
{kind=link}
{kind=link}
Remember me
Intracranial pressure (ICP) is defined as the pressure within the cranial vault, usually measured in millimeters of mercury (mmHg) (Schmidt et al 2018). Since the skull forms an enclosed space, ICP is the result of the pressure exerted by the cerebral tissue itself, as well as the surrounding fluid, including both blood and cerebral spinal fluid (CSF) (Czosnyka 2004). In a healthy adult, the normal ICP range is between 7 and 15 mmHg, with intracranial hypertension (IH) occurring at values above this (Munakomi and Das 2025). During normal physiologic conditions, cerebral autoregulation works to maintain a constant cerebral blood flow (CBF) through the constriction and dilation of cerebral blood vessels across different physiologic conditions, which has an indirect impact on maintaining constant values for ICP (Mount and Das 2025). For example, if there is an increase in blood pressure, cerebral autoregulation results in the vasoconstriction of the cerebral vessels to help maintain the CBF to the brain, indirectly helping to keep the current ICP (Mount and Das 2025). On the other hand, if there is a decrease in blood pressure, cerebral autoregulation would result in the vasodilation of the cerebral vessels to maintain the CBF and again have an indirect effect on the maintenance of ICP (Mount and Das 2025). In certain neurological conditions, such as during secondary neural injury from traumatic brain injury (TBI), the risk of complications such as hemorrhage or edema is much higher. ICP can increase drastically in both cases, resulting in IH (Armstead 2016). IH can cause significant stress on the brain and surrounding structures, potentially resulting in symptoms such as headaches, vision impairments, nausea, vomiting, seizures, and even coma (Sharma et al 2025). Similarly, untreated IH is a known contributor to ongoing secondary neural injury in various states of neurological disease, contributing to long-term morbidity and mortality.
ICP is typically monitored invasively through a device placed inside the parenchyma of the brain or in CSF pathways (Munakomi and Das 2025). There are two main categories of ICP monitoring devices: fluid-based devices and implantable devices (Munakomi and Das 2025). Fluid-based systems typically use a ventricular drain attached to an external pressure sensor (Evensen and Eide 2020). These devices are typically placed within the ventricular system, most commonly the lateral ventricle, in which the Foramen of Monro is utilized as a zero reference point for subsequent values of ICP to be compared to Munakomi and Das (2025). Fluid-based measures of ICP are typically considered the ‘gold standard’ not only because of their high accuracy when determining ICP but also because of their therapeutic benefits, such as the potential to drain CSF if necessary (Munakomi and Das 2025). However, fluid-based devices have significant limitations that prevent their widespread clinical use. These include the potential for misplacement, as the ventricular system can be difficult to locate in some cases, potential inaccuracies attributed to air bubbles and debris, and the risk of both hemorrhage and infection (Munakomi and Das 2025). Due to these limitations, implantable ICP monitoring devices are typically used. Implantable devices include epidural, subdural, and parenchymal devices (Munakomi and Das 2025). Epidural devices utilize a sensor placed between the skull and the dura mater, whereas subdural devices utilize a sensor placed in the subdural space (Evensen and Eide 2020, Munakomi and Das 2025). Both of these devices have been shown to have a low sensitivity, limiting their use in clinical settings (Evensen and Eide 2020, Munakomi and Das 2025). Parenchymal devices are placed within the brain tissue and have some benefits over fluid-based ICP monitoring devices (Evensen and Eide 2020, Munakomi and Das 2025). Firstly, since parenchymal devices are placed in the brain tissue itself, finding a particular location, such as a ventricle, is not necessary, making them easier to insert in cases of brain swelling (Munakomi and Das 2025). Secondly, the procedure of inserting a parenchymal device is less invasive when compared to fluid-based systems, resulting in a lower risk of severe complications (Evensen and Eide 2020). Lastly, the signals obtained from the parenchymal device are less prone to artifacts from either hemorrhage or debris (Evensen and Eide 2020, Munakomi and Das 2025). There is, however, a major limitation associated with parenchymal devices. These parenchymal devices are not able to be calibrated once they are placed into the brain tissue, resulting in issues with drift (Munakomi and Das 2025). The most common commercial ICP sensors used include the fibre-optic ICP sensor (Integra) and the strain-gauge ICP sensor (Codman) (Evensen and Eide 2020, Munakomi and Das 2025). These devices can be placed in either the parenchyma or the ventricular system and are designed to transmit pressure readings (Munakomi and Das 2025). While several of the methods listed above provide an accurate measurement of ICP, they are invasive, often require specialized expertise and surgical skills to install, are expensive to maintain, or have a low spatial resolution, as typically only one brain area is monitored (Maas et al 2022, Volovici et al 2022, Sainbhi et al 2023).
