Our study has shown that in people with diabetes and an active CN, male sex and previous amputation were associated with an increased risk of amputation (major and minor). In addition, we reported 1-year (2.2%), 5-year (9.8%), and 10-year (13.3%) amputation rates, and 1-year (2.7%), 5-year (18.9%), and 10-year (40.0%) mortality rates. Our data suggests that having a previous amputation and a more severe CKD stage were associated with an increased risk of premature death.
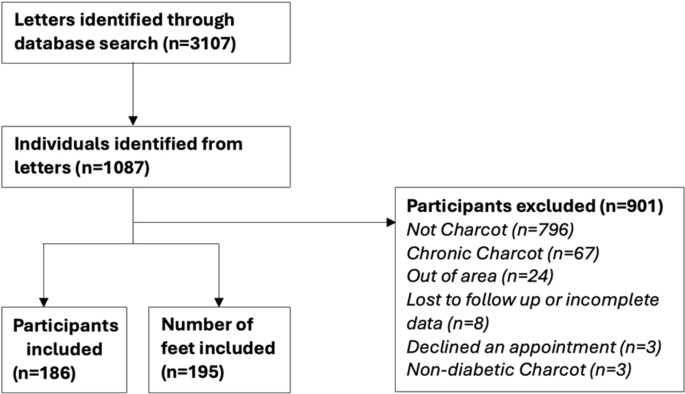
This retrospective study included 186 people with a new diagnosis of active CN between 2007 and 2022. The people included in this study are representative of those with CN as reported in other studies and case series. In agreement with previous data, our population was predominately male patients with a mean age of 60.4 (± 13.2) years [10, 11]. The most common Sanders and Frykberg stage was stage 2 (Lisfranc, tarsometatarsal joints).
There has been one recent systematic review and meta-analysis [4] and a number of studies [12,13,14,15] that have reported CN related morbidity and mortality and the associated risk factors. Sohn et al. showed that people with CN had an increased mortality compared to those with diabetes, without CN [5]. Previous work suggested no significant difference in mortality in individuals with CN compared to those with neuropathic ulcers, there was still an overall higher mortality rate in those with CN compared to controls who were matched for sex, age (± 2 years), disease type, disease duration (± 2 years) and year of referral (± 3 years) [3]. Yammine et al. supported this as they showed in their meta-analysis looking at 16 studies with a combined population of 2250 patients that 16% of people with CN went on to have an amputation, and there was a significantly higher mortality in those with CN feet and diabetic foot ulcers compared to those without any foot complications [4].
Crude Rate Comparison
The meta-analysis conducted by Yammine et al. looked at the amputation and mortality frequencies associated with diabetes related CN. The authors included similar inclusion and exclusion criteria used in the present study. They reported an overall amputation rate of 15.0% from ten studies including 871 feet, comparable to the amputation rate of our study, 15.3% from 195 feet [4].
The meta-analysis also reported an overall 1-year mortality of 4.0% (from two studies including 255 participants), a 5-year mortality of 24.5% (from seven studies including 1706 participants), and a 7 + year mortality of 16.0% (from four studies including 277 participants). In comparison, the 1-year (2.7%) and 5-year (18.9%) mortality rates of our study while numerically lower were too small to be able to suggest any statistical differences. Similarly, whereas the 10-year mortality rate (40.0%) of our study was numerically higher than the 7 + year mortality rate of the meta-analysis, possibly due to the longer follow-up period, no statistical inferences can be made [4].
A previous study from our center by Stark et al. reported the 5-year outcomes for 50 people with active CN [12]. That study reported 5-year outcomes for the whole cohort, which were an 8.0% (4/50) amputation rate and 4.0% (2/50) mortality rate. Our 5-year amputation rate 9.8% (12/122) and mortality rate 18.9% (23/122) were higher than this.
Factors Affecting Amputation
Our results showed that male sex was associated with an increased risk of amputations. This aligns with data from the USA by Ramanujam et al. who reported a higher proportion of their lower extremity amputations in male patients compared to female patients [14]. It is important to highlight that their study focused only on those who required surgery, which may mean that the CN episodes are more likely to be severe as they may have been unsuccessful with conservative treatment. Male patients have previously been shown to have a higher incidence of CN which could mean that CN episodes in male patients are more likely to progress and be more severe requiring amputation as a treatment [16].
In line with another study, our study found previous amputations were associated with an increased risk of further amputation [13]. This could be explained by non-healing, or changes to lower limb biomechanics leading to transfer ulcers which go onto require amputation [17].
Factors Affecting Mortality
Van Baal et al. previously demonstrated that the mortality of a person with a CN was the same as someone with a noninfected foot ulcer, with a median survival of 7.88 (4.0–15.4) and 8.43 (3.4–15.8) years, respectively [3]. However, previous amputations were also shown to be associated with a higher mortality rate. There are many reasons why this may be. Mortality rates are higher in those who do not regain the ability to walk after an amputation compared to those who do remobilize [18]. A person’s health status prior to amputation including age, presence or absence of renal disease, peripheral arterial disease and cardiovascular disease will all impact on mortality rates [17, 19]. Worsening CKD stage was also associated with a higher mortality rate. Studies from the USA and India have reported similar findings to our work with higher mortality rates in those with renal disease and diabetic foot complications including CN, ulcers, and infections [20, 21]. The presence of CKD is associated with increased cardiovascular risk [22].
Some of our outcomes differ to the published literature. This may be because our sample size is not large enough to observe the true effect. The participant characteristics and treatment strategies may also be different compared to other published studies. Earlier offloading or the use of non-removable versus removable offloading devices in addition to a more intense approach to the prevention and management of other risk factors, such as diabetes control, CKD or cardiovascular factors, may all improve the reported outcomes. More work is needed to further understand how these participant and CN characteristics and different treatment strategies affect the outcomes of CN.
The strengths of this study are that due to it being single centerd with a consistent approach to the treatment of CN over the 15 years of this study. As per international guidelines all cases of active CN were treated with non-removable or removable knee-high offloading devices based on clinician’s recommendations and individuals’ preference [23].
The limitations of the study are that the center was a tertiary center so there was an increased number of participants for whom long-term follow-up data was not available. This is because once the CN had gone into remission, people were discharged back to their local care provider. Another limitation of this study is that no multivariant factors have been accounted for with regards to amputations due to a low sample size. Whilse it is appreciated that risk factors are different for different types of amputation, (major or minor) data on these were not collected. Data for confounding factors such as further foot ulcer formation, cardiovascular disease, peripheral arterial disease and stroke were not collected so the results were not corrected for. There was also no control group to compare the amputation and mortality rates to. Another limitation of this study is that it was retrospective which makes the study more susceptible to incomplete data.

Comments (0)