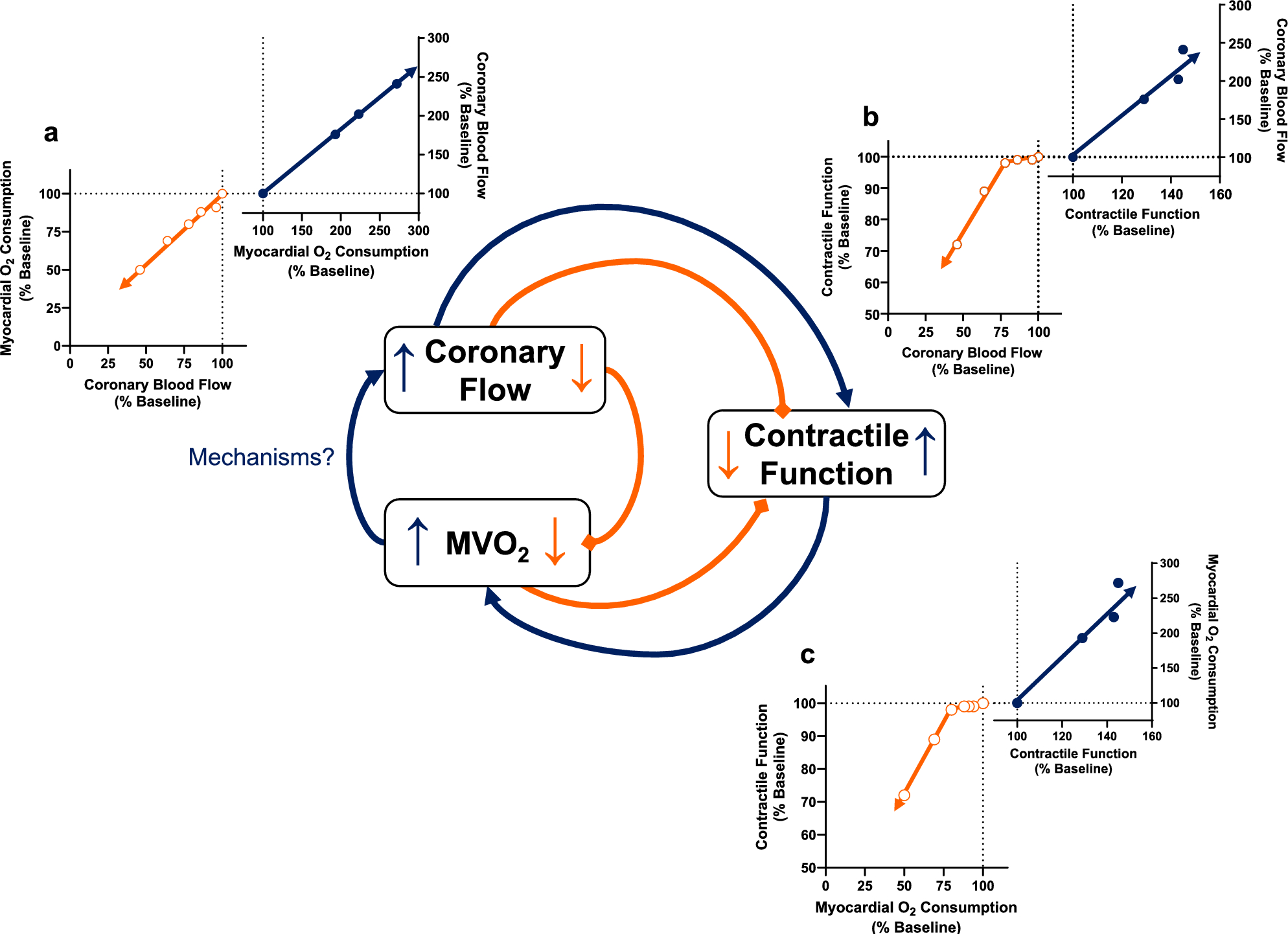
Following over a century of research, understanding of the mechanisms responsible for the coupling of coronary blood flow with myocardial metabolic requirements has remained elusive. Discovery of specific factors/pathways continues to be confounded by continued debate around anticipated experimental outcomes and interpretation of complex circular relationships (Fig. 1) between key variables that are inconsistently measured and reported throughout the literature [14]. To directly address this matter, the present studies were designed to interrogate interrelationships between decreases (CPP and 4-AP) and increases (dobutamine) in regional wall thickening and MVO2 in the absence and presence of either constant or reduced coronary flow conditions. Our findings support the hypothesis that impairments in the control of coronary blood flow are consistently characterized by progressive decreases in contractile function in response to reductions in volume of myocardial perfusion per beat below ~ 5.0—7.5 μL/g/beat [16]. Results highlight the need for concurrent measurement of contractile function, coronary flow, and MVO2 and corroborate that antagonist-mediated contractile dysfunction should be corrected by the restoration of coronary flow to normal, pre-treatment levels [14, 27]. Data also provide a definitive framework of anticipated outcomes to guide future investigation of local metabolic mechanisms of coronary blood flow control.
