
Remember me
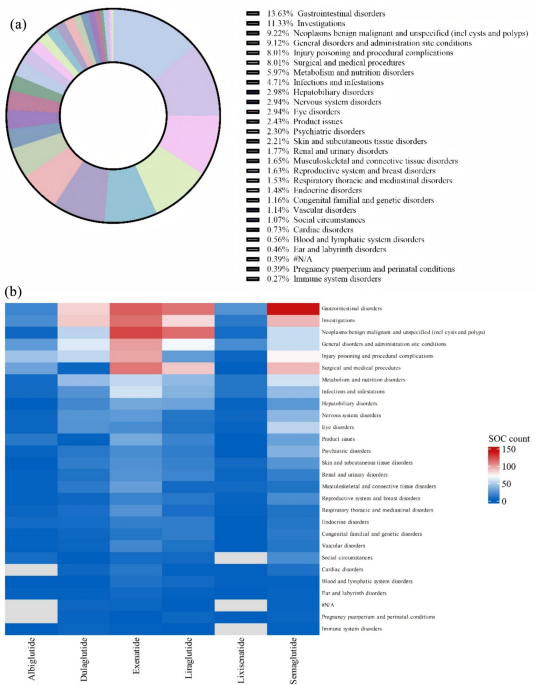
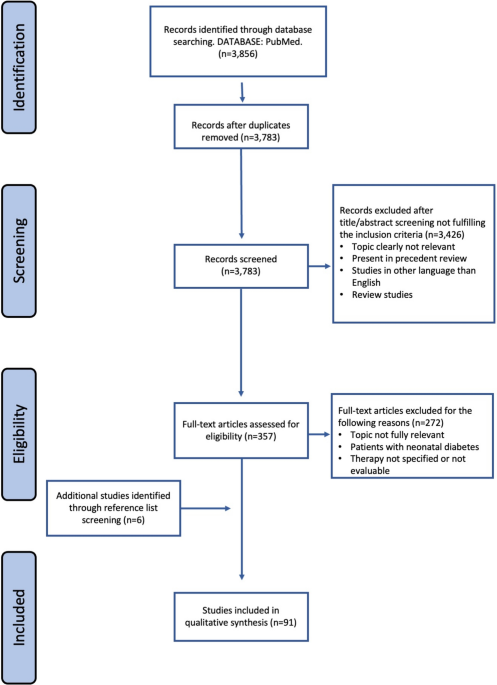
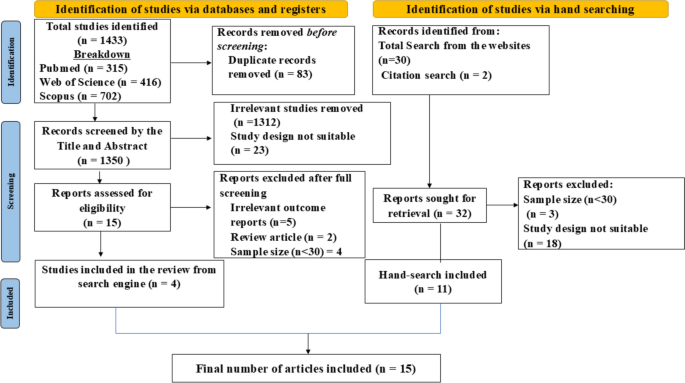
Figure 1 demonstrates key best practice recommendations for GM, including SMBG frequency targets by diabetes type and treatment regimen.
