
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Remember me
Heart failure (HF) is a chronic and progressive cardiovascular condition that affects more than 64 million people globally (Savarese et al 2023), including approximately 100 000 new diagnoses each year in Canada (Saveski et al 2025) and 960 000 in the United States (Hauptman 2017). It remains one of the leading causes of hospital readmissions among adults over the age of 65 and carries a five-year mortality rate of approximately 50% following diagnosis (Bytyçi and Bajraktari 2014, Cotter et al 2023). HF is characterized by the heart’s reduced capacity to pump blood effectively, which limits the delivery of oxygen and nutrients to peripheral tissues. This impaired circulation results in symptoms such as dyspnea, fatigue, and reduced exercise tolerance. Together, these symptoms negatively affect patients’ daily functioning and quality of life (Heo et al 2008, Pavlovic et al 2021). Without appropriate management, HF frequently leads to repeated hospitalizations and creates substantial emotional, logistical, and financial burdens for patients and caregivers alike (Pavlovic et al 2021). As a result, there is a growing emphasis on improving outpatient monitoring strategies, particularly those that can be used at home or in community settings.
Peripheral edema, often presented as swelling in the lower limbs, is a key clinical sign of congestive HF (CHF) and serves as an indicator of fluid volume overload (King and Goldstein 2025). However, it is not unique to HF. Similar fluid accumulation may occur in patients with chronic kidney disease, liver dysfunction, or venous insufficiency, and certain other conditions (Goyal et al 2025). While edema is rarely dangerous on its own, persistent swelling can lead to discomfort, impaired mobility, skin damage, and social withdrawal, particularly in older individuals (Greene and Meskell 2016). More importantly, worsening edema can indicate declining cardiovascular function and often precedes acute decompensation, which increases the likelihood of emergency interventions and hospital readmissions (King and Goldstein 2025). These risks highlight the importance of timely and reliable edema monitoring to support early detection and treatment.
Traditional methods for assessing limb edema include daily weight tracking, manual limb circumference measurements, water displacement tests, and physical examinations such as the pitting edema scale (Nishimura et al 2020, Fudim et al 2023). Among these, weight tracking is the most used method in clinical practice; however, it is limited by its intermittent nature, dependence on patient compliance, and inability to accurately quantify fluid accumulation, which is critical for the early detection of clinical deterioration (Abraham et al 2011, Fallahzadeh et al 2017, Zhang et al 2018, Physiopedia contributors 2025). In many outpatient or post-discharge scenarios, they may fail to detect subtle changes in fluid accumulation. These limitations have led to increased interest in objective, non-invasive, and continuous monitoring techniques that can be used in everyday environments.
Recent advances in medical device research have enabled the development of portable and wearable technologies aimed at improving edema detection. Among these, two approaches stand out: wearable ultrasound systems and bioelectrical impedance analysis, also referred to as bioimpedance (BI).
Wearable ultrasound provides real-time imaging of subcutaneous fluid and soft tissue, offering detailed anatomical information (Niimi et al 2014, O’Rourke et al 2015, Fudim et al 2023). However, the technology is expensive and remains limited in wearable form due to its size and the need for expert interpretation of the resulting images. These factors restrict its practicality for long-term or ambulatory use (Gathright et al 2024, Hu et al 2024).
In comparison, BI offers a promising alternative for fluid monitoring. It measures the impedance of biological tissue by applying a small alternating electrical current and analyzing voltage responses. Because different current frequencies can probe extracellular and intracellular compartments, and different tissue types result in different impedances, BI provides insight into fluid and volume distribution across tissues (Carlson-Newberry et al 1997). This technique is highly sensitive to small changes in hydration and is compatible with compact, low-power devices. These features make BI especially suitable for use in wearable formats, such as socks, ankle bands, or textile-based electrodes (Roh et al 2023, Sánchez et al 2024). For instance, Sánchez et al demonstrated the stability and usability of textile BI systems in daily monitoring contexts (2024). Despite these advances, many BI systems are still in early development stages, and further research is needed to validate their use in clinical and home settings.
We note that pulmonary edema is also a critical medical condition, where fluid accumulates in the lungs, leading to shortness of breath, wheezing, and difficulty breathing. Often caused by CHF, sudden onset of pulmonary edema requires immediate medical attention. Many works have studied impedance measurements or impedance-based imaging of the torso to assess pulmonary edema to guide treatment and/or monitoring of pulmonary edema, particularly during recovery (Ciu et al 2024). However, peripheral edema presents a different challenge for patients and clinicians. With a prevalence of almost 20% of adults in the US (Besharat et al 2021), peripheral edema is strongly associated with low activity and low mobility levels and pain. It is also a frequent complaint in out-patients, as well as a frequent cause of re-hospitalization. Further, the presence of peripheral edema is correlated with poorer outcomes in hospitalized patients—for example, admission with peripheral edema was associated with a 26% higher risk of hospital mortality, compared to patients without edema (Danziger et al 2016). Regular monitoring of peripheral edema can play a key role in disease management (Heidenreich et al 2022, Patel et al 2022). Therefore, this review focuses on BI for peripheral edema measurement and/or monitoring, to support identification of changing health status (and delivery of intervention) as rapidly as possible.
