This is one of the first studies utilizing real-world data (RWD) to examine differences in HbA1c and weight outcomes among GLP-1 RA naïve and non-naïve patients with T2D initiating either tirzepatide or injectable semaglutide.
Comparison with Clinical Trials
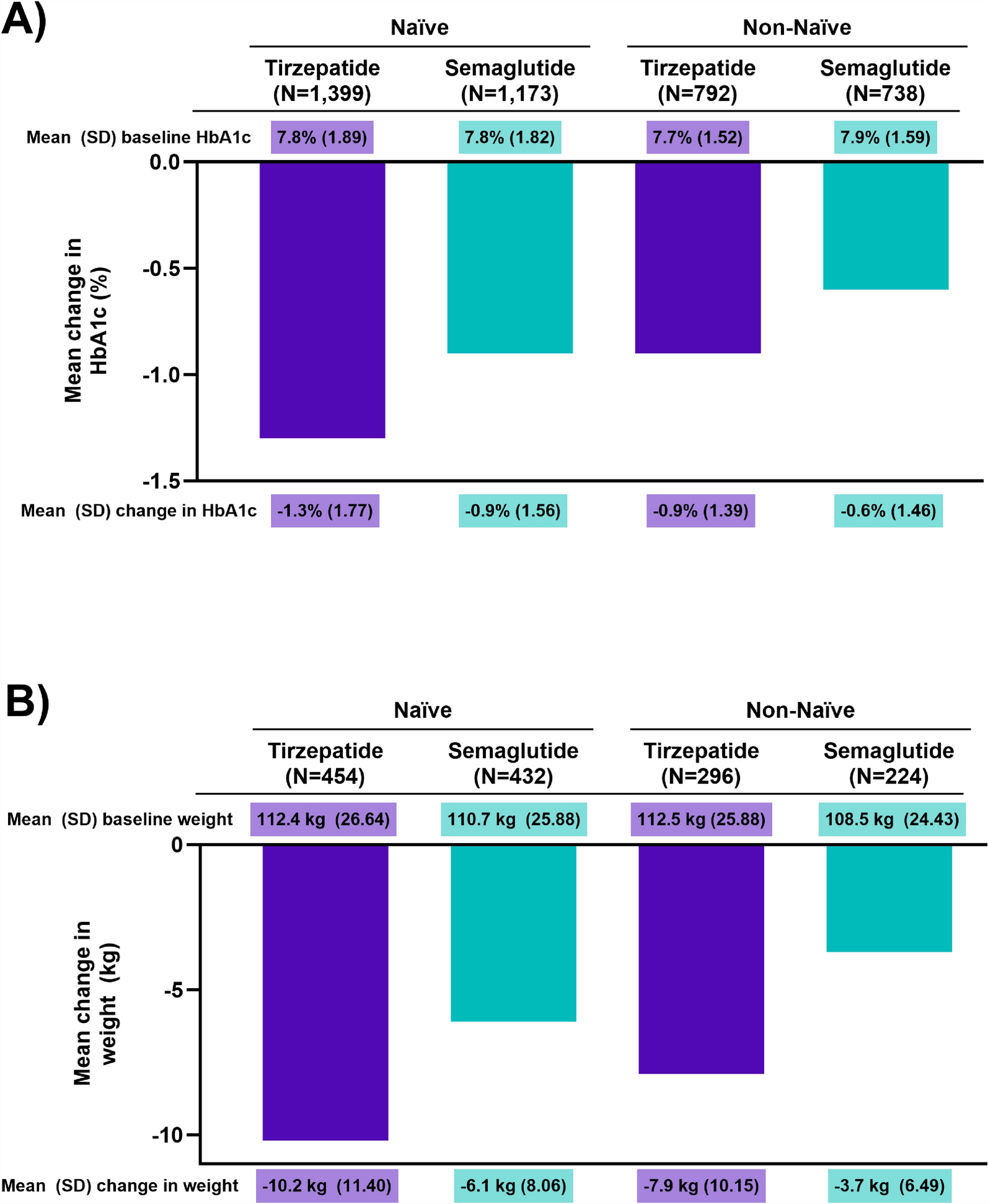
Our findings align with previous clinical trials that report blood sugar control and weight reduction with both tirzepatide and semaglutide [21, 33]. This study’s results are aligned with the head-to-head SURPASS-2 phase 3 clinical trial in naïve participants, though with some differences [21]. Reductions in HbA1c were less pronounced than those in SURPASS-2, where mean changes from baseline in HbA1c were: – 2.01% for 5 mg, – 2.24% for 10 mg, – 2.30% for 15 mg tirzepatide, and – 1.86% for 1 mg semaglutide. This study observed – 1.3% in naïve tirzepatide initiators, and – 0.9% for naïve semaglutide. Despite this, the difference in HbA1c reduction between the treatments was similar across both studies: – 0.15%, – 0.39%, and – 0.45% for the respective tirzepatide doses versus semaglutide in the clinical trial, and – 0.4% for all doses in the naïve cohort in this study. In the SWITCH-2 study, participants who switched to tirzepatide 5 mg from GLP-1 RAs experienced an additional HbA1c reduction at week 12 with tirzepatide (0.43%) versus semaglutide (0.36%), also aligned with the results from the current analyses [33]. The weight loss results from the current analyses are similarly aligned with clinical trials, however less pronounced as SURPASS-2 reported a mean weight change from baseline of – 7.6 kg, – 9.3 kg, and – 11.2 kg for tirzepatide doses of 5 mg, 10 mg, and 15 mg, respectively and – 5.7 kg with 1 mg semaglutide [21]. In the current study, the reductions observed were – 10.2 kg for naïve tirzepatide, – 7.9 kg for non-naïve tirzepatide, – 6.1 kg for naïve semaglutide, and – 3.7 kg for non-naïve semaglutide.
