
Remember me

CM9ER was a phase 3, open-label, randomized, controlled trial for which detailed methods have been previously reported [1]. In summary, adults with previously untreated aRCC with a clear cell component were randomized 1:1 to receive 1L CaboNivo or SUN. Eligibility was not limited by International Metastatic Renal Cell Carcinoma Database Consortium (IMDC) risk score, and patients were stratified at randomization by IMDC risk score (0 versus 1–2 versus 3–6), geographic region (USA and Europe versus rest of world), and tumor expression of the programmed cell death protein 1 (PD-1) ligand (PD-L1) (≥ 1% versus < 1%, or indeterminate). Although no crossover between study arms was allowed, patients were allowed to receive subsequent anticancer treatments.
The endpoints from the CM9ER trial utilized for the present post hoc analysis were OS and post-discontinuation survival after a mFU of 67.6 months. Post-discontinuation survival was defined as the time from the trial treatment discontinuation date to the date of death due to any cause. The TSE analysis included patients from the CM9ER ITT population who had discontinued treatment for any reason. Patients were excluded if their date of discontinuation was also registered as their date of death or if they had been censored for OS on that day.
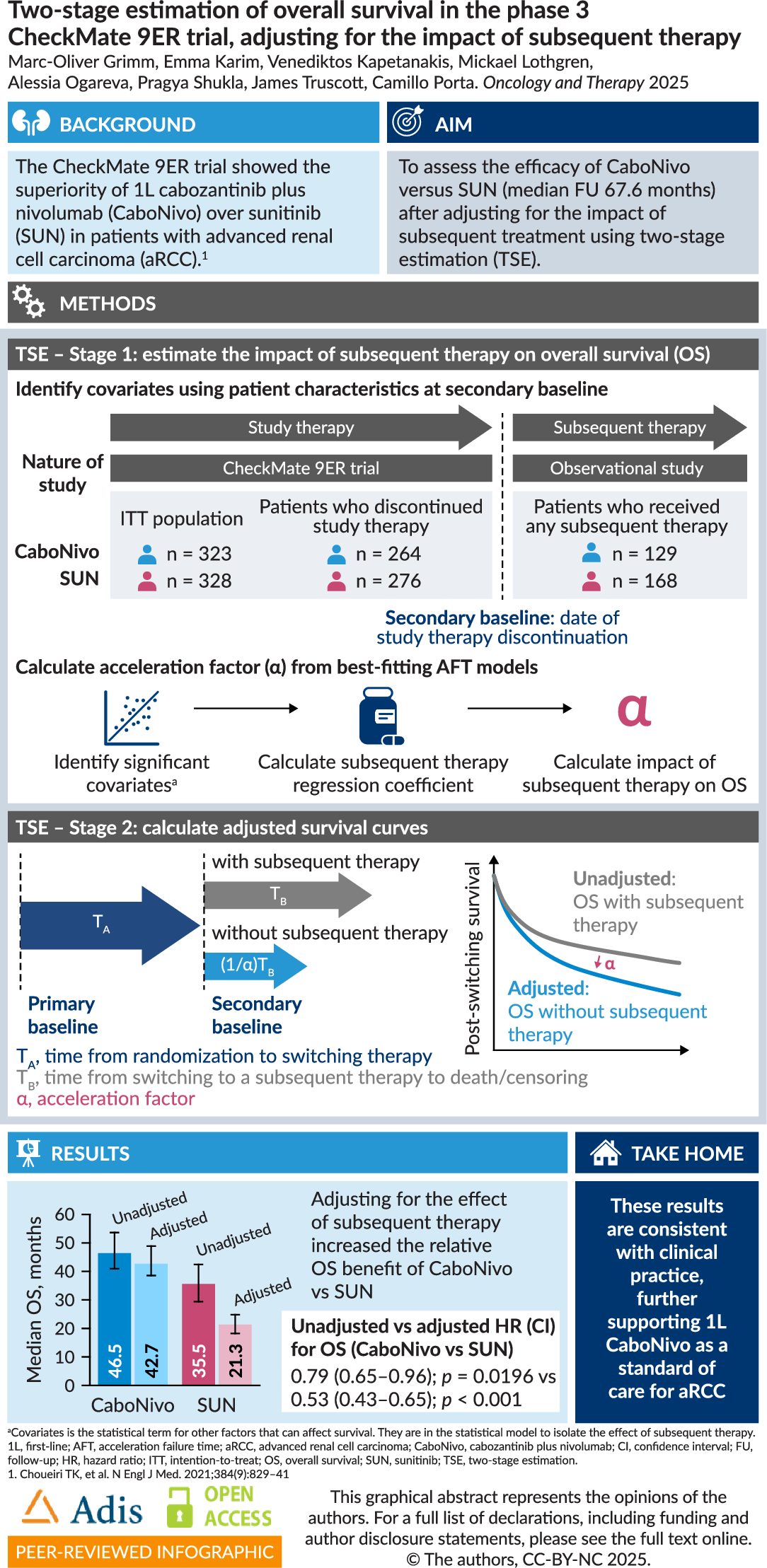
AnalysisTSE Stage 1TSE is a statistical method requiring patient-level data that can be used to estimate counterfactual (or “hypothetical”) OS for patients who switched to a subsequent therapy after treatment discontinuation, for the imagined scenario that they had not received subsequent therapy (Fig. 2). TSE requires a secondary baseline – a disease-related point in time after which all treatment switching occurs. There must also be no unmeasured confounding at the secondary baseline, and no confounding between the secondary baseline and the time of treatment switching [13]. For this analysis, the secondary baseline was the date of treatment discontinuation. The TSE method recognizes that, after patients discontinue study treatment, the trial becomes an observational study because the randomization no longer holds [13].