Specifically, the objective of this review is to assess the current state of portable and wearable BI technologies used to monitor peripheral edema in the lower limbs, with a particular focus on applications in HF. Studies involving other clinical conditions were also considered if the monitoring methods could be adapted for HF care. While several reviews have explored the broader medical uses of BI, none have specifically addressed its role in tracking lower-limb edema using wearable or non-invasive systems. Much of the current literature has focused on pulmonary edema, leaving fewer studies that address swelling in the ankle, calf, or thigh. This is a notable gap, especially given the clinical relevance of peripheral edema in chronic conditions such as HF, lymphedema, and venous disease.
By synthesizing the available evidence, this review aims to support future research, guide clinical integration, and inform the design of wearable monitoring technologies that can improve outcomes for individuals at risk of fluid overload.
2.1. Search strategyThis review aimed to identify primary research articles focused on the use of BI for the assessment or monitoring of peripheral leg edema. Studies were included if they: (1) were original research from peer-reviewed journals, (2) involved human participants, (3) assessed peripheral leg edema, and (4) utilized BI-based technology for measurement or monitoring. Studies were excluded if they focused on non-leg anatomical sites, employed implantable devices, involved animal or simulation models, or were not original research. This review was conducted in accordance with the PRISMA 2020 reporting guidelines (Page et al 2021a, 2021b).
A systematic search was conducted across PubMed, IEEE Xplore, and Web of Science databases on 17 June 2025. The search was limited to studies published between 2005 and 2025, and only English-language journal articles were considered. To capture earlier literature, an additional search covering the period from 1995 to 2004 was conducted on 25 September 2025.
Search queries were structured using the following four concept clusters:
1.
‘edema’ OR ‘fluid’ OR ‘water’AND
2.
‘monitoring’ OR ‘measurement’ OR ‘tracking’ OR ‘volume’ OR ‘size’ OR ‘continuous’ OR ‘track’ OR ‘monitor’ OR ‘estimating’ OR ‘sensing’ OR ‘estimation’AND
3.
‘portable’ OR ‘wearable’ OR ‘remote’AND
4.
‘bioimpedance’ OR ‘impedance’ OR ‘electrical impedance’
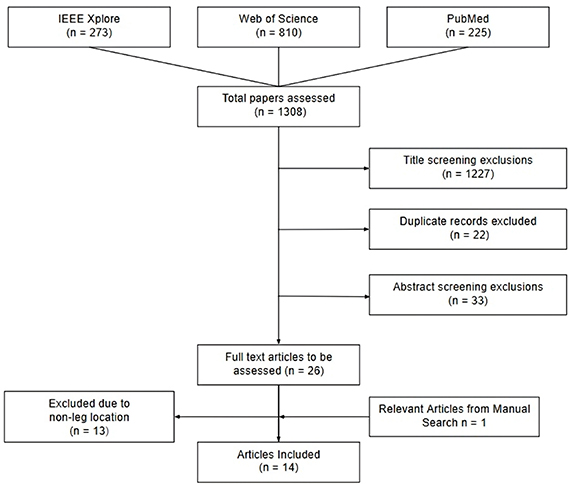
Search results from each database were exported into Microsoft Excel for screening and data handling. Screening was conducted in four stages: (1) title screening, (2) duplicate removal, (3) abstract screening, and (4) full-text review. The full article selection process is illustrated in figure 1.
Figure 1. Workflow of the article screening and selection steps.
Download figure:
Standard image High-resolution image 2.2. Article selectionScreening and data extraction were independently performed by the authors. A total of 273 articles were retrieved from IEEE Xplore, 810 from Web of Science, and 225 from PubMed. Following title screening, 1227 articles were excluded for lack of relevance to the topic (260 from IEEE Xplore, 778 from Web of Science, and 189 from PubMed). An additional 22 duplicate entries were removed, resulting in 59 unique articles for abstract review.
During abstract screening, 33 articles were excluded for the following reasons:
Not original research (n = 6; review articles)Not published in a peer-reviewed journal (n = 1; conference paper)Not specific to leg edema (n = 18; thoracic [n = 8], total body water [n = 7], abdominal [n = 1], wrist [n = 1], forearm [n = 1])Involving implantable devices (n = 2)Based on non-human models (n = 3; including phantom, stimulation, and plant-based studies).A total of 26 articles progressed to full-text screening, of which 13 were excluded for lacking a focus on edema in the lower extremities. One article from the citations was manually included.