In 1977 Franz Jöbsis described using near-infrared spectroscopy (NIRS) as a tool for assessing cerebral physiologic variables (Jöbsis 1977). This technology operates by emitting a continuous wave of near-infrared (NIR) light, typically within the 650–950 nm range, which can penetrate the cerebral tissue by being able to permeate both the scalp and skull (Jöbsis 1977, Gomez et al 2022). Once inside the cerebral tissue, NIR light interacts with physiologic chromophores, such as oxygenated hemoglobin (OxHgB) and deoxygenated hemoglobin (deOxHgB), where it is either absorbed or scattered (Gomez et al 2022; Cope, no date). The portion of NIR light that is reflected back towards the NIRS system allows for the estimation of concentrations for both OxHgB and deOxHgB using the modified Beer-Lambert law (Gomez et al 2021, 2022). These hemoglobin concentrations can then be used to derive other measures, such as the total hemoglobin concentration (tHgB), which is calculated by taking the sum of both OxHgB and deOxHgB concentrations, and regional oxygen saturation (rSO2), which is calculated from the ratio of OxHgB to tHgB (Gomez et al 2021, 2022; Cope, no date). Some of the newer NIRS technology utilizes multiple channels which allows for more accurate cerebral signals such as total oxygen index (TOI) and total hemoglobin index (THI) (Zweifel et al 2010). TOI is determined through dividing the uncalibrated concentration of OxHgB by the the uncalibrated concentration of tHgB, while THI is calculated by summing the uncalibrated concentrations of OxHgB and deOxHgB (Zweifel et al 2010). This is achieved through the use of both short and long distance channels, that are able to help differentiate between cerebral and extra-cerebral signals, such as those coming from the scalp (Zweifel et al 2010). One example of a commercially available NIRS device is the Covidien INVOS 7100 (Covidien-Medtronic, Minneapolis, MN, USA) which utilizes two different channels, one at 730 nm, and another at 810 nm (Moerman et al 2013). By using two different light detectors, signal can be picked up from both superficial and cerebral tissue (Moerman et al 2013). One of these detectors is placed 3 cm from the emitter and is responsible for superficial tissue signals, whereas another detector that is placed 4 cm from the emitter receives signals from an approximate depth of 1.3 cm (Hogue et al 2021). A combination of signals from cerebral and extra-cerebral tissue allows for a higher accuracy when reporting values of cerebral variables. Due to the characteristics of NIR light allowing it to penetrate into cerebral tissue, NIRS has been proposed as a method to continuously monitor cerebral physiology in a cost-effective and non-invasive manner. Furthermore, NIRS technology is also relatively simple to use, and does not require the need for surgical skills, as seen with the invasive ICP sensors.
Preliminary data has suggested the utility of NIRS measures as surrogates for cerebral blood volume (CBV) (Sainbhi et al 2021, Gomez et al 2022). This raises the natural question as to the use of non-invasive continuous NIRS as a surrogate for invasive ICP measurements. As CBF and ICP are closely related to one another (Mount and Das 2025), any changes determined in CBF could be used to estimate further changes in ICP (Moraes and Silva 2021). When it comes to NIRS technology, hemoglobin concentrations can be estimated through the amount of NIR light that is absorbed or reflected (Gomez et al 2022; Cope, no date). These values not only have the potential to estimate CBF values, but indirectly ICP values as well. This is because there is an indirect relationship between CBF and ICP, as when the pressure inside the cranial vault increases, blood flow towards the brain is inhibited (Steiner and Andrews 2006). As ICP is invasively monitored in clinical settings to not only to maintain the current stability of patients but also prevent future secondary neurological injury, determining the relationship of ICP to NIRS signals can provide beneficial information regarding the non-invasive monitoring of patients. Both CBV and CBF are important indicators of cerebral hemodynamics in which fluctuations in these parameters not only impact the blood supply to the brain, but can also be associated with changes in ICP (Oswal and Toma 2023). CBV, CBF, and ICP are similar in the fact that all three of these variables in some way are related to changes in blood levels. Changes to the dynamics of the blood of the blood vessels can impact the amount of blood flowing towards the brain, which directly impacts values of both CBV and ICP (Kinoshita 2016). For example, in a state of hypercapnia, blood vessels will dilate to allow for more blood to get to the brain, in order to satisfy the increased need for oxygen (Kinoshita 2016). This will increase the CBV as there is now a larger volume of blood, but also the ICP as an increased amount of fluid in the cranial vault will increase the pressure within the cranium. When discussing ICP, blood levels are not the only factor impacting the variable, as a combination of both cerebral tissue and CSF also impact the pressure in the cranial vault (Czosnyka 2004). In order to fully grasp an understanding of how NIRS can be used to non-invasively monitor cerebral physiology, it is important to explore the existing literature on the potential relationships that exist between NIRS and the unique physiologic variables, such as CBV, CBF, and ICP.
There have been some recent advancements in displaying a potential statistical link between the NIRS variables and ICP (Zeiler et al 2017, Gomez et al 2023). In one paper, by Zeiler and colleagues, preliminary evidence describes a weakly positive correlation between many different NIRS-derived indices, including tissue oxygen reactivity (TOx) and total hemoglobin reactivity index (THx), and invasively obtained measurements of ICP; However, the majority of these relationships were not determined to be statistically significant (Zeiler et al 2017). In another paper, Gomez and colleagues determined that values for the NIRS based signal rSO2 and ICP were associated with one another during the experiment (Gomez et al 2023). Similarly, there are a handful of other small studies that have attempted to explore this relationship.