Fig. 1 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Algorithmic flowchart: best practice recommendations for GM, including SMBG frequency targets by diabetes type and treatment regimen. *Recommended monitoring frequencies represent minimum targets for optimal outcomes. Increased frequency may yield additional clinical benefits, especially during periods of therapeutic adjustment or instability. #Laboratory-based plasma glucose/HbA1c testing are not day-to-day monitoring modalities and are used only as clinically indicated. $HbA1c—point-of-care glucose testing (finger-prick testing). GM: glucose monitoring, SMBG: self-monitoring of blood glucose, CGM: continuous glucose monitoring, T1D: type 1 diabetes, T2D: type 2 diabetes, GDM: gestational diabetes mellitus
Utilization of GM Modalities Across AsiaBGM practices across Asia are evolving, with CGM increasingly used alongside SMBG and HbA1c testing [16,17,18,19]. CGM is recommended by the American Diabetes Association (ADA) and International Diabetes Federation (IDF) for insulin-treated individuals (including those with T1D and insulin-treated T2D) and those at high risk of hypoglycemia, particularly those treated with insulin or sulfonylureas regardless of diabetes type. This recommendation is supported by robust clinical evidence, including the DIAMOND randomized trial, which demonstrated that CGM significantly improves glycemic outcomes in insulin-treated adults with T1D. Real-world evidence further reinforces these clinical benefits [17]. The COMISAIR study demonstrated that adults with type 1 diabetes using CGM achieved significantly greater improvements in HbA1c and time-in-range than those relying solely on SMBG, regardless of insulin delivery method. Multiple real-world cohorts have similarly shown sustained reductions in hypoglycemia, improved treatment satisfaction, and better long-term glycemic outcomes with CGM use [20]. However, its adoption remains limited because of affordability, infrastructure gaps, and inconsistent/lack of reimbursement [5, 16, 21]. SMBG continues to be widely accepted, particularly in LMICs, owing to its accessibility and familiarity [5].
Expert insights reflected uniform agreement that SMBG, CGM, and laboratory-based glucose/HbA1c testing are all routinely used in clinical practice. In the pre-meeting survey, experts indicated that SMBG remains the most commonly recommended modality overall, particularly for individuals with type 2 diabetes managed with non-insulin therapies. CGM was consistently preferred for people with type 1 diabetes and insulin-treated type 2 diabetes, while laboratory-based testing was viewed as a complementary, periodic assessment tool rather than a day-to-day monitoring method. Finger-prick point-of-care HbA1c and 1,5-anhydroglucitol tests were rarely used. Item-level details are provided in Supplementary Table S6. Usage patterns vary by diabetes type and treatment regimen. Experts agreed that for type 1 diabetes, CGM and HbA1c are generally preferred, while SMBG remains widely used as a complementary method. In contrast, for type 2 diabetes treated with insulin, experts generally regarded SMBG and HbA1c as the most commonly used monitoring approaches, while CGM was mentioned less frequently. For type 2 diabetes managed with non-insulin therapies, SMBG and HbA1c remained dominant modalities. Although CGM is rarely used for individuals with type 2 diabetes managed with non-insulin therapies, experts noted its potential value in select cases, particularly for those on sulfonylureas with hypoglycemia risk or undergoing intensive lifestyle modifications. In such contexts, CGM can provide actionable trend data to inform therapeutic decisions and enhance safety [16]. In gestational diabetes, all three modalities were used more evenly, reflecting a balanced approach based on clinical goals and patient needs.
These expert recommendations are consistent with published evidence supporting structured SMBG for non-insulin-treated type 2 diabetes, as demonstrated in the STeP and PRISMA trials [9, 10]. Experts emphasized that SMBG remains a widely accessible and affordable strategy, hybrid models combining CGM and SMBG for calibration or confirmation are increasingly recognized as pragmatic solutions, especially in resource-constrained settings [16].
A recent umbrella review [20] confirmed CGM’s efficacy in improving glycemic outcomes but found no significant impact on patient-reported outcomes, reinforcing the continued relevance of SMBG in patient-centered care. Additionally, a Malaysian quasi-experimental study [19] showed that a structured SMBG program integrated with a mobile app significantly improved glycemic outcomes. Participants using the connected glucometer and receiving regular follow-up support experienced a reduction in HbA1c from 7.7% ± 1.1% to 7.3% ± 1.3% (p = 0.008), while the control group showed deterioration in glycemic control. These findings highlight the value of SMBG in both physiological and psychosocial aspects of diabetes management. Emerging modalities such as point-of-care HbA1c testing enables rapid, on-site glycemic assessment and may support timely clinical decisions.
