
Remember me
We conducted a systematic review in accordance with PRISMA 2020 recommendations (qualitative synthesis; no meta-analysis planned a priori). We searched PubMed for studies published from April 16, 2020 (date of the last study included in the previous review [13]) to October 11, 2025 (search last run on October 11, 2025). The full search string was: ((mody[Title/Abstract]) OR (maturity-onset diabetes of the young[Title/Abstract]) OR (HNF4A[Title/Abstract]) OR (GCK[Title/Abstract]) OR (HNF1A[Title/Abstract]) OR (Pancreatic and Duodenal Homeobox 1 -PDX1- [Title/Abstract]) OR (HNF1B[Title/Abstract]) OR (Neurogenic Differentiation 1 -NEUROD1-[Title/Abstract]) OR (Krüppel-like factor 11 -KLF11-[Title/Abstract]) OR (Carboxyl Ester Lipase -CEL-[Title/Abstract]) OR (Paired Box 4 -PAX4-[Title/Abstract]) OR (Insulin –INS-[Title/Abstract]) OR (B-Lymphocyte Kinase -BLK-[Title/Abstract]) OR (ATP-binding cassette transporter sub-family C member 8 -ABCC8-[Title/Abstract]) OR (potassium inwardly rectifying channel subfamily J member 11 -KCNJ11-[Title/Abstract]) OR (adapter protein containing PH domain -APPL1-[Title/Abstract])) AND ((treatment[Title/Abstract]) OR (therapy[Title/Abstract])). PubMed was selected as the primary database for its extensive coverage of the biomedical literature. To minimize missing studies, we also manually screened the reference lists of included articles, identifying additional relevant publications. This approach was consistent with the search strategy adopted in our previously published systematic review [13], in order to ensure methodological continuity and comparability between the original review and the present update. The selection of articles was conducted according to the PICOS framework as follows:
Population: individuals with genetically confirmed MODY (any subtype), children or adults.
Intervention/Exposure: any antihyperglycemic treatment or therapy modification after genetic diagnosis with reported outcomes.
Comparators: any (including within-patient before/after) or none for single-arm/case designs.
Outcomes: glycemic outcomes (e.g., hemoglobin A1c -HbA1c-, continuous glucose monitoring -CGM- metrics), hypoglycemia, weight or body mass index (BMI), tolerability/adverse events, pregnancy outcomes, and explicit post-genetic switches (e.g., from insulin to sulfonylurea -SU-).
Eligibility CriteriaFor this review, we included only peer-reviewed original studies (trials, cohorts, case series, case reports). Papers were eligible if the diagnosis of MODY was genetically confirmed, the treatment was defined, and outcomes were clearly reported. Additional papers were identified by a manual search of the references from the retrieved articles. Conference abstracts without full text, reviews/editorials/guidelines papers, papers without clearly reported outcomes or insufficient/fragmented data precluding extraction, and non-English language manuscripts were excluded. This review uses only previously published data and does not include research involving human participants or animals conducted by the authors.
Two reviewers (LZ, MD) independently screened titles/abstracts and full texts; disagreements were resolved by consensus. Using a piloted template, we collected: first author, year, country, study design, genetic test, MODY gene/variant, sample size, age/sex where available, treatment(s) and post-genetic therapy changes, and outcomes (HbA1c and other clinical endpoints). When multiple time points were reported, pre/post values related to therapy changes were extracted.
Outcomes and SynthesisThe primary objective of this paper is to provide an update about gene-specific treatment management by summarizing therapeutic responses and outcomes. The methodological quality of the included studies was assessed using the Newcastle–Ottawa Scale (NOS). Given the inclusion of case reports and case series, quality assessment was interpreted descriptively across study designs. The quality assessment results are displayed in the supplementary material, Tables 1–14.
Protocol and DeviationsThe methodological framework was consistent with that used in the previously published review. To further ensure transparency, the protocol for this updated review has now been registered in the PROSPERO database (registration number CRD420261328522). Methods followed those of the prior review [13], with an extended time window to October 11, 2025. Final PRISMA counts (records identified/removed/excluded/included) and any additional studies retrieved in the last search will be reported in the Results and the PRISMA flow-chart. The PRISMA 2020 checklist is provided as supplementary material (Table 15).