Although some preliminary evidence suggests a possible link between NIRS-derived metrics like rSO₂ and ICP, the temporal dynamics of this relationship remain poorly defined. The existing literature is limited, with findings that are often inconsistent and methodologically difficult to compare to one another. This scoping review (ScR) was therefore conducted to examine current human and animal research exploring the correlation between cerebral NIRS variables and invasively obtained ICP. By synthesizing the available literature, this work aims to clarify current understanding, identify knowledge gaps, and inform the development of future research into non-invasive ICP monitoring using NIRS technologies.
The methodology for this systematic review adheres to the methodological guidance outlined in the cochrane handbook for systematic reviews (Page et al 2021). Reporting of content in this review was structured according to the preferred reporting items for systematic reviews and meta-analyzes extension for ScRs (PRISMA-ScR) (Tricco et al 2018, Page et al 2021). Appendix A details a finalized PRISMA-ScR checklist. Both NS and FAZ collectively developed the search strategy for this review, with KYS providing support in the screening and selection of relevant articles.
2.1. Ethical considerationAll studies selected for this review were published in peer-reviewed journals prior to this analysis. As such, it is assumed that these articles have been through an appropriate screening process by these journals. As a result, it was not required to seek specific approval regarding ethics for this systematic ScR.
2.2. Eligibility criteria and search questionThis ScR set out to answer the central question: What is the relationship between NIRS-based cerebral signals and ICP? Studies were eligible for inclusion if they included a quantitative statistical comparison between the NIRS-based signals and ICP measurements. Any NIRS-derived signal, such as measures that are post-processing based and required additional signal sources for derivation (i.e. like ABP or others), were not included in this review of the literature. NIRS-based signals include measures that are directly obtained from the NIRS device, as well as measures that are returned live time from the parent NIRS device. The ICP data could be continuous or intermittent and obtained from humans or animals. Studies were excluded from our analysis if they were not published in English, were not full-length articles, or lacked an objective analysis between NIRS metrics and ICP.
2.3. Search strategyA comprehensive search was conducted across six databases: MEDLINE, EMBASE, SCOPUS, BIOSIS, Cochrane Library, and Globalhealth. The search of available records spanned from the time period of the inception of each database until 6, Jan 2025. Terms and synonyms for ‘brain’, ‘NIRS’, and ICP formulated detailed search strings that were inputted into each database (Appendix B). Results from each database were combined and screened for duplicate entries, resulting in a comprehensive set of possible studies.
2.4. Selecting studiesFollowing the removal of duplicate studies, the articles underwent a two-stage, two-reviewer approach, which was carried out by two independent reviewers (NS and KYS). During the first stage, titles and abstracts were assessed based on the predefined eligibility criteria. Studies that met these criteria proceeded to the second phase, where the full text of each article was independently assessed by each reviewer. In cases where the two reviewers disagreed on a study’s eligibility, a third party (FAZ) assisted in resolving the conflict. Additionally, the reference lists of all included studies were manually reviewed, to ensure that all the relevant articles were included in the analysis of this review paper.