In total, 14 articles were selected for inclusion. Of these, five focused on patients with HF, while the remaining eight involved non-HF populations. The studies were conducted across North America and Europe, published between 2008 and 2024. The populations studied included healthy individuals as well as patients with CHF, knee or ankle injuries, and those undergoing hemodialysis (HD). We note that the search from 1995–2005 returned no relevant articles. Although foundational research towards BI-based edema measurement was ongoing during that period, studies targeting limb edema monitoring in an at-home, wearable context, were only initiated in later years.
2.3. Screening and quality assessmentScreening and data extraction were performed independently by one researcher, with subsequent review and verification by another. Discrepancies were resolved by consensus. If relevant study details were unavailable or unclear in the full text, the data item was marked as missing and no assumptions were made.
2.4. Summary of studiesFor each included study, the following data were extracted: first author, year of publication, measurement method, number of electrodes used, frequency range, subject population, and the parameter assessed. Summaries of the included studies are presented in table 1 for studies focused on HF, and table 2 for studies focused on other clinical applications.
Table 1. Summary of studies including heart failure patients (n = 5).
AuthorsYearNumber of electrodesFrequency rangeParticipantsEnvisioned applicationGutiérrez-Carretero et al (2024)2024450 kHz76 subjects with HFPredict HF risk & monitor decompensationSánchez et al (2024)202443–1000 kHz5 healthy participants 2 participants with HFWearable edema monitoring in HFScaliusi et al (2023b)202341–200 kHz1 healthy participant 1 participant with HFReal-time fluid tracking in HFScaliusi et al (2023a)202341–200 kHz4 healthy participants 2 participants with HFWearable volume tracking for early HF detectionDelano and Sodini (2018)201844–1000 kHz17 participants undergoing hemodialysis (9/17 with CHF)Calf BI to prevent fluid overload in CHFTable 2. Summary of studies including patients without heart failure (n = 9).
AuthorsYearNumber of electrodesFrequency usedParticipantsEnvisioned applicationDelano et al (2022)202241–500 kHz5 healthy participantsEvaluates textile BIS for fluid trackingCritcher and Freeborn (2021)202141–128 kHz3 healthy participantsImproving PCB durability in wearablesMabrouk et al (2021)202145–100 kHz8 participants with healthy ankles 7 participants with injured anklesDetects edema & injury during walkingMabrouk et al (2020)202045–100 kHz8 healthy participants 5 participants with recent acute ankle injuryTracks ankle edema recovery with wearable BISHersek et al (2017)2017450 kHz42 healthy participants 7 participants with recent acute, unilateral knee injuryWearable knee edema and recovery monitoringVilla et al (2016)201661 kHz, 796 kHz1 healthy participantTracks fluid shifts during real-world activityMontalibet et al (2016)201643.084–1000 kHz4 healthy participants 4 participants on HDMitigating posture effects in dialysis monitoringHersek et al (2016)2016450 kHz7 healthy participants 2 participants with recent unilateral knee injuryHigh-res knee edema & flow monitoringZhu et al (2008)200845 kHz20 maintenance HD patientsUsing calf BIS to assess hydration3.1. BI and tissue fluid estimationBody fluids, mainly water with dissolved ions such as potassium (K+), sodium (Na+), and chloride (Cl−), are distributed across two main compartments: intracellular and extracellular spaces. These compartments are separated by cell membranes, which act like capacitors, storing charge and affecting how electrical current flows depending on the frequency applied. In living tissue, water serves as the primary conductor, and the ions within these fluids provide the pathway for electrical current.
BI refers to the impedance biological tissues offer to an alternating electrical current. BI measurement technologies offer a non-invasive technique used to assess physiological characteristics such as fluid status, body composition, and tissue health. In the context of this review, BI is applied to evaluate tissue hydration, focusing on detecting and monitoring peripheral edema. The method involves placing surface electrodes—like those used in Electrocardiograms—on the skin to introduce a small alternating current, then measuring the resulting voltage to calculate the tissue’s impedance.