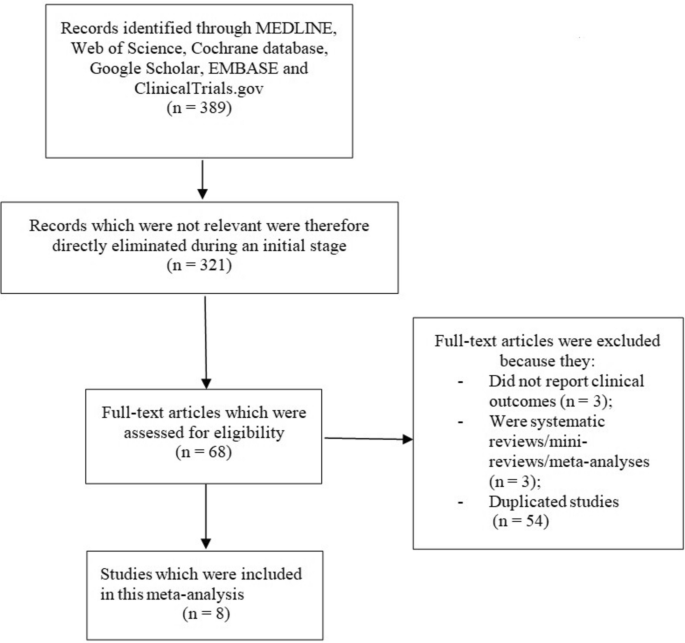
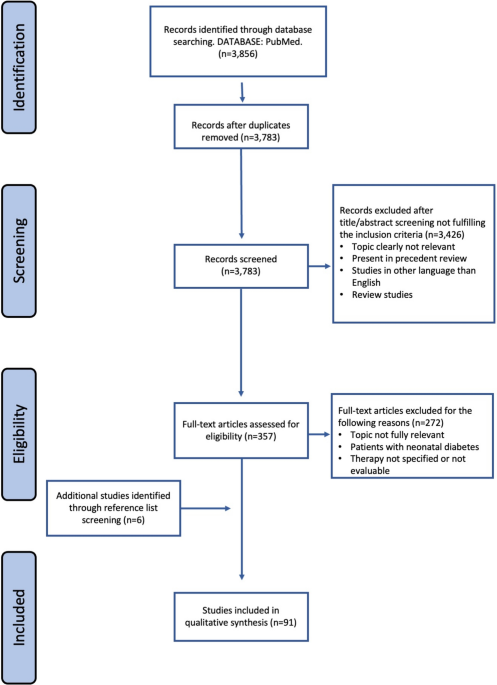
Study SelectionThe initial search yielded 3856 records. After removal of duplicates, 3783 titles/abstracts were screened, and 3426 records were excluded for not meeting the inclusion criteria. Of 357 full-text articles assessed, 272 were excluded (topic not fully relevant, neonatal diabetes, therapy not specified or not evaluable). Six additional studies were identified through reference list screening. In total, 91 studies met all inclusion criteria and were included in the qualitative synthesis (Fig. 1).
Fig. 1 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.To avoid excessive length of the manuscript, and given the lack of meaningful novelty in the pathophysiology over the last year, we do not describe in this paper the genetic defects and the pathophysiological effects, reported in our previous paper [13], but just a brief clinical presentation of each MODY subtype.
This article is based on previously conducted studies and does not contain new studies with human participants or animals performed by any of the authors.
HNF4A-MODY (Supplementary Material, Table 1)Individuals with HNF4A-MODY usually have normal or near-normal glucose tolerance in the first decade of life. Glucose intolerance typically emerges in adolescence/early adulthood alongside hormonal changes that increase insulin resistance. In early disease, when fasting glucose and HbA1c remain in the non-diabetic range, moderating dietary carbohydrate can reduce post-prandial excursions. Over time, HbA1c tends to rise, while ketosis remains uncommon owing to preserved endogenous insulin secretion. When lifestyle alone is insufficient, SUs in this genotype, often outperform insulin as first-line therapy [2]. SUs bind Sulfonylurea Receptor 1 (SUR1) subunit, closing the potassium ATP-sensitive (KATP) channel, depolarizing the β-cell membrane and promoting insulin [14, 15]. Current guidance emphasizes the high SU sensitivity of HNF4A-MODY and supports SUs as preferred initial pharmacotherapy when feasible [2].
