
Remember me
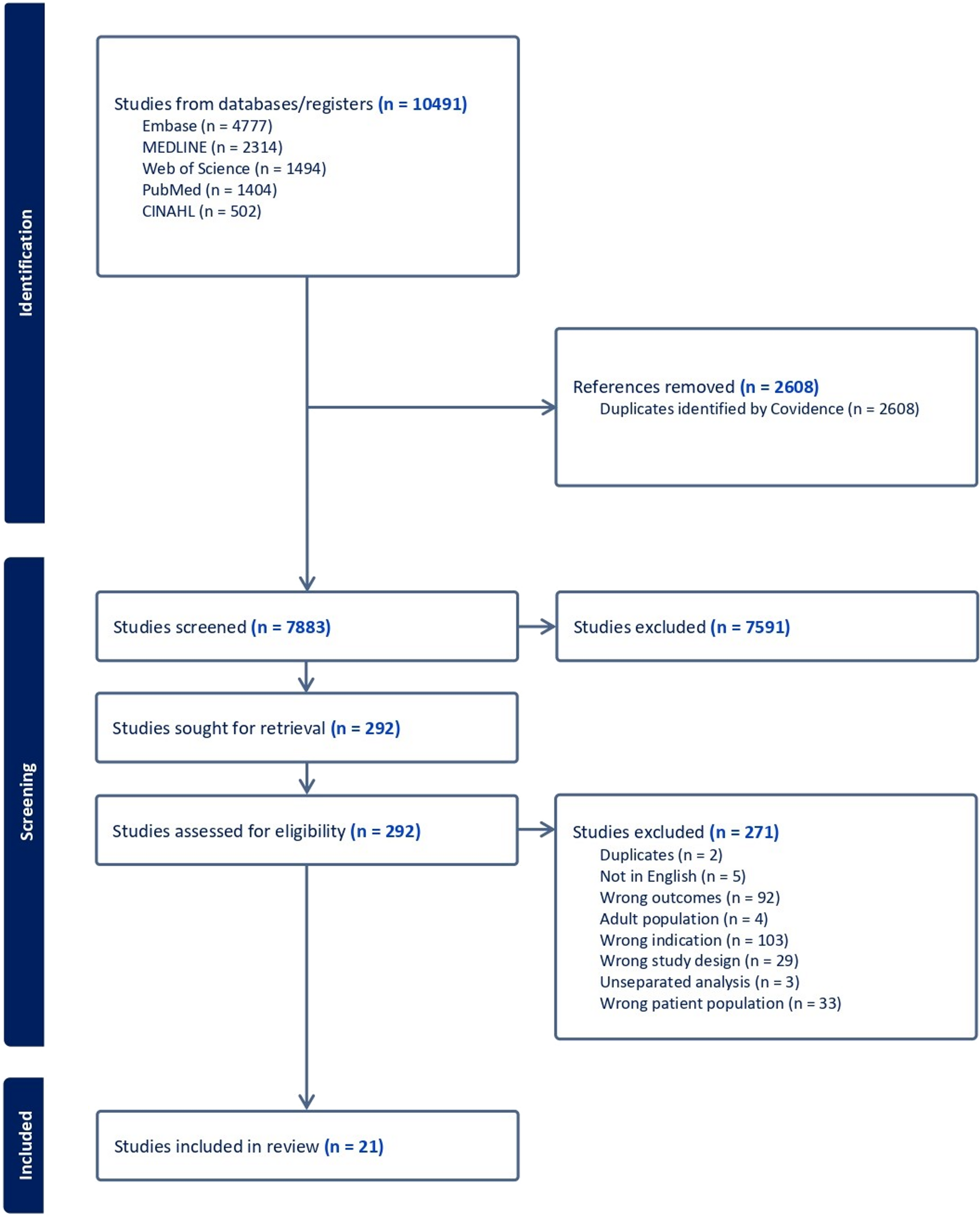
A total of 10,491 citations were retrieved from 5 the databases. Of these, 2,609 duplicates were removed while 7,591 citations were excluded based on the titles and their respective abstracts. Two hundred and ninety-two articles were screened for full-text review and 271 were excluded. Finally, 21 articles were selected to estimate the pooled prevalence of overweight and obesity among children and adolescents with T1D. The steps involved in the screening process are shown in detail in the PRISMA flow chart of study selection (Figure 1).
Fig. 1
PRISMA flowchart showing the study's selection process
Characteristics of included studiesTwenty-one (n = 21) studies were included in this systematic review and meta-analysis. These studies were published between 2008 and 2024 from a wide array of geographical regions: North America (USA, Canada) [24,25,26,27,28,29,30], South America (Brazil) [31, 32], Europe (Germany, Austria, Denmark, Iceland, Norway, Sweden, Netherlands, Poland) [15, 28, 33,34,35], Asia and Middle East (India, Malaysia, Iran, Israel) [36,37,38,39] and Australia [40]. North America led the geographical distribution of the studies, with Europe, Asia and the Middle East, South America, and Australia following in that order.
Seventeen (17) articles utilized a cross-sectional design [15, 24,25,26,27, 31, 32, 34,35,36,37,38,39,40] while 4 employed cohort (prospective and retrospective) study designs [15, 29, 33, 41]. The sample sizes ranged from 63 to 32,936 participants, and the total pooled sample size was 95,861 children and adolescents. The mean age of participants ranged from 9.7 to 16.4 years, with several studies reporting their medians and interquartile ranges. Duration of T1D also varied, with means from 3.9 to 8.1 years. The percentages of females across various samples were between 42.7% and 55%. Only a few studies (5) reported mean body mass index, with means ranging from 18.5 kg/m² to 21.2 kg/m². Table 1 presents the full details of the characteristics of the included studies.