At low frequencies, the current primarily passes through extracellular fluid (ECF), allowing estimation of extracellular resistance (Re). At higher frequencies, the current can penetrate cell membranes and access intracellular fluid (ICF), enabling calculation of total tissue resistance RT (wherein, the equivalent total resistance is Re in parallel with Ri, such that RT = ReRi/(Re + Ri)) (Scagliusi et al 2023b), where Ri is the intracellular resistance. The capacitive properties of the cell membrane also introduce a reactance (Xc) into the complex tissue impedance, which changes with frequency. Since edematous tissues contain more water, they conduct current more easily and therefore exhibit lower overall impedance compared to normally hydrated tissue. The Cole equation (Heidenreich et al 2022) is widely used to describe this frequency-dependent behavior of impedance, offering an approach for assessing tissue hydration through multi-frequency measurements:

where Z is the complex impedance value,  is the resistance at infinite frequencies (equivalent to Re in parallel with Ri), R0 is the resistance at the DC frequencies (equivalent to Re),
is the resistance at infinite frequencies (equivalent to Re in parallel with Ri), R0 is the resistance at the DC frequencies (equivalent to Re),  is the angular frequency,
is the angular frequency,  is the time constant of the frequency response, and
is the time constant of the frequency response, and  is a constant phase term (value between 0 and 1) that modifies the width of the dispersion to match empirical values. While the Cole equation is used widely to model the complex, frequency-dependent impedance of individual (homogeneous) tissues, we note that each tissue or body fluid within a region (e.g. fat, muscle, blood, etc) would have distinct impedance characteristics and thus the Cole equation’s parameter values will vary depending on the tissue. Furthermore, within a specific region in the body, several tissue types may be mixed in a complex arrangement—while each tissue can be modeled based on their individual impedance properties, the Cole equation does not readily enable modeling the impedance distribution or complexity of such a scenario.
is a constant phase term (value between 0 and 1) that modifies the width of the dispersion to match empirical values. While the Cole equation is used widely to model the complex, frequency-dependent impedance of individual (homogeneous) tissues, we note that each tissue or body fluid within a region (e.g. fat, muscle, blood, etc) would have distinct impedance characteristics and thus the Cole equation’s parameter values will vary depending on the tissue. Furthermore, within a specific region in the body, several tissue types may be mixed in a complex arrangement—while each tissue can be modeled based on their individual impedance properties, the Cole equation does not readily enable modeling the impedance distribution or complexity of such a scenario.
The fields of BI for body composition and fluid monitoring are well established, with extensive studies demonstrating validated measurements in both healthy subjects and patients. Several review studies of earlier works in the field are available (Chumlea and Baumgartner 1990, Kyle et al 2004a, 2004b, Jaffrin and Morel 2008, Khalil et al 2016), for example, (Kyle et al 2004a) examines body impedance analysis equations across a wide range of studies, and (Jaffrin and Morel 2008) provides a review and comparison of methods for using non-invasive BI measurements in estimating extracellular, intracellular, and total body water. Importantly, early works highlighted challenges such as inconsistent protocols, lack of standardization, and difficulties distinguishing between fluid compartments, which limited the accuracy and reliability of these measurements in clinical settings. These foundational issues remain important considerations as modern wearable BI technologies continue to evolve.
