set (SAS; randomised participants receiving at least one treatment dose), assessed during the main-on-treatment and on-treatment periods. The number of hypoglycaemic events and proportion of participants achieving HbA1c < 7.0% were analysed using a negative binomial regression model.
Efficacy Outcomes
For HbA1c and FPG, the ANCOVA models included treatment as a fixed factor and baseline response as a covariate for all three studies (ONWARDS 1, ONWARDS 4, and ONWARDS 6). Additional fixed factors included personal CGM device in ONWARDS 4; and HbA1c group at screening, and pre-study basal insulin treatment in ONWARDS 6.
For CGM parameters (TIR and TBR), the ANCOVA models included treatment as a fixed factor across all three studies (ONWARDS 1, ONWARDS 4, and ONWARDS 6). Additional factors included a personal CGM device in ONWARDS 4; HbA1c group at screening, and pre-study basal insulin treatment in ONWARDS 6. For TBR, time spent is analysed using a negative binomial regression model (log link) on the number of recorded measurements in a given range. The model had fixed factors that were similar to those for respective TIR and TAR, and the logarithm of the total number of recorded measurements as an offset.
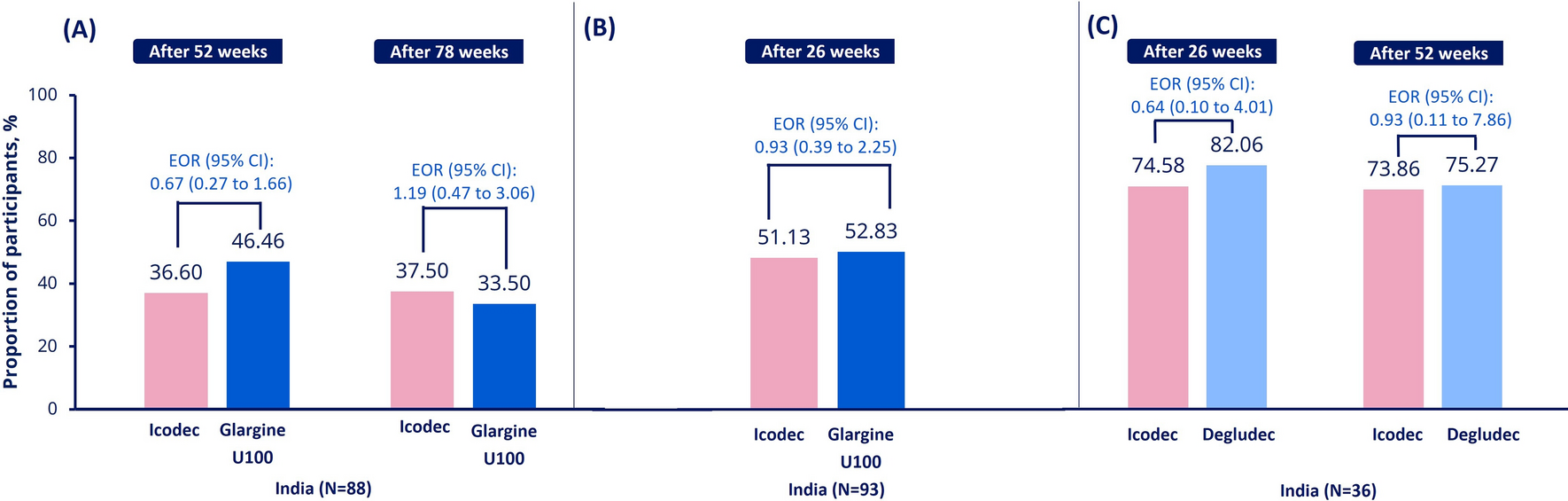
For the proportion of participants achieving HbA1c < 7.0%, the binary responses after week 52 (ONWARDS 1) or week 26 (ONWARDS 4 and 6) were analysed using a binary logistic regression model (logit link). The model included treatment as a fixed factor and baseline HbA1c as a covariate. Additional fixed factors were similar to the ANCOVA model used for assessing changes in HbA1c. Missing HbA1c measurements were imputed using the same method as specified for the primary analysis before the target achievement criterion was applied.
The mean weekly insulin dose was log-transformed and analysed using an ANOVA (ONWARDS 1) or ANCOVA (ONWARDS 4 and 6) model with variations in the model’s configuration. For ONWARDS 1, treatment as a fixed factor; for ONWARDS 4, treatment and personal CGM device use as fixed factors, and log-transformed screening response as a covariate; for ONWARDS 6, treatment, HbA1c group at screening, and pre-study basal insulin treatment as fixed factors, and baseline response as covariate.
Safety Outcomes
Hypoglycaemic events were analysed by category using a negative binomial regression model with log-link function. The logarithm of time period for which events are considered was used as an offset. Fixed factors were treatment in ONWARDS 1; treatment, and personal CGM device use in ONWARDS 4; treatment, HbA1c group at screening, and pre-study basal insulin treatment in ONWARDS 6.
Ethics
The studies were conducted in accordance with the Declaration of Helsinki, Good Clinical Practice guidelines and International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use. Before initiation of the studies, the protocol, consent form, and subject information sheets were reviewed and approved by the appropriate health authorities and an independent ethics committee/institutional review board, in compliance with local regulations. All protocol amendments and subsequent versions were also reviewed and approved, where required, in compliance with local regulations before implementation.


Comments (0)