2.5. Data collectionDetails from studies selected for this review are outlined in extraction tables formulated of different sections. One included section was patient/subject information, in which information regarding which patients/subjects were used and the respective sample size. The extraction tables also highlighted general study information in which details such as how ICP was recorded, the specific device and settings for the NIRS system, the specific NIRS signals investigated, and the specific experimental conditions of the study were all recorded in the extraction tables. Information regarding the results of the study, the association between NIRS signals and ICP, and the limitations of the selected studies were also obtained.
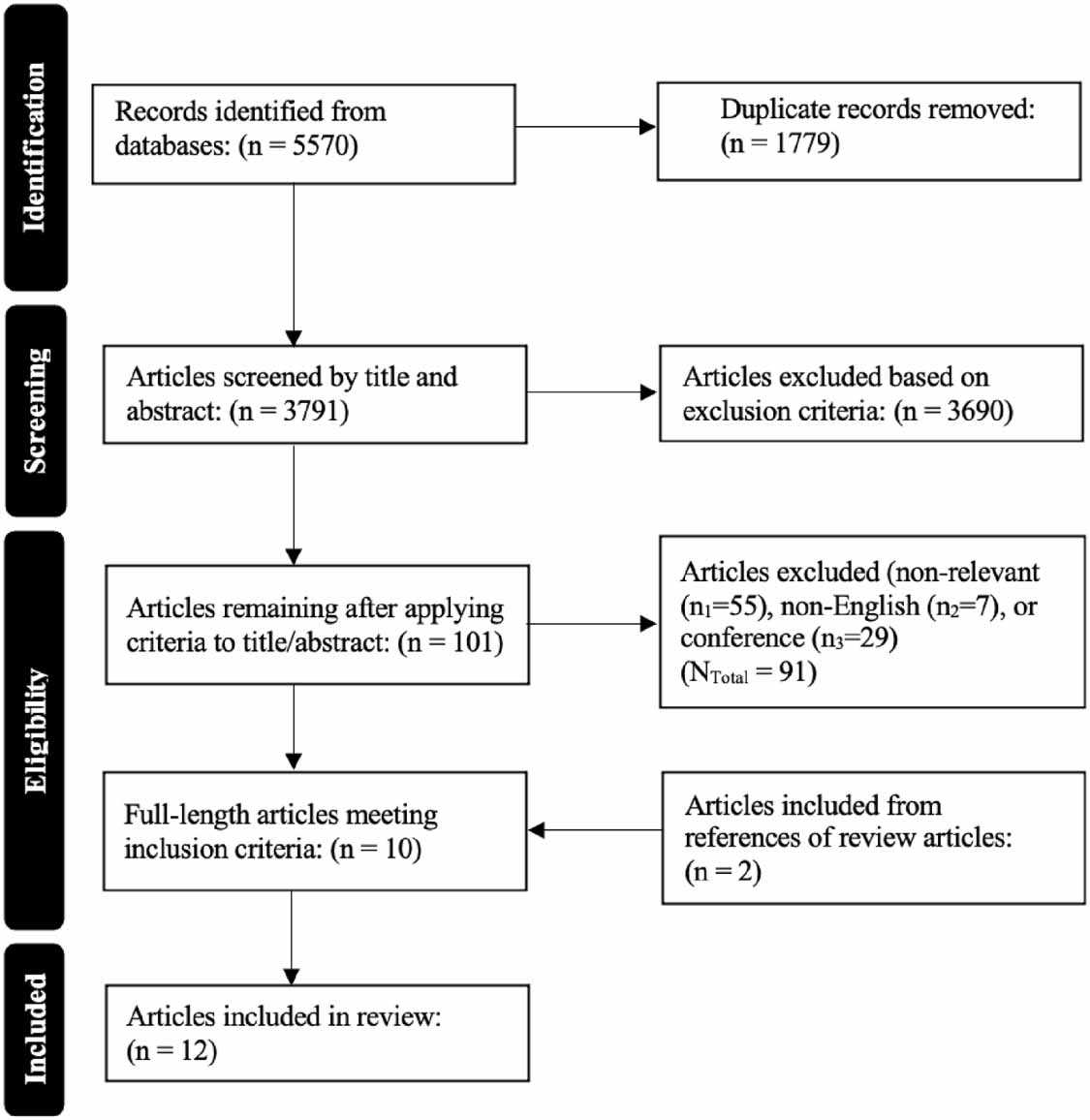
3.1. Search strategy and resultsThe study selection process is illustrated in figure 1, using a PRISMA flow chart. The initial search returned 5570 studies. After removing 1779 duplicate studies, 3791 unique articles remained to undergo screening of title and abstract using the predetermined eligibility requirements. This stage led to the exclusion of 3690 articles, as they did not meet the eligibility requirements. This left 101 articles for a full-text review. Upon assessing the full texts, 91 articles were excluded based on the same inclusion criteria, resulting in 10 studies being included from the initial search. The citation lists for these included studies were then examined, and with an additional two studies being included, a total of 12 studies were included in this systematic ScR.
Figure 1. PRISMA flowchart outlining the process of the systematic scoping review.
Download figure:
Standard image High-resolution image 3.2. Study demographicsOf the 12 articles included in the analysis of this review, five were animal-based studies, and seven were human-based. Of the animal-based studies, two were performed on non-human primates (NHPs) (Ruesch et al 2020, Relander et al 2022), one study utilized newborn piglets (Park et al 1999), one study was performed on adult male rats (Huang et al 2021), while the other study was performed on pigs (Putzer et al 2016). Out of the studies that were human-based, two were performed on adult patients (age 18 years and older) with a history of CSF circulatory disorder (Weerakkody et al 2010, 2012), three studies were performed on adult patients (age 16 years and older) who had been diagnosed with TBI (Zweifel et al 2010, Davie et al 2021, Gomez et al 2023), while two studies utilized pediatric patients (ages 1-16 years) (Wagner and Pfenninger 2002, Wang et al 2023). One of the studies utilizing pediatric patients focused on patients who have experienced acute global encephalopathy with coma (Wagner and Pfenninger 2002). All of the studies that utilized human subjects obtained informed consent from either the patients themselves (Zweifel et al 2010, Davie et al 2021, Gomez et al 2023) or written consent from parents when applicable (Wagner and Pfenninger 2002, Wang et al 2023). One of the studies that utilized pediatric patients also included a control group that was composed of 70 healthy children volunteers (aged 1–16 years) (Wang et al 2023). Individual sample sizes ranged from 6 to 115 individuals, with four of these articles having sample sizes under 10 individuals (Wagner and Pfenninger 2002, Putzer et al 2016, Ruesch et al 2020, Relander et al 2022). Table 1 summarizes details from the individual animal-based studies, while table 2 summarizes aspects for the individual human-based studies.
Table 1. Summary of animal-based studies investigating the relationship between NIRS signals and ICP.