3.2. Wearable BI in HF and broader applicationsThis section summarizes the current research on wearable BI technologies for fluid status monitoring, as identified through the process described in section 2. It includes studies focused on HF populations as well as broader applications like peripheral edema detection, joint injury assessment, vascular dynamics, and dialysis-related fluid management. The studies are detailed in tables 1 and 2 and collectively demonstrate how BI is evolving as a continuous, non-invasive tool to track physiological changes, tackle clinical challenges related to fluid overload and tissue health, and advance wearable systems for real-world healthcare.
3.2.1. Overview of HF-related BI studiesAmong the included studies, five specifically focused on peripheral edema in HF patients, exploring BI’s potential to assess fluid status, monitor disease progression, and improve care after hospital discharge. This research is crucial because managing congestion remains a key challenge in HF, and continuous, non-invasive monitoring could improve both clinical decisions and patient self-management. Key features of these studies are discussed in this section.
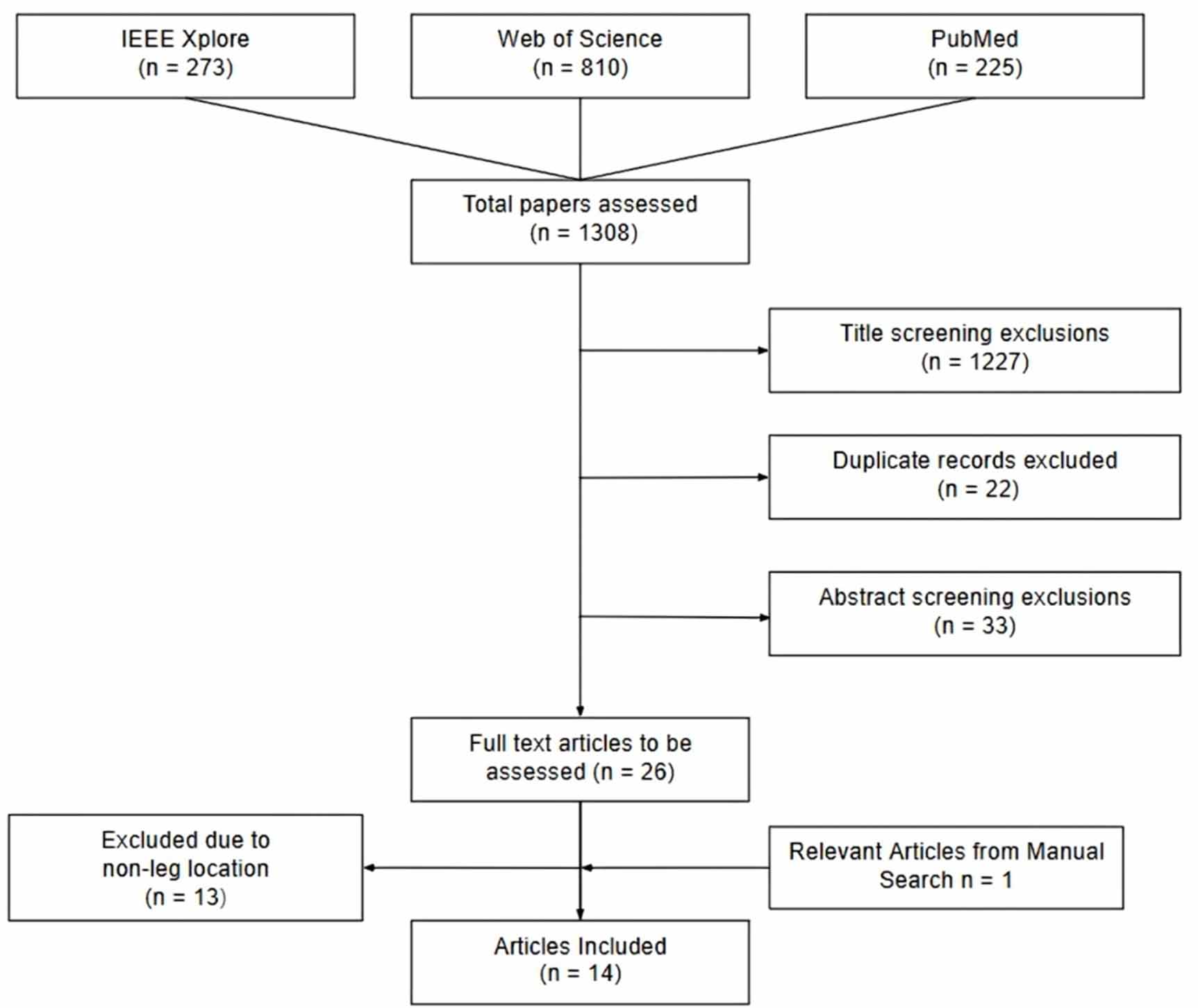
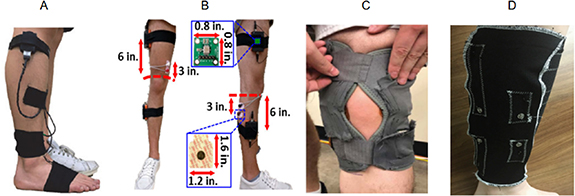
With a wearable device as shown in figure 2(A), Gutiérrez-Carretero et al (2024) demonstrated BI as a strong prognostic tool, identifying a threshold of ⩽21.8 Ω BI value that predicted significantly lower survival over almost 37 months in 76 acute HF patients (mean age 66, 71% male). Lower BI values were associated with increased peripheral edema, elevated NT-proBNP levels—a biomarker released by the heart under stress—and impaired cardiac function, including reduced left ventricular ejection fraction (<50%) and right ventricular dysfunction, highlighting BI’s potential to reflect underlying disease severity.
Figure 2. Wearable BI device designs from (A) Reproduced from Gutiérrez-Carretero et al (2024). CC BY 4.0. (B) Reproduced from Sánchez et al (2024). CC BY 4.0. (C) © 2023 IEEE. Reprinted, with permission, from Scagliusi et al (2023b); an (D) Reproduced from Scagliusi et al (2023a). CC BY 4.0. Delano and Sodini (2018) was excluded from the figure, as it did not include a wearable device at this stage of research.
Download figure:
Standard image High-resolution imageSince long-term monitoring depends on patient comfort and adherence, Sanchez et al (2024) developed wearable textile electrodes for continuous leg BI measurements (figure 2(B)). Their system showed high repeatability and successfully distinguished two HF patients from five healthy controls by comparing their BI data at different times of the day, with HF patients showing significantly lower BI values.
Scaliusi et al (2023b) tested a low-cost wearable device in real-world conditions (figure 2(C)). Over a month, the device monitored one HF patient and one healthy control, reliably capturing fluid changes that matched clinical observations of edematous tissue and healthy tissue. This highlights the potential of BI measurements to support daily monitoring and early detection of worsening symptoms outside the hospital.
Scaliusi et al (2023a) also assessed another version of their prototype in terms of the ability to track extracellular volume and circadian changes (figure 2(D)). In four healthy and two HF participants, impedance patterns in healthy individuals were stable and less sensitive to small volume changes, while HF patients showed greater variability and responsiveness—consistent with more fluid buildup. The device also detected daily volume fluctuations, supporting the use of calibrated low-frequency BI for continuous fluid monitoring.