These differences may be due to SURPASS-2’s stringent criteria, including only treatment-naïve patients with baseline metformin usage. This group typically responds well to weight and glucose control interventions, unlike the diverse participants in our real-world study. The current population also had lower HbA1c and higher body weight at baseline compared to SURPASS-2, likely due to the more stringent inclusion/exclusion criteria of the clinical trial. Additionally, the controlled setting of clinical trials includes factors like strict regimen adherence and frequent monitoring, which differ from real-world conditions where variability in adherence is common due to behavior, health care access, and socioeconomic factors. Patients may not reach or maintain high doses of medication, potentially leading to the underestimation of treatment benefits in real-world scenarios [34, 35].
Finally, the SURPASS-2 trial analyzed each tirzepatide dose separately (5 mg, 10 mg, and 15 mg), providing a detailed dose–response relationship. Conversely, our study observed a pooled cohort across various dosages, possibly diluting specific dose-related effects. Moreover, the introduction of the 2-mg semaglutide dose in real-world settings may introduce variations in patients’ outcomes, thereby potentially affecting comparative efficacy.
The relationship between sex and weight loss among individuals with T2D using incretin-based therapies has been reported previously. In a recent post hoc analysis of the SURPASS 1–5 tirzepatide clinical trials [36] female participants achieved the composite endpoint (HbA1c < 6.5%, and weight loss target of ≥ 10%) at higher rates than male participants across the five trials. These observations have been hypothesized to be due to a higher medication exposure among women, i.e., increased plasma concentration of the treatment due to their lower mean body weight. The current analyses utilized PS matching of the cohorts to minimize any differences in sex distribution between study cohorts; a subgroup analysis by sex was outside the study’s scope.