In summary, while CGM is gaining clinical endorsement, SMBG remains foundational because of affordability and accessibility. Expert insights and published evidence converge on the need for a patient-centered, context-specific approach to BGM, one that balances clinical efficacy with accessibility and affordability.
Recommendation
CGM for insulin-treated or high-risk patients
Structured SMBG for non-insulin-treated patients with T2D
Hybrid CGM–SMBG models where feasible
Monitoring Frequency and Clinical Decision-MakingA recent 2024 Asia–Pacific consensus highlights the evolving role of glucose monitoring in diabetes care, emphasizing the need for individualized strategies based on patient profiles and regional healthcare contexts [16]. While CGM is gaining global traction as a complement to HbA1c and SMBG, its adoption in Asia–Pacific is shaped by distinct challenges: limited infrastructure and access in settings with constrained healthcare resources, inconsistent reimbursement policies, cultural barriers to technology use, and affordability and familiarity with SMBG in clinical practice. These factors highlight the importance of region-specific guidelines and hybrid models that prioritize accessibility, patient preferences, and local resource realities over wholesale adoption of Western protocols [16].
Recent evidence from an Asia-based meta-analysis underscores the clinical relevance of SMBG in individuals with type 2 diabetes who are not on insulin therapy. The study by Zou et al. [22] highlights that structured SMBG defined by consistent timing and frequency (typically 8–11 checks per week) is associated with significantly improved glycemic outcomes compared to unstructured or no monitoring practices. Specifically, the meta-analysis reported a mean HbA1c reduction of − 0.27% (95% CI − 0.49 to − 0.04; P < 0.018) when structured SMBG data were actively used to guide therapeutic adjustments [22]. These findings reinforce the importance of aligning SMBG practices with individualized treatment goals and patient capacity, suggesting that structured monitoring can serve as a valuable tool in optimizing glycemic control even in the absence of insulin therapy [23].
Diagnostic selection in diabetes care depends on several clinical and practical factors, including the type of diabetes, whether the patient is on insulin, and the frequency of hypoglycemic episodes, with those experiencing frequent lows or requiring intensive monitoring being ideal candidates for CGM. Clinicians often recommend CGM when starting any intervention, regardless of insulin use, as it helps both patients and providers observe the direct impact of management on glucose control. CGM offers dynamic insights, but its use remains limited in many settings because of previously discussed access barriers.
For individuals with type 1 diabetes, experts recommend frequent monitoring, typically ranging from three to ten times per day, to support insulin titration and prevent glycemic excursions. In patients with type 2 diabetes on insulin, two to five daily checks are typically sufficient, with flexibility for more frequent monitoring when clinically indicated. For individuals managed with non-insulin therapies, SMBG may be performed less frequently, such as weekly or based on symptoms, with structured monitoring during periods of therapeutic adjustment or instability. Gestational diabetes management is anchored in four-point daily monitoring (fasting and postprandial), with some cases requiring expanded profiles. Pediatric patients often require three to five daily checks, while older adult patients may benefit from symptom-based or less frequent monitoring, adjusted according to medication regimen, cognitive function, and caregiver support (as shown in Fig. 2).
Fig. 2 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Recommended GM monitoring frequency. GM: glucose monitoring, CGM: continuous glucose monitoring, GDM: gestational diabetes mellitus
Recommendation
Customize monitoring frequency by diabetes type and treatment
Use structured SMBG and CGM–SMBG hybrids during therapy changes or instability
Outcomes and Value of SMBGBGM plays a pivotal role in diabetes management by enabling timely therapeutic adjustments, improving glycemic control, and enhancing patient engagement. Across LMICs, where access to advanced technologies may be limited, a context-specific approach to BGM is essential. Within this framework, structured SMBG remains highly relevant and widely adopted.