ArticleStudy subjectsNumber of subjectsMeasure of ICP, MAP, and CPPNIRS Device, wavelength, and SDSNIRS signal examinedExperimental conditionsAssociation determinedStudy limitationsPark et al (1999)Newborn piglets54ICP was monitored through cisternal puncture by a 22-gauge spinal needle, and monitored by the Hewlett Packard neonatal monitoring system. Sampling frequency not mentioned.Hamamatsu NIRO 500 at four different wavelengths (776 nm, 828 nm, 848 nm and 913 nm). Sensors were applied to the parietal region, with an inter-optode distance of 4 cm. Sampling frequency was not mentioned.OxHgB, DeOxHgB, and, tHgB Animals were sedated through the inhalation of ether and then anesthetized through doses of sodium thiopental.Pancuronium was administered for paralysis.A tracheostomy was then performed for mechanical ventilation.Femoral arteries and veins were cannulated.ICP, MABP, and CPP were continuously monitored throughout the experiment.Bacterial inoculation of E. coli was done either i.v. or i.c.Animals were grouped according to the invasion results: i.v. (+) (positive CSF culture post-injection), i.v. (−) (negative CSF culture post-injection), i.c. (+) (positive blood cultures post-injection), and i.c. (−) (negative blood cultures post-injection).The control group received saline injections of equal volume to the experimental groups.Data analysis was performed using SAS software using t-tests, and ANOVA. It was determined that none of the invasively measured physiologic parameters showed any significant association with changes in NIRS parameters (p > 0.05).In the control group, it was found that during the 4 h, minimal changes in both NIRS parameters or ICP occurred.In the i.v. (+) group, tHgB, progressively increased, and DeOxHgB increased significantly. This contrasts with ICP, which did not show any significant changes over the 4-hour period.In the i.v. (−) group, tHgB, progressively increased, and DeOxHgB increased. This contrasts with ICP, which did not show any significant changes over the 4-hour period.In the i.c. (+) group, OxHgB decreased but was not determined to be significant. This contrasts with ICP, which increased progressively over the 4-hour period.In the i.c. (−) group, OxHgB decreased but was not determined to be significant. This contrasts with ICP, which increased progressively over the 4-hour period. No bias assessment was performed.Anesthesia and ventilation procedures could have impacts on physiological variables.Putzer et al (2016)Healthy 12–16 week old pigs.9ICP was monitored through a probe placed in the white matter of the left hemisphere through a burr hole. MAP was obtained through different catheters placed in the pulmonary and femoral arteries. CPP was then calculated by taking the difference between MAP and ICP.INVOS system on the right forehead. SDS was not mentioned. Sampling frequency was not mentioned.rSO2 Before being anesthetized, animals were fasted and premedicated with azaperone and atropine.Animals were then anesthetized with ketamine, propofol, and piritramide.The pigs were then placed in a supine position to be intubated.After placing all catheters and probes, pigs were left for a stabilization phase of 15 min.Pigs were cooled to a core temperature of 28 °C.Hypoxia was induced for 20 min by decreasing the amount of inspired oxygen.Hypercapnia was induced through the removal of the CO2 absorber.Ventricular fibrillation was induced through an alternating current, and mechanical ventilation was removed.Measurements were obtained at baseline and then after hypothermia, hypoxia, and hypercapnia. It was determined that relative changes in rSO2 and relative changes in CPP correlated with one another (r = 0.844, p < 0.001) before adrenaline was administered.After administering adrenaline, it was determined that relative changes in rSO2 and relative changes in CPP no longer correlated with one another. Small sample size.No bias Assessment was performed.Ruesch et al (2020)Healthy male rhesus macaques7ICP was monitored through the intraparenchymal probe. The sampling frequency was 100 Hz.OxiplexTS at two different wavelengths (690 and 830 nm). SDS was set to 0.75 cm, 1.33 cm, 1.66 cm, and 2 cm. Sensors were placed directly onto the skull, over the visual cortex. The sampling frequency was 5 Hz.OxHgB, DeOxHgB, and tHgB concentration. NHPs were initially sedated with ketamine, diazepam, and atropine.Isoflurane was used to anesthetize NHPs in the surgery room.An ICP sensor was placed into the brain’s frontal lobe, and a catheter was placed in the lateral ventricle.Pressure changes were induced by gravitational force, and the height of a saline bag was changed.A syringe pump was used to induce pressure changes.Experiments lasted from 10 to 15 h.After signal processing, the tfest function on MATLAB was used for data fitting.OxHgB was used alongside invasively obtained ICP in order to determine a transfer function that was subsequently applied to the hemoglobin data.This was used to obtain an estimation of ICP through the use of NIRS metrics.Oscillations in ICP were induced through rotating the reservoir, and were set to occur within the 0.009 Hz and 0.059 Hz range. The linear relationship between oscillation magnitudes in OxHgB and ICP was determined to be r2 = 0.86.When using the NIRS data to estimate values of ICP and comparing this to the invasively obtained ICP, it was determined that both amplitude and phase delay highly correlate (r2 = 0.86), while the transfer function is less correlated but still remains high (r2 = 0.57). Only male samples were used.Small sample size.Huang et al (2021)Adult male Sprague-Dawley rats.16ICP was monitored through a pressure-monitoring catheter. MAP was measured by cannulating the femoral artery. These two signal sources were then used to calculate CPP by taking the difference between MAP and ICP. The sampling frequency was not listed.A research device was designed and utilized two different wavelengths (735 nm and 850 nm). Sensors were placed over the striatum on the brain, and the penetrating depth of the light was about 8 mm. The sampling frequency was 25 Hz.OxHgB, DeOxHgB, and tHgB concentrations The rats were divided into four different groups: sham, 1.6 atm impact (mild TBI), 2.0 atm impact (moderate TBI), and 2.4 atm impact (severe TBI).A fluid percussion injury model was used to induce TBI. The rats were anesthetized, and a luer-lock connector containing a fluid-filled reservoir was secured.NIRS, ICP, and MAP monitoring devices were installed, and measurements were recorded for the next 2 h.MATLAB was used for subsequent statistical analysis. It was determined that the relation between ΔCPP and ΔOxHgB (r = 0.72) was statistically significant (p < 0.05).It was determined that the relation between ΔCPP and ΔtHgB (r = 0.6) was statistically significant (p < 0.05).It was determined that the relation between ΔCPP and ΔDeOxHgB (r = 0.36) was lower than the other NIRS variables and was not determined to be statistically significant (p > 0.05). Small sample size within each of the four groups.No bias assessment was performed.Short monitoring period (2 h).Relander et al (2022)Nonhuman Primates8ICP was measured using a parenchymal pressure sensor. The sampling frequency was 100 Hz.Freqeuncy-domain NIRS system (OxiplexTS) at both 690 and 830 nm. The optodes were placed directly onto the skull. The sampling frequency was 50 Hz.Changes in OxHgB, DeOxHgB, and tHgB concentrations. NHPs were sedated throughout the experiment.Changes in ICP were done using a lumbar catheter in the lateral ventricle of the brain.Each NHP had between 7 and 10 trials, each lasting around 90 mins. Each trial had a particular ICP level.Data from the devices was aligned using the voltage spikes measured during the experiment. A high correlation between actual ICP values and estimated values of ICP when looking at the NIRS metrics tHgB and OxHgB (r2= 0.946 and r2 = 0.937, respectively).A plot of the data showed a 95% CI of agreement between actual and estimated ICP values.MSE for ICP estimates using tHgB was 2.301 mmHg. MSE for ICP estimates using OxHgB was 2.703 mmHg.It was found that tHgB performed slightly better than OxHgB in estimating ICP. Data for one NHP was disregarded, as the instrument had some instabilities.Small sample size.ABP, arterial blood pressure; atm, standard atmosphere; cm, centimeters; CPP, cerebral perfusion pressure; CSF, cerebral spinal fluid; deOxHgB, deoxygenated hemoglobin; i.c. intracisternal; ICP, intracranial pressure; i.v., intravenous; MABP, mean arterial blood pressure; MAP, mean arterial pressure; MSE, mean squared error; NHP, non-human primate; NIRS, near infrared spectroscopy; nm, nanometers; OxHgB, oxygenated hemoglobin; rSO2, regional oxygen saturation; SDS, source-detector distance; TBI, traumatic brain injury; tHgB, total hemoglobin.
Table 2. Summary of human-based studies investigating the relationship between NIRS signals and ICP.
ArticleStudy subjectsNumber of subjectsMeasure of ICP, MAP, and CPPNIRS device, wavelength, and SDSNIRS signal examinedExperimental conditionsAssociation determinedStudy limitationsWagner and Pfenninger (2002)Pediatric patients experiencing acute global encephalopathy with coma6ICP was measured through either epidural or intraparenchymal monitoring. Sampling frequency was not given.Hamamatsu NIRO 500 at four different wavelengths (775, 825, 850, and 905 nm). Two fiberoptic bundles were placed over the frontotemporal region, directly onto the skin, with optodes being positioned 4–5 cm from each other.HgBDiff (OxHgB DeOxHgB) and tHgB concentrations were calculated at 2 Hz. Patients were eligible if they experienced acute global encephalopathy, had a GCS < 7, were ventilated, and had invasive ABP and ICP monitoring.MABP, ICP, HbDiff and tHgB were continuously monitored.Autoregulation is assessed through the injection of phenylephrine.Physiologic signals were recorded simultaneously on a hard disk and for online presentation.Pearson’s product-moment test was applied to HbDiff and ICP. Using visual inspection of the data, it was determined that the HgBDiff signal followed the changes in ICP. This was only present in the rise time series, as the synchronization was not seen during baseline or after MABP elevation.No synchronization was seen between the tHgB signal and ICP.The correlation between NIRS signals and ICP in the rise time series was (0.46 ± 0.05, p = 0.002). This was higher than both the third and fourth time series 0.21 ± 0.04, p = 0.002; 0.18 ± 0.07, p < 0.001; respectively).The correlation between HbDiff and ICP was r = 0.82 (p < 0.0001).The correlation between tHgB and ICP was r= 0.58 (p < 0.0006). Small sample size.Catecholamines were infused during half of the phenylephrine tests, but not the other half.2 out of 33 phenylephrine tests were excluded as the rise time was prolonged.Zweifel et al (2010)Human patients diagnosed with TBI40ICP was monitored with an intraparenchymal probe sampled at a frequency of 50 Hz.Hamamatsu NIRO 200 at three different wavelengths (775, 810, and 850 