Switches to SUs. Beyond earlier reports [16,17,18,19], additional case-based papers describe late reclassification to HNF4A-MODY with transition from insulin to low-dose SU (gliclazide/glipizide), improving HbA1c and CGM metrics [20,21,22]. Across case series and observational studies, switching from insulin to SUs consistently improves glycemic control (HbA1c 6–7%) in patients initially misdiagnosed with T1D or T2D [20,21,22,23,24,25].
Efficacy and durability of SUs. A recent HNF4A-MODY series documented clinically meaningful HbA1c reductions on SU monotherapy, with durable control during follow-up; adjunct agents such as glucagon-like peptide-1 receptor agonists (GLP-1 RAs) and sodium-glucose co-transporter inhibitors (SGLT2i) were used when BMI was higher, diabetes was longer-standing, or insulin secretory capacity was reduced [26]. In particular, in this large series (31 patients), 51.6% of the patients showed a significant reduction in HbA1c (p = 0.045) during SU treatment with stable glycemic control after 6 years of follow-up (IQR: 3.5–11). The remaining 48.4% of patients required additional therapies, such as insulin, presenting a higher BMI (p = 0.037) and a longer duration of diabetes (p = 0.03) [26]. The authors conclude that patients on just SU (mean dose 120 mg/day) were younger (p = 0.011) and presented a shorter history of dysglycemia (p = 0.019).
Alternatives or add-on to SUs. Two descriptive case series of four patients, two treated with GLP-1 RAs and two with dual gastric inhibitory peptide (GIP)/GLP-1 RAs [27], and two patients, treated with GLP-1 RAs [28], showed that these agents are effective to enable down-titration or even withdrawal of insulin or other oral hypoglycemic agents (OHAs). HbA1c decreased by 0.6–1.8% reaching the therapeutic target, BMI decreased by 1.4–5 kg/m2 and 7.4–10.4 kg/m2 in patients on GLP-1 RAs and dual GIP/GLP-1 RAs, respectively, with overall good tolerability [26]. Larger improvement (HbA1c − 2.5% and − 3.7%) was reported by Broome et al. [28]. Similar data were reported by Crowley et al. [26] in three patients treated with GLP1-RAs who showed an HbA1c decrease from 76 mmol/mol to 58 mmol/mol and a meaningful weight reduction. Even SGLT2i were shown to be effective in two patients from the same cohort, despite an increased risk of genital-urinary infection.
GCK-MODY (Supplementary Material, Table 2)GCK-MODY is the most frequent subtype of MODY worldwide. It is characterized by mild, stable hyperglycemia since birth. In our previous review, the studies supported no pharmacologic therapy for individuals with GCK-MODY [13], and more recent reports are in line with previous conclusions. In the majority of patients, diet and physical exercise are sufficient to manage mild hyperglycemia with HbA1c only slightly above the normal range [19, 29,30,31].
Excluding pregnancy studies, we identified 208 individuals with GCK-MODY: 157 were managed with diet/exercise, 17 received no therapy, 30 were on OHAs (most commonly metformin, n = 12), and 11 were on insulin, which was discontinued after genetic confirmation in most of them [18, 29,30,31,32,33,34,35,36,37,38,39,40].
Studies consistently show that GCK-MODY is characterized by mild, stable hyperglycemia at diagnosis (fasting glucose ~ 125 mg/dl, mean HbA1c around 6–7%). Most patients maintain adequate glycemic control with diet and lifestyle measures alone, while the addition of insulin or oral glucose-lowering agents (metformin, SU, GLP-1 RA, SGLT2i) provide little or no additional benefit and are often discontinued after genetic confirmation. These findings are consistent across adult and pediatric case series, cohorts, and registries, supporting early molecular diagnosis and minimal-intervention management [8, 21,22,23,24, 29, 30, 40,41,42,43,44]. This new evidence reinforces the “no routine drugs” principle outside pregnancy and confirms that in these subjects the molecular diagnosis prevents unnecessary medication.