Recent evidence from Asia reinforces the value of SMBG in improving both physiological and psychosocial outcomes. The same Malaysian quasi-experimental study also reported meaningful improvements in emotional functioning and diabetes-related quality of life, highlighting that structured SMBG supports not only physiological outcomes but also psychosocial well-being [19].
Complementing these findings, a systematic review and meta-analysis of digital SMBG interventions across Asia revealed consistent improvements in HbA1c (mean difference − 0.52%, 95% CI − 0.63% to − 0.42%; p < 0.001), fasting blood glucose, postprandial glucose, and BMI among individuals with T2D [24]. These outcomes were attributed to frequent SMBG supported by responsive healthcare guidance, underscoring the importance of integrating SMBG into digital health ecosystems. Additionally, structured SMBG has been shown to reduce hypoglycemia risk and improve quality of life when used for therapeutic decision-making, particularly in insulin-treated individuals [25].
Across Asia, SMBG practices are increasingly embedded within national healthcare frameworks and education programs. In Thailand, SMBG is integrated into structured diabetes education under the Universal Health Coverage system, with patients receiving supplies for multiple daily tests. However, discontinuation of SMBG among individuals with type 1 diabetes often due to perceived routine stability has been associated with suboptimal glycemic control, reinforcing the need for sustained monitoring to support insulin titration and complication prevention. In Korea, SMBG is leveraged as a behavioral reinforcement tool, with glucose data reviewed alongside dietary habits to facilitate personalized feedback loops. This approach is often paired with quarterly HbA1c assessments, creating a dynamic framework for patient motivation and engagement. In the Philippines, SMBG serves as a preferred modality for individuals who opt for selective monitoring or are psychologically resistant to CGM, offering a less intrusive, more affordable and adaptable alternative.
Importantly, SMBG is increasingly recognized not as a lesser alternative to CGM but as a complementary modality within hybrid monitoring models. Its affordability, accessibility, and adaptability make it indispensable in diverse healthcare settings. Reframing SMBG as an empowerment strategy, one that enables individuals to understand their glucose dynamics and make informed decisions in real time supports its integration into national guidelines, reimbursement policies, and structured education programs. This evolving understanding of SMBG’s value, grounded in regional practice and supported by emerging evidence, underscores its continued relevance in modern diabetes care.
Recommended SMBG targets values by diabetes type are summarized in Table 1, which serves as a visual guide for clinical implementation.
Table 1 Recommended SMBG targets values by diabetes type [28]The broader clinical and psychosocial benefits of structured SMBG are illustrated in Fig. 3, highlighting its role in improving glycemic control, emotional well-being, reduced hypoglycemia, and patient empowerment.
1.Improved glycemic control Structured SMBG has been shown to significantly reduce HbA1c in non-insulin-treated patients with T2D, as demonstrated in the STeP (− 0.3% reduction) and PRISMA trials, both of which confirmed meaningful improvements when SMBG data were used to guide therapeutic adjustments [9, 10, 22].
2.Enhanced well-being A Malaysian quasi-experimental study demonstrated that structured SMBG integrated with digital follow-up significantly improved emotional functioning scores in addition to improved glycemic control, reflecting the positive psychosocial impact of SMBG [19].
3.Reduced hypoglycemia A systematic review by Pleus et al. reported that structured SMBG supports earlier detection of glycemic excursions and helps reduce hypoglycemia risk in insulin-treated individuals by informing dose adjustments and reinforcing self-management behaviors [25].
4.Patient empowerment A meta-analysis by Holmes-Truscott et al. found that structured SMBG improves self-efficacy and diabetes-related empowerment, particularly when patients are trained to interpret their readings and apply results to behavior change [26, 27].