Finally, Delano and Sodini (2018) extended this work to dialysis, monitoring nine chronic HF patients where precise volume management is critical. They observed heterogeneous responses during dialysis: 65% had decreased calf extracellular water (cECW), 29% had no change, and 6% showed increases. Changes in total calf water correlated with ultrafiltration volume and rate (R2 = 0.23–0.27 overall; up to 0.55 in CHF patients). Calf normalized resistivity is also related to baseline extracellular-to-total water ratio (R2 = 0.63) and pedal edema scores (R2 = 0.56), confirming the method’s sensitivity to fluid shifts and its clinical value for personalized volume assessment.
Together, these studies highlight the growing importance of wearable BI for managing congestion in HF. Its ability to non-invasively, continuously, and comfortably track edema positions it as a promising technology to improve outcomes through timely, tailored interventions. Figure 2 illustrates the HF studies that used wearable devices for impedance monitoring.
3.2.2. Overview of non-HF related studiesComplementing the HF research, a growing number of studies have explored wearable BI spectroscopy (BIS) for fluid and tissue monitoring in non-HF populations. These address challenges in injury assessment, dialysis hydration, vascular dynamics, and hardware design, pushing BIS toward wider clinical use.
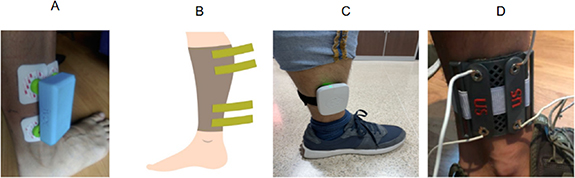
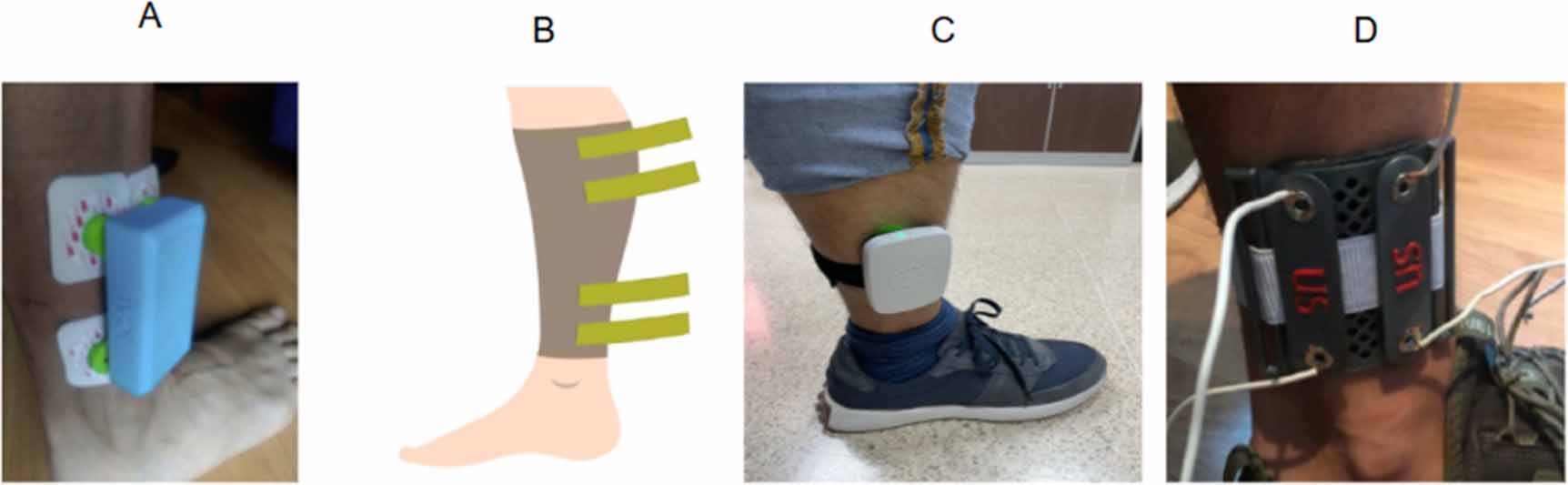
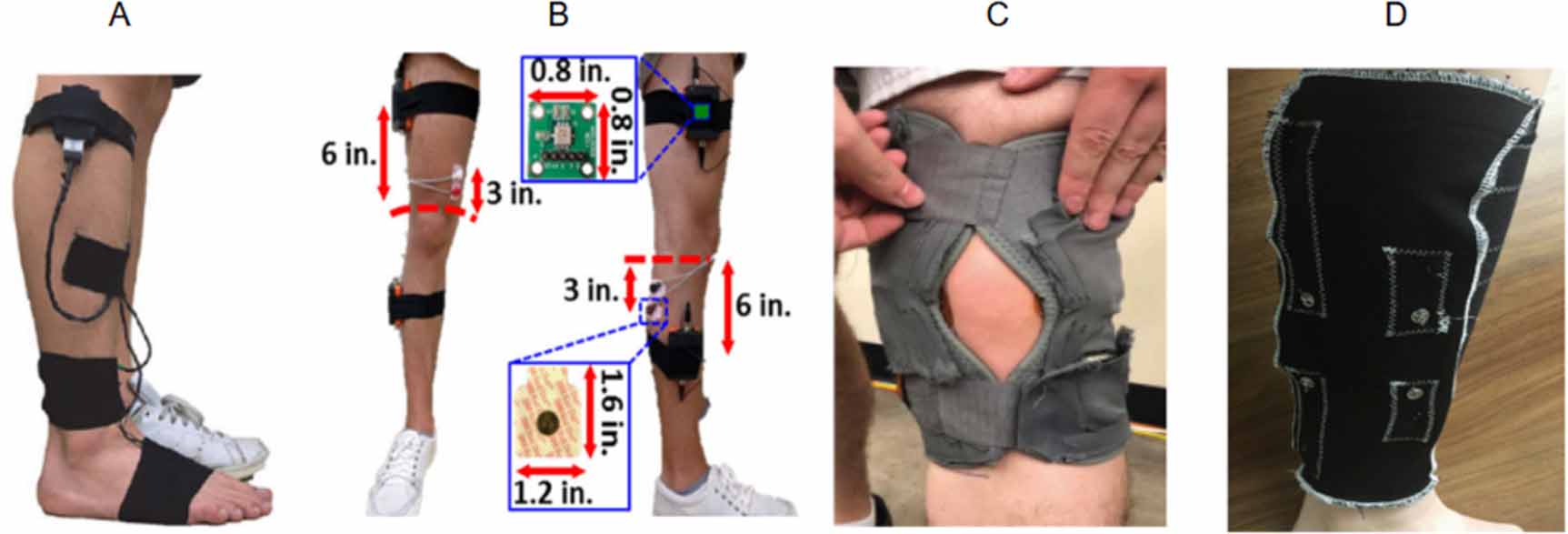
A key focus has been using BIS for injury detection and recovery. Mabrouk et al (2020) introduced a method to monitor edema without interfering in the participants’ daily life by taking participant movement into the evaluation. They proposed the hα parameter, which is an empirical parameter that relates the range of change in BI changes at high frequency (1000 kHz) due to positional changes, to the range of change in BI at low frequency (5 kHz) associated with those changes (Mabrouk et al 2020):

The hα parameter was used to detect ankle edema, and the results showed significantly lower values in injured ankles (∼0.6) compared to healthy ones (∼1.0), with minimal overlap and low variability—outperforming traditional impedance measures. In other words, participants with injured ankles showed more extracellular edema than their healthy counterparts.