nm). Two detecting photodiodes were used and placed bilaterally over the frontal area. Sampling frequency was not mentioned.OxHgB, DeOxHgB, and THI. Patients were included if they were over the age of 16, had a diagnosis of TBI, underwent informed consent, and had ICP monitoring.Signals from ABP and ICP monitors were digitized using an A/D converter.Data acquisition and analysis were completed using ICM+ software.NIRS devices were removed once ICP monitoring was removed.10 s moving average filters were applied to ABP, ICP, and THI data.Pearson correlation was done to compare ICP and NIRS data. It was determined there was a good level of association between THI and ICP slow waves (0.65 ± 0.11). A bias assessment (Bland-Altman method) showed a small amount of bias within the results.Frontal contusions on some patients could impact NIRS recordings.Weerakkody et al (2010)Human patients with a history of CSF circulatory disorder19 (12 Males, 7 Females)ICP was obtained through an intraventricular catheter is connected to a pressure transducer and a saline-filled tube. The sampling frequency was 50 Hz.Hamamatsu NIRO 200 at four different wavelengths (775, 810, 850, and 910 nm). Optodes were at a distance of 4.5 cm from the laser diode complex. The sensors were placed on the forehead. The sampling frequency was 50 Hz.OxHgB, DeOxHgB, tHgB, and TOI. After informed consent from patients, NIRS signals, as well as ABP, were measured simultaneously.ICP, ABP and NIRS parameters were recorded throughout the experiment, including baseline, infusion plateau, post-infusion, and return to baseline.Signal artifacts were manually extracted.Non-parametric paired test and Spearman rank correlation analysis were used to analyze the data. Slow waves in OxHgB, DeOxHgB, tHgB, and THI were observed in coherence with slow waves of ICP.Coherence between ICP and NIRS variables in the slow-wave section was determined to be ⩾0.7.No significant phase shift was observed between NIRS and ICP variables, potentially indicating a direct link between the two.There was a positive correlation between the change of power in ICP and HgB slow waves. No bias assessment was performed.No healthy control group.Weerakkody et al (2012)Human patients with a history of CSF circulatory disorder19 (12 Male, 7 Female)ICP was obtained through an intraventricular catheter is connected to a pressure transducer and a saline-filled tube. The sampling frequency was 50 Hz.Hamamatsu NIRO 200 at four different wavelengths (775, 810, 850, and 910 nm). SDS was not mentioned. The sampling frequency was 50 Hz.OxHgB, deOxHgB, and tHgB concentrations. After informed consent from patients, NIRS signals, as well as ABP, were measured simultaneously.ICP and NIRS parameters were recorded throughout the experiment, including baseline, infusion plateau, post-infusion, and return to baseline.A parametric paired test was used to examine differences between NIRS variables and ICP. Slow waves of ICP were positively correlated with both OxHgB and deOxHgB.Over longer periods of time, there was a negative correlation between OxHgB and deOxHgB.When no slow waves are present, it was found that changes in OxHgB and deOxHgB were negatively correlated with each other; However, when slow waves are present, this becomes a positive correlation.This change in correlations could be used to determine ICP fluctuations. No bias assessment was performed.Davie et al (2021)Adult humans with TBI18 (15 Male, 3 Female)Collected from the bedside ICU monitor. Sampling frequency was not given.ForeSight monitor with sensors applied bilaterally to the frontotemporal arearSO2 sampled at 1 Hz. Patients were eligible in the study if they had a GCS ⩽ 8, were ventilated, had an arterial cannula, and were undergoing invasive ICP monitoring.rSO2 was monitored continuously for 72 h.MAP, ICP, and CPP data was collected every 5 min from the bedside monitor.Cerebral desaturation is defined as a decrease in rSO2 < 65%. Using Pearson correlation, it was found that in all patients, AUT for rSO2 <65% and area above the ICP threshold of 20 mm Hg were correlated (r = 0.72).A linear regression between AUT for rSO2 < 65% and area above the ICP threshold of 20 mm Hg in patients with a decreased rSO2 indicated that changes in rSO2 and ICP are moderately related to each other (r2 = 0.52, p < 0.01). Different extremes of TBI could have impacted cerebral hemodynamics differently.12 out of the 18 patients experienced a cerebral desaturation event, introducing potential discrepancies.Gomez et al (2023)Adult Human Patients diagnosed with TBI83 (66 Male, 17 Female)ICP was monitored with intraparenchymal strain gauge probes. The sampling frequency was 100 Hz.Covidien INVOS 5100 C monitor with sensors applied to the right and left forehead to record the right and left frontal lobes.rSO2 sampled at 1 Hz. Included patients were diagnosed with TBI, had invasive ICP and ABP monitoring, and had concurrent NIRS monitoring.Data acquisition and analysis were completed using ICM+ software.Artifacts were manually removed from high-resolution data.10-second non-overlapping, moving average filters were applied to ABP, ICP, and rSO2 data.PRx was derived as a Pearson correlation between ICP and ABP on a minute-by-minute basis.COx was derived as a Pearson correlation between rSO2 and CPP on a minute-by-minute basis.COx_a is derived as a Pearson correlation between rSO2 and ABP on a minute-by-minute basis.Data analysis was performed using R. Using agglomerative hierarchical clustering, ICP and rSO2 measures