Fig. 2
Illustrative example of using an acceleration factor to estimate counterfactual survival times. Scenario assumes α > 1, i.e., switching to 2L TKI has a higher efficacy than not receiving 2L therapy. TA represents the time from randomization until switching to a subsequent therapy; TB represents the time from switching until death or censoring. α accleration factor; 2L second-line; CaboNivo cabozantinib plus nivolumab; OS overall survival; TKI tyrosine kinase inhibitor
Patient characteristics at the secondary baseline were used as covariates that could be independent predictors of initiating a subsequent treatment for the TSE analysis. Initial covariate selection was informed by previous TSE analyses of 1L combination checkpoint inhibitor plus tyrosine kinase inhibitor (CPI–TKI) regimens [12, 14]; they were also validated by clinicians for their potential impact on OS prognosis. The full list of covariates that were considered in the analysis are included in Table S1.
For the characteristics that had only been recorded at baseline (Karnofsky performance status [KPS] score, tumor PD-L1 expression, IMDC prognostic risk score, sarcomatoid features), clinical input was sought to assess the suitability of using baseline values for the secondary baseline. The approach was deemed appropriate on the basis that no other data were available but with the caveat that IMDC score would likely evolve over the time between baseline and the secondary baseline. Additionally, the sites of metastasis, number of metastatic organs/sites, sum of diameters of target lesions, and 5-dimension EuroQol questionnaire (EQ-5D) utility values had been recorded longitudinally but not at the secondary baseline. As such, values for these covariates were imputed using the measurement at the closest available time point to the secondary baseline. For the EQ-5D values, a cut-off window of 30 days before or after the secondary baseline was used to identify measurements suitable for imputation. No cut-off window was used for the metastasis variables on the assumption that they were less likely to change rapidly over time. Feedback from clinicians confirmed the validity of this approach for performing the imputations. No other imputation of missing data was required.
To assess the effects of subsequent therapy on survival, parametric accelerated failure time (AFT) models were fitted to post-discontinuation data after the secondary baseline. The models were developed to evaluate the impact of any subsequent therapy initiation on OS rather than that of specific subsequent therapies; evaluating the impact of individual subsequent therapies would have resulted in sample sizes insufficient to support statistically robust effect estimates. For each arm, six models (exponential, Weibull, log-logistic, log-normal, generalized gamma, and gamma) were compared to determine the best-fit model on the basis of goodness-of-fit criteria (Akaike and Bayesian information criteria). The models included a time-varying covariate that indicated whether or not subsequent therapy had been initiated.
Once the best-fitting models were identified, covariate selection processes were carried out, with each model always including the subsequent therapy covariate. The impact of each covariate on the model was first assessed individually to identify covariates that were significantly associated with post-discontinuation survival at the 0.1 threshold. Multivariate models were then generated for each arm including all significant covariates from the previous step. Backward selection was performed to remove covariates from the multivariate model that were no longer significant at the 0.1 level. Forward selection was then performed to reinclude covariates that had not been initially added to the multivariate model if they were now significant at the 0.1 level. Finally, any covariates that had lost significance during the previous step were removed from the model. The covariate selection processes were performed separately for each study arm, resulting in models containing covariates for subsequent therapy and any other significant predictors of survival.
TSE Stage 2The second stage of the TSE method uses an acceleration factor to calculate counterfactual OS. The factor represents the degree to which subsequent therapy increases (or decreases) post-treatment discontinuation survival time, and was calculated using the following equation:
where coeff is the regression coefficient for the subsequent therapy covariate in the best-fitting AFT model. Counterfactual survival times were then calculated for each patient. OS was separated into the time from randomization to treatment switching, which is unaffected by subsequent therapies received, and the post-switching survival, which is affected by subsequent therapy (Fig. 2). This resulted in the following equation for counterfactual survival time, where for each patient, \(i\):
where \(T\) is the OS time, \(_\) is the time from randomization until switching to a subsequent therapy, and \(_\) is the time from switching to a subsequent therapy until death or censoring.
Counterfactual survival curves for OS and HRs were calculated for the ITT population to compare OS between the CaboNivo and SUN arms. Stratified Cox proportional hazards models were used to estimate the HRs and 95% CIs. Robust bootstrap CIs were also estimated. This allowed comparison between the OS and HRs for the observed survival (with subsequent therapy) and the adjusted survival (without subsequent therapy).
In line with best practice for TSE analyses, survival curves and HR calculations were performed without re-censoring (the base case) and with re-censoring, as a sensitivity analysis to allow the effect of potential biases to be observed [12]. Analyses with and without re-censoring provide two boundaries for the uncertainty around informative censoring bias: re-censoring may underestimate long-term survival of patients who received subsequent therapy; analyses without re-censoring may overestimate their long-term survival. Details of the re-censoring methods have been included in the supplementary materials.
All analyses were performed in the R software (version 4.2.3 or above) [15].
EthicsThe results presented in this manuscript are based on data from the published CheckMate 9ER trial (international review board number 930112125). All procedures were conducted in accordance with Good Clinical Practice guidelines defined by the International Council for Harmonisation. Enrolled patients provided written informed consent according to the principles of the Declaration of Helsinki. Informed consent was obtained from all individual participants included in the original trial.
Comments (0)