Hersek et al (2017) extended this to knees, showing injured knees had consistently lower resistance and altered reactance than healthy knees. As patients recovered post-surgery, these differences decreased by over 70%, indicating reduced swelling and improved tissue health. These findings show wearable BIS can monitor joint health, aiding both injury detection and recovery tracking.
Mabrouk et al (2021) further validated hα during walking, introduced a β parameter linked to tissue integrity, and showed strong correlations (p ≪ 0.01, r = 0.8) with edema indicators, distinguishing injured from healthy ankles with high sensitivity. Measuring BI at key moments in the gait cycle preserved diagnostic accuracy while reducing data needs, advancing low-power wearable injury monitors.
Beyond joints, Villa et al (2016) examined multiple parts of the body (right thigh, pelvis, and left thigh) using a multi-segment BIS system during exercise to observe impedance decreases in active thighs and compensatory increases elsewhere, capturing dynamic vascular redistribution. The device recorded impedance every 6 s across eight frequencies, detecting rapid changes from muscle contractions and posture shifts. Sit-to-stand movements caused impedance increases in thighs and decreases in the pelvis, demonstrating sensitivity to transient, localized fluid shifts. Hersek et al (2016) combined knee and cardiovascular impedance, showing injured knees had ∼14 Ω lower resistance and ∼5.25 Ω reduced negative reactance, while cardiovascular signals matched ECG and cold pressor test results, highlighting BIS’s versatility.
Critcher and Freeborn (2021) recognized the need for a durable printed circuit board (PCB) suitable for long-term wearable use and tested a flexible design that could adapt to the shape of a device. During a week-long test of three healthy volunteers, one participant maintained stable signals, while others experienced signal instability due to trace cracking, highlighting the need for more robust hardware solutions.