were more closely related than the other physiological parameters.Using a principal component analysis, it was determined that ICP and rSO2 measures are associated in multidimensional physical space. This was because co-variance patterns of PRx, PAx, and RAC were closely related to patterns in COx and COx_a. Possible interference with NIRS signals could have occurred depending on injury type; however, these were noted and recorded during the data collection.The majority of signals came from the right NIRS sensor, with the left sensor being used in only a few patients.Wang et al (2023)The injury group consisted of pediatric patients115 (59 Males, 56 Females) (45 in the injury group and 70 in the control group)ICP was measured using intraventricular monitoring. Sampling frequency not given.MNIR-P200 at two different wavelengths (730 and 850 nm). The two receivers were placed 3 and 4 cm from the NIR light source. The sensors were placed on the forehead. The working sampling frequency was from 10 kHz to 100 kHz.rSO2 The control group consisted of 70 healthy children (aged 1-16), while the injury group included pediatric patients who underwent craniocerebral surgery (aged 1-16). All participants required intact skulls and no skin defects.rSO2 was obtained 6, 12, 24, 48, and 72 h after surgery. It was also continuously recorded from 15 min until 6 h after dehydrating drug admission.CT scans were used to categorize the amount of edema. Edema was then categorized as non, focal, or multifocal edema.Data processing was done using SPSS and R software.T-tests were used to make comparisons between two groups, whereas comparisons between multiple groups were done using ANOVA.Linear correlation was performed to determine the correlation between variables. It was determined that rSO2 was significantly lower in the injury group compared to the control group.There was a positive correlation between rSO2 and CPP in all ages (r = 0.48, p < 0.001).Over the recording period, ICP increased significantly (p < 0.001) in all age groups except for the 1-3-year-old group, where increases in ICP were not found to be statistically significant (p = 0.056).Over the recording period, rSO2 decreased significantly for all age groups (p < 0.001). No bias assessment was performed.ABP, arterial blood pressure; AUT, area under threshold; COx_a, ABP based cerebral oxygenation index; COx, cerebral oxygenation index; CPP, cerebral perfusion pressure; deOxHgB, deoxygenated hemoglobin; GCS, glasgow coma scale; HgB, hemoglobin; HgBDiff, cerebral hemoglobin saturation; ICP, intracranial pressure; ICU, intensive care unit; MABP, mean arterial blood pressure; MAP, mean arterial pressure; NIRS, near infrared spectroscopy; OxHgB, oxygenated hemoglobin; PRx, pressure reactivity index; rSO2, regional oxygen saturation; SDS, source-detector distance; TBI, traumatic brain injury; TCD, transcranial doppler; tHgB, total hemoglobin; THI, total hemoglobin index; TOI, tissue oxygenation index.
3.3. Animal based studies3.3.1. NIRS conditions and variablesFour among the five animal-based articles analyzed in this review used commercially available NIRS devices to record the measurements: the Hamamatsu NIRO-500 (Park et al 1999), an INVOS system (Putzer et al 2016), and the OxiplexTS system (Ruesch et al 2020, Relander et al 2022). The other included study utilized a research device designed for the particular experiment (Huang et al 2021). The cerebral NIRS signal that was most utilized in these animal-based studies included concentrations of both OxHgB and deOxHgB, which were subsequently summed together to determine the total hemoglobin (tHgB) concentration (Park et al 1999, Ruesch et al 2020, Huang et al 2021, Relander et al 2022). Out of the five animal-based studies included, only one study did not directly utilize either OxHgB or deOxHgB values and instead used regional oxygen saturation (rSO2) as the cerebral NIRS signal (Putzer et al 2016).
Despite many of the same cerebral NIRS signal sources being utilized among the included animal-based studies, the context in which these signals were obtained differed between the studies, varying from healthy controls to different experimental groups. In a study performed by Park and colleagues, both intravenous (i.v.) and intracisternal (i.c.) inoculation of piglets with Escherichia coli was used to create five different groups (Park et al 1999). These groups included a control group that received injections of saline equal to the volume of the E.coli injections and an i.v. (+) group which had a positive CSF culture post venous injection, an i.v. (−) group which had a negative CSF culture post venous injection, an i.c. (+) group which had positive blood cultures post cisternal injection and an i.c. (−) group which had negative blood cultures post cisternal injection (Park et al 1999). In another study, Putzer and colleagues created different experimental groups by inducing states of hypoxia and hypercapnia (Putzer et al 2016). Lastly, Huang and colleagues performed a study in which measurements were made on rats divided into four groups of TBI severity (Huang et al 2021). These groups included a sham group, rats with mild TBI, rats with moderate TBI, and rats with severe TBI (Huang et al 2021).
3.3.2. ICP techniques and measurementOver the five animal-based studies included in this review, the methodology for obtaining measurements for ICP varied. In one of the included studies, ICP was monitored through a cisternal puncture, where the Hewlett-Pack
Comments (0)