Table 1 Characteristics of the Included StudiesQuality of included studiesThe quality scores for the included studies ranged from 4 to 8 out of 8 for cross-sectional studies and 5 to10 out of 11 for cohort studies. More than three-quarters of the studies, 76.2%, had a moderate to high quality with a score ≥ 6. The most common methodological deficiency in the reviewed studies pertained to the vague description of strategies to address confounding, which was found in many cohort studies. The outcome of the quality assessment is appended as a supplemental file [Appendix 2].
Prevalence of obesityOverall, the prevalence of obesity ranged from 2.5% [39] to 18.5% [33] in 19 cross-sectional and cohort studies. In random effects model, the pooled prevalence of obesity in children and adolescents with T1D was 8.8% [95% CI = 6.9–11.1], with statistically significant heterogeneity among studies (I² = 99.0%, p-value < 0.001), as shown in figure 2.
Fig. 2
Overall prevalence obesity
Prevalence of overweightApart from obesity, nineteen (19) studies also reported prevalence of overweight among children with T1D. The prevalence of overweight reported across different countries varied between 10.8% [39] and 49.5% [38]. In this meta-analysis, the estimated pooled prevalence of obesity among children with T1D was 22.0% [95% CI: 19.7–24.5]. However, there was a significantly high heterogeneity among the studies in the random effects model analysis (I² =98.1%, p < 0.001) (Figure 3).
Fig. 3
Overall prevalence of overweight
Prevalence of overweight and obesityTwenty-one (21) articles were included in the meta-analysis to estimate the overall prevalence of overweight and obesity which varied from 13.3% [39] and 63.6% [38]. For studies in which combined prevalence data were not reported but data for overweight and obesity were reported separately, the prevalence values were summed to obtain the overall prevalence of overweight and obesity. In random effects model, the pooled prevalence of overweight and obesity in children and adolescents with T1D was 30.0% [95% CI = 26.7–33.6]. There was a significant level of heterogeneity among studies (I2 = 99.0, P-value < 0.001) as illustrated in figure 4.
Fig. 4
Overall prevalence of both overweight & obesity
Subgroup analysisThe included studies were categorized into five continents including North America, South America, Europe, Asia and the Middle East, and Australia. Nineteen studies reported country-specific prevalence of overweight and obesity in diverse geographical regions. However, two studies [15, 42] were excluded in the analysis because it was conducted in two different continents. In this meta-analysis, the estimated pooled prevalence of obesity and overweight among children with T1D was highest in South America 38.8% [95% CI: 34.4–43.4], followed by North America at 32.2% [95% CI: 29.6–35.0] and Europe at 29.1% [95% CI: 15.8–47.3] while Asia and the Middle East reported the lowest pool at 20.3% [95% CI: 11.1–34.2]. In Australia, the estimated prevalence derived from one single study [40] was 33.1% [95% CI: 31.5 to 34.7], which was comparable to that of North America. The subgroup analyses reduced heterogeneity from the overall analysis by 99.0%. Importantly, substantial reductions in heterogeneity were observed in subgroups such as South America and North America, with I² values of 0.0% and 82.2%, respectively, although Europe and Asia and the Middle East continued to exhibit high heterogeneity at 99.8% and 90.5%, respectively.
Moreover, of all studies included in the current meta-analysis, 7 of them [24, 25, 27, 29, 34, 35, 42] reported gender-specific data on prevalence of overweight and obesity among children with T1D. The pooled prevalence from the random effects model analysis was slightly higher in females at 17.2% [95% CI: 14.9–16.1] than in males at 15.5% [95% CI: 15.1–19.6].
The prevalence of overweight and obesity was higher in cross-sectional studies at 32.1% [95% CI: 30.1–34.1] compared to cohort studies, which reported a prevalence of 26.8% [95% CI: 17.6–38.6]. Table 2 presents the full details of the subgroup analyses.
Table 2 Subgroup analysisPublication biasThe publication bias was checked by a funnel plot and objectively by the Begg’s and Egger’s test. There was a publication bias among the included studies in obesity, overweight, and both obesity and overweight, as depicted by asymmetrical distribution of funnel plot tests in Figures 5, 6, and 7 respectively. However, the Egger’s test of the funnel plot did not show any significant publication bias, with p-values of 0.689 for overweight, 0.364 for obesity, and 0.511 for combined obesity and overweight. Similarly, Begg’s test showed no significant bias for overweight, with p = 0.689, and obesity, with p = 0.552, while it showed statistical significance for combined obesity and overweight, with p = 0.046 (Appendices).
Fig. 5 Fig. 6
Fig. 6 Fig. 7
Fig. 7
Funnel Plot - Both obesity & overweight
Few studies (n = 6) reported factors associated with overweight and obesity in children with T1D, limiting the feasibility of a meta-analysis. Sociodemographic factors such as female gender [31, 32, 43], increasing age [24, 32], Hispanic/Latino race [24], lower household income [24], and lower parental education [43] were linked to higher overweight and obesity risk. Clinical factors included longer T1D duration [24, 25], higher HbA1c levels [24] and increased insulin doses [24, 32]. Behavioral factors such as reduced physical activity [24], lower self-monitoring of blood glucose [24], perceived stress [25], poor diabetes care activities [25], and poor quality of life [25] were significant. The results indicate the complex interaction of sociodemographic, clinical, and behavioral elements that present the risk of obesity and overweight among children with T1D. Table 3 presents the details of factors associated with overweight and obesity.
Table 3 Summary of the factors associated with overweight and obesity among Children with T1D
Comments (0)