Interrelationships between coronary blood flow, contractile function, and MVO2
It is well established that increases in cardiac contractile function and MVO2 are directly linked with proportionate increases in coronary blood flow [17, 21, 28, 29]. Conversely, limitations in coronary flow produce commensurate reductions in MVO2 and contractile function (Fig. 1). How then would the inhibition of metabolic factors that link perfusion to metabolism influence these variables? Would not primary alterations in flow or MVO2 simply follow the prescribed relationships outlined in Fig. 1? To what extent would the slopes of these relationships change? How do changes in myocardial oxygen extraction influence these interrelationships? What if the factor/pathway blocked only influenced coronary flow under baseline resting conditions? What would happen to the relationships if local metabolic control was completely abolished? The lack of definitive answers to these, and many other related questions continues to plague the field and thus was the major impetus for this study.
Our results confirm the presence of a threshold of coronary flow, below which MVO2 (Fig. 2a) and contractile function (Fig. 2b) begin to fall [16, 20]. This threshold was shifted to lower levels of flow as initial reductions in CPP were accompanied by increases in myocardial oxygen extraction that were sufficient to sustain MVO2 and wall thickening at baseline levels at CPPs ≥ 60 mmHg. Findings also verify that if antagonist-mediated reductions in MVO2 (Fig. 2d) and function (Fig. 2e) are related to deficits in perfusion, they should be corrected by the restoration of coronary flow to normal, pre-treatment levels [14, 27]. Data from this investigation also established physiological windows that reflect relative operating ranges for changes in regional wall thickening and MVO2 as coronary blood flow is limited during increases in cardiac workload (Fig. 3). These functional “loops” highlight expected limits of variable degrees of inhibition of any potential local metabolic factor(s)/pathway(s), down to the elimination of changes in blood flow which correspond with an ~ 35% reduction in wall thickening and an ~ 50% increase in MVO2 relative to normal baseline levels. This increase in MVO2 is in fact exaggerated in this study by the lower levels of oxygen extraction (baseline = 46 ± 5%; Table 3) observed in our cannulated, extracorporeal perfused coronary preparation. Thus, the working physiological range for changes in the relationship between coronary blood flow and MVO2 is likely smaller than that depicted in Fig. 3a. The functional coronary “loops” presented in Fig. 3 were generated using coronary flows at or above baseline values and thus do not depict effects of potential antagonist-mediated reductions in baseline coronary blood flow.
Balance between coronary blood flow and MVO2
Dogma of the coronary field has long held that inhibition of a local metabolic pathway will decrease the balance between coronary flow and MVO2 [11,12,13,14, 18]. Evidence to support the impairment of “supply/demand balance” has largely centered around increases in myocardial oxygen extraction and predicted reductions in coronary venous PO2 relative to changes in MVO2 (see Fig. 4a) [11, 13, 30,31,32]. While augmented oxygen extraction is a logical consequence of reductions in coronary flow, the degree of compensation is quite limited as the left ventricle typically extracts ~ 75–80% of the oxygen delivered at rest [12, 13, 33]. Accordingly, MVO2 is highly dependent on coronary blood flow, and thus any reduction in flow will lead to a proportional reduction in myocardial oxygen delivery and thus MVO2 (see Fig. 1a; [13]). Consequently, it is important to recognize that the slope (i.e. “balance”) between coronary blood flow and MVO2 cannot be appreciably altered within these physiologic constraints. The interdependence of these variables is also evident in calculation of MVO2 as the product of coronary blood flow and the arterial-coronary venous difference in oxygen content. As such, analysis of the relationship between MVO2 and coronary blood flow is inherently confounded by the fact that coronary blood flow is represented on both the ordinate and abscissa of the relationship [14]. This point is highlighted in the present study by the relatively modest increase in MVO2 when coronary flow is clamped at baseline levels during systemic dobutamine administration (Fig. 3a). As outlined above, this increase in MVO2 is higher than normal as resting oxygen extraction was significantly reduced in our cannulated preparation.