Comparison with Prior Real-World Evidence
The exploration of tirzepatide versus semaglutide effectiveness has been informed by a few other real-world studies. Rodriguez et al. examined the effects of tirzepatide and semaglutide on weight change in GLP-1 RA naïve patients with overweight or obesity [37]. After 12 months, PS-matched patients on tirzepatide showed a 15.3% bodyweight reduction, while semaglutide patients showed an 8.3% reduction. Adjusting for residual confounding, they observed a – 6.9% difference, exceeding our naïve cohort’s finding of – 3.5%. However, both studies favored tirzepatide over semaglutide. The discrepancy in weight loss between the two studies is likely due to patient demographics. All patients in our study had a diagnosis of T2D, compared to 50% in the Rodriquez study. GLP-1 RAs tend to result in more significant weight loss for individuals without diabetes [38,39,40,41,42], likely contributing to the greater weight loss and highlighting the importance of considering patient demographics in evaluating GLP-1 RAs.
Chuang et al. reported that tirzepatide treatment was associated with lower risk of all-cause mortality, adverse cardiovascular events, acute kidney injury, and adverse kidney events compared to GLP-1 RAs in patients with T2D [43]. They observed a body weight loss difference of – 2.9 kg between tirzepatide and GLP-1 RAs, although the specific GLP-1 RA was not identified, limiting direct comparison with our study. While specific mortality, cardiovascular, and renal outcomes were not the focus in the current study, the comparable changes in absolute weight observed for both naïve and non-naïve cohorts suggest similar effects for patients with these comorbidities.
Clinical Significance and Future Directions
The differences in HbA1c and weight reduction suggest that tirzepatide’s dual agonism may offer improved glycemic control and weight loss benefits for patients with T2D compared to a single agonist like semaglutide, potentially reducing diabetes-related complications. Clinicians should consider these differences, especially for patients struggling with both weight management and glycemic control, to optimize individualized treatment. Future research should explore tirzepatide and semaglutide’s long-term effects on cardiovascular outcomes, mortality, and quality of life across diverse populations. Studying subgroup (e.g., age, gender, and baseline weight) responses could enhance personalized medicine by identifying patients likely to benefit most from each treatment.
Strengths and Limitations
Our study provides insights into the performance of these treatments beyond controlled clinical trials. The study’s inclusion of a diverse patient cohort, including those with multiple comorbidities and varying GLP-1 RA doses, reflects the complex health scenarios encountered in routine clinical practice and enhances the generalizability of its findings. Furthermore, patients were categorized by previous (within 6 months) GLP-1 RA use to include both populations and account for the potential confounding of outcomes. Large sample sizes and various robustness analyses strengthen the study's conclusions. Additionally, previous comparator trials did not include semaglutide at its highest dose of 2 mg, which was included in the current analysis.
The study also has limitations, including a 12-month follow-up, which may not reflect the complete clinical impact of T2D a chronic condition requiring long-term treatment. Administrative claims data, which are primarily used for billing, may contain diagnostic or treatment inaccuracies due to coding errors or undocumented medication use and exclude free samples and over-the-counter drugs. For instance, a 6-month washout period is clinically sufficient to capture prior GLP-1 RA exposure, yet out-of-pocket purchased medications (including compounded GLP-1 RAs) are unaccounted for. Other relevant factors, such as provider preferences, health plan details, and specific patient characteristics (e.g., social needs, family history), are unavailable, potentially leading to unmeasured confounding. The study’s focus on commercially insured patients may limit generalizability, as such individuals may differ from those with public or no insurance. Exclusion of groups of patients with gestational diabetes, type 1 diabetes, specific surgeries, or pregnancy may further limit generalizability. Continuous enrollment requirements might introduce immortal time bias as outcomes for patients with less than 12 months of follow-up are not included, and selection bias might arise from including only patients with available laboratory results and EHRs. However, we expect these biases to affect both treatment arms similarly. Additionally, analyses of the baseline demographics of patients with baseline and follow-up HbA1c and weight measurements, presented in Table S2, indicate minor imbalances between groups after PS matching; regression models fitted as a sensitivity check verified the original results [29].


Comments (0)