Fig. 3 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Value of structured SMBG. SMBG: self-monitoring of blood glucose
Recommendation
Structured SMBG improves glycemic and emotional outcomes
Integrate SMBG into digital platforms and education programs for long-term engagement
SMBG Technique and EducationStructured SMBG, defined as purposeful, pre-specified monitoring over a set timeframe, has shown clinical relevance in enhancing glycemic control and patient engagement [22]. Findings from the TLR highlighted persistent gaps in SMBG technique. Common errors including inadequate handwashing, repeated use of lancets, and excessive finger squeezing, and failure to rotate finger-stick sites have been shown to contribute to inaccurate glucose readings and increased finger-site injuries. Evidence from Le Floch et al. further demonstrated that approximately 30% of individuals perform SMBG incorrectly, underscoring the need for structured, technique-focused education. A meta-analysis by Holmes-Truscott et al. reported a statistically significant HbA1c reduction (− 0.29%, 95% CI − 0.46 to − 0.11) and consistent improvements in self-efficacy, especially when SMBG data guided behavioral or therapeutic changes [26]. Optimal outcomes were noted with 8–11 tests per week, particularly when combined with lifestyle modifications [22].
Despite regular SMBG, technique often deteriorates over time, especially among individuals with long-standing diabetes [28]. These recurring issues highlight the importance of not only initial training but also repeated educational efforts, as technique errors can re-emerge over time even among previously well-trained individuals. HCPs recommend hand hygiene, site rotation, and safe lancet use to ensure accurate readings [28].
Figure 4a and b illustrate best practices for SMBG technique, including step-by-step instructions and common do’s and don’ts to support accurate and safe monitoring.
Fig. 4 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.a Step-by-step SMBG. b Four best practices for accurate SMBG technique: do’s and don’ts. SMBG: self-monitoring of blood glucose
Effective SMBG involves not only testing but also recording, interpreting, and sharing results with providers. HCPs should instruct patients to check strip expiry dates and avoid excessive finger squeezing, as this can lead to sample contamination by interstitial fluid, potentially affecting glucose readings. Given cost concerns, safe reuse of lancets may be discussed, with practical disposal methods such as using plastic bottles or clinic returns being feasible and widely adopted.
Education is key to successful SMBG. A quasi-experimental study showed that weekly sessions on diet, exercise, medication adherence, and stress management significantly improved scores on the Diabetes Self-Management Questionnaire (DSMQ), Diabetes Empowerment Scale (DES), and Patient Activation Measure (PAM) scores [27]. These tools assess self-care behaviors, confidence in managing diabetes, and patient engagement, respectively. ADA and Centers for Disease Control and Prevention (CDC) guidelines advocate for Diabetes Self-Management Education and Support (DSMES) programs that include personalized, culturally appropriate SMBG training [29].
When selecting SMBG devices, experts consistently prioritize accuracy and reliability, followed by patient comfort, safety, ease of use, and affordability factors that directly influence adherence and user experience. Device selection is influenced not only by accuracy and usability but also by the affordability constraints outlined earlier. To further improve patient comfort and sampling consistency, lancets with adjustable depth settings are preferred. These devices allow customization based on individual skin thickness, reducing pain and minimizing tissue trauma during capillary blood testing. Adjustable-depth lancets also support better technique adherence and may enhance long-term engagement with SMBG. Practical considerations such as regulatory approvals, brand reputation, and device availability also influence real-world adoption.
Increasingly, digital connectivity and data integration are seen as essential for enhancing patient engagement and clinical decision-making. Digital platforms, mobile apps, video tutorials, and telehealth are more effective than traditional materials in improving lifestyle habits, HbA1c, and medication adherence, especially when paired with remote coaching and real-time feedback [30]. Adolescents using mobile monitoring tools showed better adherence and communication than those using paper logbooks [31]. HCPs emphasized that digital and video-based content is more engaging than handouts or verbal instructions, highlighting the need for standardized, accessible educational resources to support long-term adherence.
Recommendation
Emphasize DSME for effective SMBG
Use culturally tailored education and digital tools to improve technique and self-efficacy
Choosing Between SMBG and CGMRecent evidence highlights the importance of individualized glucose monitoring strategies tailored to patient needs, healthcare access, and treatment goals. While CGM provides real-time insights and trend analysis, SMBG remains central to diabetes care in Asia, particularly in resource-constrained settings.
