This real world study demonstrates that tirzepatide caused substantial and sustained weight reduction accompanied by broad metabolic and organ-specific benefits in adults with obesity. The magnitude of these effects was significantly greater among individuals treated for more than 1 year than those treated less than 1 year. A central observation is the pronounced persistence-dependent cumulative gradient across all outcome domains, highlighting the necessity of continued therapy to achieve the full therapeutic potential of tirzepatide.
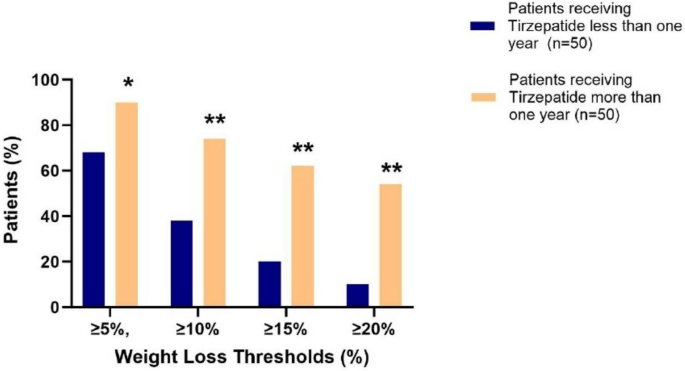
Participants who remained on therapy for more than 1 year achieved nearly twice the relative weight reduction of short-term users, with more than 60% attaining > 15% weight loss. These effects were accompanied by significant decreases in BMI and waist circumference, and were comparable between men and women. Beyond weight reduction, tirzepatide elicited marked improvements in lipid metabolism, with long-term treatment resulting in greater reductions in total cholesterol, LDL-C, and triglycerides, as well as an increase in HDL-C. Glycemic parameters improved despite normoglycemia at baseline, suggesting benefits extending to diabetes prevention. Liver transaminases declined significantly with prolonged treatment over 1 year, indicating potential hepatic benefit. Serum creatinine and blood urea nitrogen decreased in the long-term persistent group, with no significant between-group difference. Changes in microalbuminuria did not differ significantly between short- and long-term persistent participants. Correlation analyses confirmed that weight loss was strongly associated with improvements in lipid and hepatic indices, underscoring the interdependence between adiposity reduction and metabolic normalization.
The findings extend the evidence from the SURMOUNT clinical program by providing real-world confirmation of tirzepatide’s long-term multisystemic effectiveness [4]. The degree of weight reduction observed in our population is comparable to the magnitude reported in the Optum analysis, despite differences in baseline characteristics, sample size, and treatment duration [6]. Both studies suggest that real-world tirzepatide effectiveness approximates outcomes observed in the SURMOUNT clinical trials, even though dose escalation is slower and the maximum doses are often not reached.
Our results reinforce the central role of treatment persistence in mediating multidimensional benefits across the CKM continuum in adults with obesity [8]. Participants receiving tirzepatide therapy for more than 1 year experienced significantly greater reductions in body weight, BMI, waist circumference, and glycaemic control compared with those who discontinued earlier, a pattern consistent with the persistence-dependent gradient reported in SURMOUNT-1 and SURMOUNT-4 trials [1, 9].
Improvements in lipid profile in the long-term group, including significant reductions in LDL-C and triglycerides with concurrent HDL-C elevation, aligns the cardioprotective role observed in real-world analyses of tirzepatide’s phase 3 program [6]. Such atherogenic lipid attenuation translates into improved cardiovascular risk modulation, consistent with the objectives of the emerging CKM framework proposed by the American Heart Association Presidential Advisory [10].
Persistent therapy for more than 1 year led to progressive decline in hepatic transaminases (SGOT and SGPT), suggesting additional liver benefits, including potential mitigation of steatotic and inflammatory processes in metabolic dysfunction-associated steatotic liver disease (MASLD). Similar hepatoprotective effects have been reported in the SURPASS-3 trial and its Magnetic Resonance Imaging (MRI) substudy, as well as in other incretin-based intervention studies [11].
Renal function was preserved in both groups and showed a favorable persistence-dependent trend with longer treatment duration. These findings are consistent with clinical evidence showing that incretin-based therapies may exert neutral or protective renal effects through reductions in glomerular hyperfiltration, as observed in the SURPASS-4 post-hoc renal analysis [12].
Overall, in this real-world analysis, longer persistence with tirzepatide was associated with consistent and progressive improvements across anthropometric, metabolic, hepatic, and renal outcomes. These data reinforce the clinical relevance of sustained therapy to achieve the full cardiometabolic benefit of dual GIP/GLP-1 receptor agonist [13, 14] and support its role in the long-term management of obesity-related CKM dysregulation.
Study Strengths and Limitations
There are several limitations of this study. Its observational design may be subject to selection bias. The sample size was modest; however, the study was conducted within a single high-volume metabolic obesity center, where a uniform treatment protocol and standardized follow-up procedures ensured data consistency and minimized inter-site variability. Furthermore, adherence was not systematically monitored, which may influence the observed treatment effects.
A key strength of this study is that it provides the first real-world evidence from a single-center cohort with a comprehensive evaluation of persistence-dependent outcomes across the CKM spectrum. Compared to the two previously published real-world analyses (6, 7) our study provides important methodological and clinical advantages. First, by evaluating outcomes in individuals persisting on tirzepatide for more than 1 year, we directly captured a graded association with treatment duration that was not assessed in the Optum or Veradigm datasets (6,7). Second, our cohort included richer CKM phenotyping that allows more comprehensive insight into organ-level responses. Third, we demonstrated a clear hepatic signal in long term persistent group, with significant reductions in SGOT and SGPT, an outcome not characterized in the prior database analyses. Finally, by representing a Middle Eastern population, our study expands the geographic and demographic generalizability of evidence on tirzepatide use in individuals with obesity without T2DM.

Comments (0)