PregnancyPregnancy is a special context of increased insulin resistance and requires gene-aware management. In a registry analysis of 54 women and 128 pregnancies, 39 insulin-treated gestations were associated with adverse events (hypoglycemia in 22 pregnancies, including nine severe), whereas no adverse events were reported in untreated gestations. Among mutation-positive fetuses, maternal insulin treatment was associated with lower birthweight than non-insulin management; among mutation-negative fetuses, birthweight did not differ between treated and untreated pregnancies [46]. In a similar study of 34 women, 59% of pregnancies were managed with diet and 41% with insulin: in GCK-unaffected offspring, cesarean section rate, birthweight and large for gestational age (LGA) prevalence were higher than in GCK-affected offspring. This is because the fetus, not inheriting the mutation, perceives maternal blood glucose as “too high”, thus increases insulin secretion and the risk of macrosomia. Insulin during pregnancy did not reduce LGA in unaffected offspring and was associated with earlier gestational age and more cesarean sections, with no effect on birthweight in affected offspring [47]. A prospective series of 41 GCK-MODY pregnancies compared insulin (n = 21) vs. diet (n = 20): hypoglycemia occurred in a substantial fraction of offspring in the insulin group, whereas no hypoglycemia or perinatal complications were reported among offspring from non-insulin pregnancies; birthweight was lower in GCK-affected newborns when mothers received insulin than when they did not, whereas unaffected neonates had higher birthweight and 33% were macrosomic [48].
Contemporary single-case reports illustrate how CGM can support diet-only management in most GCK-MODY pregnancies, with time-in-range improving across gestation and no increase in maternal hypoglycemia or neonatal complications in a pregnant woman from China [49]. Familial GCK-MODY reports similarly emphasize that, outside pregnancy, pharmacological therapy is generally unnecessary and that intrapartum insulin should be reserved for suspected non-carrier fetuses with overgrowth [24, 25, 45].
A novel oral hypoglycemic agent, dorzagliatin provides proof-of-concept for precision treatment in GCK-MODY. It is a first-in-class dual-acting glucokinase activator approved in China for the treatment of adults with T2D. It restores glucose sensitivity in pancreatic β-cells and enhances hepatic glucose utilization, thereby targeting a fundamental defect in glucose homeostasis. In a double-blind randomized placebo-controlled crossover study, eight adults with GCK-MODY (7F/1 M; age 36.1 ± 6.4 years; HbA1c 6.7 ± 0.3%) underwent a 2-h hyperglycemic clamp after a single 75 mg oral dose. Dorzagliatin lowered basal glucose versus placebo (4.6 ± 0.6 vs. 5.4 ± 0.3 mmol/l) and significantly improved second-phase insulin secretion and β-cell glucose sensitivity, with no serious adverse events (one mild hypoglycemia treated with i.v. dextrose). In an 8-year follow-up case report, dorzagliatin 75 mg twice daily reduced HbA1c from 7.4 to 6.3% at 3 months and 6.1% at 6 months, with no hypoglycemic events reported [50, 51].
HNF1A-MODY (Supplementary Material, Table 3)HNF1A-MODY typically presents in adolescence or early adulthood with progressive hyperglycemia in non-obese, autoantibody-negative individuals. A key feature is a reduced renal threshold for glucose reabsorption, leading to glycosuria at relatively low plasma glucose levels. Glycemia often shows normal or mildly elevated fasting glucose initially, with early post-prandial hyperglycemia, followed by a gradual deterioration over time. Microvascular complications may occur; therefore, carbohydrate-moderated nutrition and early SUs therapy are recommended [2]. In early disease, satisfactory control has been reported with dietary intervention alone in some carriers [29, 32, 36]. A recent Turkish pediatric MODY cohort also reported four HNF1A-MODY cases mainly managed with diet or metformin rather than sulfonylureas, highlighting heterogeneous real-world treatment patterns [42]. As disease progresses, SUs are highly effective and often provide better glycemic control than insulin, even in pediatric cases [52]. Dosing should start low (about one-quarter of typical starting doses) and can often be maintained at low maintenance doses (e.g., gliclazide 20–40 mg/day) [53, 54]. Interestingly, some recent papers explore the safety and efficacy of other OHAs in the treatment of these patients.
The superiority of SU-based therapy has been confirmed by multiple studies and case series; after genetic diagnosis, switch to SU improves glycemic control [18, 38, 55,56,57,58,59,60]. Durable, low-dose SU regimens have been reported in adolescents and young adults with sustained HbA1c between 5.5 and 6.9% on glibenclamide/glimepiride, sometimes after initial insulin exposure [48, 61, 62]. A structured switch program showed benefit across pathogenic HNF1A variants and, in 6/9 with likely-pathogenic/variant of unknown significance (VUS), despite prior insulin use; non-responders often had absent endogenous insulin or T2D criteria [63]. Similar findings were reported in other ancestries [64,
Comments (0)