As previously mentioned, CGM is the preferred modality in patients with T1D; however, SMBG continues to play a critical role in insulin titration, hypoglycemia detection, and day-to-day monitoring, especially in settings where CGM is not feasible or reimbursed [20, 32].
In patients with T2D, CGM has also shown improvements in glycemic control among high-risk individuals [33]; however, structured SMBG remains relevant as shown by STeP and PRISMA demonstrating significant reductions in HbA1c and improvements in psychosocial outcomes, even in non-insulin-treated patients. SMBG remains the most accessible and familiar modality for both patients and providers, and its practicality makes it indispensable in settings where CGM access is limited. Although CGM provides richer trend information, its use remains limited in many Asian settings because of cost and access constraints; consequently, HCPs widely rely on and endorse SMBG as the more practical, affordable, and adaptable monitoring strategy in routine care.
Hybrid glucose-monitoring approaches, which combine intermittent CGM use with regular SMBG, provide a pragmatic and cost-conscious compromise in many Asian healthcare environments where continuous CGM use is not feasible. Intermittent CGM offers valuable trend insights and supports therapeutic adjustments, while SMBG remains essential for day-to-day treatment decisions. Hybrid approaches have also demonstrated meaningful clinical benefits in specific populations such as gestational diabetes. Evidence from the Steady Sugar Trial showed that early intermittent CGM use improved maternal glycemic control and was associated with lower rates of adverse outcomes, while routine SMBG supported day-to-day decision-making [34]. Together, these modalities enable improved safety, greater understanding of glucose patterns, and more accessible monitoring options for diverse patient groups. The ADA’s 2025 guidelines support such approaches, particularly for populations with limited CGM access. Ultimately, monitoring strategies should not be CGM-centric; they must reflect real-world constraints and prioritize patient-centered care. SMBG remains a vital tool in optimizing outcomes, empowering patients, and supporting equitable diabetes management across Asia [35]. Practical considerations such as app language options and locally available training materials should be evaluated to support sustained device use.
Figure 5 summarizes key considerations for choosing between SMBG and CGM, highlighting clinical scenarios, patient needs, and resource constraints that guide modality selection.
Fig. 5 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.SMBG vs CGM: finding the right fit. SMBG: self-monitoring of blood glucose, CGM: continuous glucose monitoring
Recommendation
Individualize monitoring strategies based on risk, access, and treatment goals
Hybrid CGM–SMBG models offer practical solutions in resource-limited settings
Ketone Monitoring PracticesKetone monitoring plays a supportive role in diabetes care, particularly for patients at risk of diabetic ketoacidosis (DKA). Blood ketone testing, especially for β-hydroxybutyrate (BHB), is preferred for its accuracy in detecting DKA, including euglycemic DKA in patients on SGLT2 inhibitors [36,37,38]. Despite its lower sensitivity compared to blood ketone testing, urine ketone testing remains frequently used across Asia owing to its affordability, ease of use, and shelf life, particularly in emergency situations [39].
Clinical judgment should guide selective use of ketone testing. Blood ketone meters are typically reserved for high-risk scenarios, while urine strips are used during illness, stress, or persistent hyperglycemia [39]. Forum insights support this pragmatic approach, emphasizing that ketone monitoring should be context-specific and not routine for all patients.
Recommendation
Use blood ketone testing for high-risk scenarios
Urine testing remains viable in low-resource settings
Guidelines and Implementation GapsRecent evidence from Asia highlights both the evolving role of SMBG and persistent gaps in its implementation. Structured SMBG initiatives continue to show potential to strengthen patient engagement and self-management across diverse Asian settings [19]. However, such structured practices remain largely inaccessible because of cost and limited integration into routine care. Complementing this, a multicountry survey across six LMICs, including Indonesia, reported that SMBG devices were frequently unavailable in public health facilities, and
Comments (0)