In dialysis, Montabélit et al (2016) observed similar impedance changes in both HD patients and controls. Although results were not statistically significant, the results indicated that there was not a major difference between the two groups. Using a commercial SFB7 device with Ag/AgCl electrodes, calf BI parameters R0 and R∞ gradually increased during 2–4 h sessions. Postural changes from standing to lying caused rapid impedance increases, indicating body position strongly affects BI. This challenges the assumption that rising R0 during HD is caused solely by the treatment itself, as it could be influenced by the position the participants are in. Zhu et al (2008) confirmed BIS’s sensitivity to fluid removal after dialysis, linking excessive fluid loss beyond dry weight to hypotension. Continuous calf BIS detected precise reductions in extracellular and total body water, with low variability (∼0.3%). These studies highlight BIS’s promise for dialysis hydration monitoring, while emphasizing posture and fluid shift control for accurate measurements.
To improve real-world usability, Delano et al (2022) developed a wearable BIS sock to measure calf impedance. Bench tests showed R0 and R∞ estimates within ±1.5% of the gold standard but non-wearable commercial device, SFB7. In five healthy volunteers, repeated measurements had precision better than 2% using Ag/AgCl electrodes. However, textile sock electrodes showed low-frequency artifacts below 5 kHz, reducing precision to ∼4% and causing inconsistent model fits. Applying pressure or wetting the electrodes improved results. Overall, the wearable sock performed comparably under ideal conditions but revealed challenges with skin-electrode impedance in textile electrodes.
Together, these studies broaden wearable BIS’s scope beyond HF, offering new methods to monitor edema across conditions. Many techniques—like segmental measurements, flexible PCBs, and postural controls—can be further investigated and adapted to improve HF monitoring, showing BIS’s cross-cutting potential in personalized care. Figure 3 illustrates wearable devices used in the non-HF papers for impedance monitoring.
Figure 3. Wearable BI device designs from (A) © 2021 IEEE. Reprinted, with permission, from Mabrouk et al (2021); (B) © 2017 IEEE. Reprinted, with permission, from Hersek et al (2017); (C) Reproduced from Critcher and Freeborn (2021). CC BY 4.0; and (D) Reproduced from Delano et al (2022). CC BY 4.0. The remaining five papers were excluded from the figure, as they did not include illustrations of wearable devices.
Download figure:
Standard image High-resolution image 3.2.3. Summary and discussionOverall, these findings reinforce the clinical versatility of wearable BI systems. Across HF and non-HF populations, BIS has demonstrated the ability to non-invasively detect edema, monitor dynamic fluid changes, and support long-term tracking of physiological status—all while being compatible with wearable, real-world use. Tables 3 and 4 summarize key findings from HF- and non-HF-related studies, highlighting device portability, measurement sites, fluid detection or monitoring, and methodology.
Table 3. Summary of the HF-related papers results.
AuthorPortable device usedLower limb site measuredFluid detectedMeasurement methodGutiérrez-Carretero et al (2024)✔Ankle✔Single sessionSánchez et al (2024)✔Ankle✔Short-termScaliusi et al (2023b)✔Calf✔Short-termScaliusi et al (2023a)✔Ankle✔Long-termDelano and Sodini (2018)✖Calf✔Single sessionTable 4. Summary of the non-HF related papers results.
AuthorPortable device used?Lower limb site measuredFluid monitored?Measurement methodDelano et al (2022)✔Calfn/aSingle sessionCritcher and Freeborn (2021)✔Knee✖Short-termMabrouk et al (2021)✔Ankle✔Long-term & single sessionMabrouk et al (2020)✔Ankle✔Single sessionHersek et al (2017)✔Knee✔Long-termVilla et al (2016)✔Thighs & Pelvis✔Single sessionMontalibet et al (2016)✖Calf✔Single sessionHersek et al (2016)✖Knees✔Single sessionZhu et al (2008)✖Calf✔Long-termMeasurement approaches are categorized as single sessions (all data collected in one encounter), short-term (monitoring over days but less than a week), and long-term (over one week). Mabrouk et al (2020) notably used longitudinal monitoring for healthy participants but single-session assessments for injured ones, showing BIS protocols can adapt to study goals and participant status.
3.2.3.1. Frequency considerationsAmong the studies reviewed, most employed multi-frequency BI, with eleven of these studies using either dual-frequency or broadband systems covering 3 kHz – 1 MHz. These systems enable more precise compartmental resolution and greater sensitivity in detecting fluid shifts. Only four studies relied on single-frequency measurements, three of which used 50 kHz (Hersek et al 2017, Mabrouk et al 2021, Scagliusi et al 2023a), a common midpoint frequency that partially captures both ECF and ICF but does not fully differentiate between them. One study used 5 kHz (Zhu et al 2008), which primarily captures ECF changes during dialysis but misses intracellular or total body water dynamics. Broadband approaches are increasingly favored, especially in wearable BI systems, due to their superior ability to continuously monitor complex hydration changes.
3.2.3.2. Number and position of electrodesA key aspect of BI is the use of electrodes to inject current and measure voltage across tissue. Although two electrodes (bipolar) are the minimum required, this setup is rarely used bec
Comments (0)