Use of coronary venous PO2 vs. MVO2 as an assessment of the balance between myocardial oxygen delivery and metabolism introduces its own set of complications. Current results highlight characteristic decreases in coronary venous PO2 (Fig. 4a) in response to changes in CPP (~ 30%; Table 1), to increases in MVO2 (~ 10%; Table 3), and to reductions in coronary flow with elevated MVO2 (~ 25%; Table 4). However, interpretation of differences in nonlinear responses and/or parallel shifts vs. changes in slope of the coronary venous PO2 and MVO2 relationship continue to obscure definitive conclusions. Underlying differences between species [11, 14] and divergent responses to similar patho-physiologic perturbations (e.g. anemia vs. hypoxemia [14]) further confound the utility of this relationship as a reliable means to assess potential mechanisms of coronary flow control.
Perfusion-contraction matching
Our group recently proposed the primary criterion to apply to experimental studies of local metabolic control is that inhibition of the factor/pathway should attenuate the coronary flow response to changes in MVO2 [14]. Although such an effect cannot markedly diminish the slope of the relationship between coronary blood flow and MVO2 (i.e. overall supply/demand balance), there is substantial evidence to support that the adequacy of myocardial perfusion is reflected by changes in regional contractile function [16, 17, 19, 20, 22, 23, 28, 29, 34,35,36]. To examine the perfusion-contraction matching paradigm in the context of local metabolic control, we assessed the relationship between systolic wall thickening and coronary blood flow per beat for all groups in this study. As shown in Fig. 4b, dobutamine-mediated increases in heart rate were matched by increases in coronary blood flow such that the volume of flow per beat remained essentially unchanged. However, the black regression line in Fig. 4b demonstrates wall thickening decreased in direct proportion to reductions in coronary flow per beat in all experimental groups (P < 0.001; R2 = 0.57), regardless of whether the decrease was due to a decrease in “supply” (↓ CPP, 4-AP) or a limitation of flow during increases in “demand” (flow reduction vs. flow clamp with dobutamine). These data are consistent with the findings of Gallagher et al. who were the first to observe that the level of contraction is determined by the availability of blood reaching the myocardium on a per beat basis both at rest and during exercise [20]. The progressive decrease in wall thickening as flow per beat falls below an apparent threshold of ~ 5.0—7.5 μL/g/beat is consistent with advancing degrees of myocardial ischemia as proposed by Heusch [16, 23]. More importantly, the escalation of contractile dysfunction in response to antagonist-mediated flow reductions is consistent with the increased contribution of the inhibited pathway to metabolic coronary vasodilation. Accordingly, we submit that progressive decreases in contractile function as a consequence of reductions in coronary flow per beat represents a more reliable means by which to interrogate potential mechanisms of local metabolic control of coronary blood flow.
Limitations of the study
It is important to appreciate that the present results relate to relationships within and below the autoregulatory range, but not above it [37]. Additionally, anesthetized/cannulated preparations typically display poor autoregulation and lower levels of myocardial oxygen extraction in comparison to conscious preparations [28, 38,39,40]. This augmented oxygen extraction reserve could influence the critical threshold at which regional contractile function begins to decline as coronary flow per beat is reduced. Positioning of the threshold could also be shifted by changes in hematocrit, myocardial compressive forces, or by endogenous factors such as nitric oxide that impact myocardial efficiency by reducing MVO2 and conserving contractile function [15, 41]. Thus, it is not surprising that the critical flow per beat necessary to induce reductions in regional wall thickening ranged from ~ 5.0 mL/g/beat (↓ CPP) to ~ 7.5 μL/g/beat (Dobutamine ↔ flow) (Fig. 4b). While the experimental preparation and/or condition may influence the value of this threshold, the primary conclusion that impairments in coronary flow control are reliably demonstrated by decreases in contractile function as a consequence of reductions in coronary flow per beat remains evident. In the absence of measures of high energy phosphates, the extent to which this perfusion-contraction matching reflects short term hibernation or overt ischemic contractile dysfunction remains to be determined [42].
We acknowledge that reductions in regional contractile function are largely dictated by decreases in subendocardial blood flow [19, 20, 28] which was not assessed in the present study. However, this limitation is tempered by the paucity of collateral blood flow and the subendocardial dominance of transmural assessments of regional contractile function and perfusion in swine [43]. Transmural flow heterogeneity also confounds interpretation of global assessments of variables such as MVO2, myocardial oxygen extraction and lactate uptake/release, which not only vary between the subepicardium and subendocardium but also fail to achieve true steady state levels during myocardial ischemia [44]. Prior studies suggest that examination of systemic inotropic stimulation on regionally ischemic myocardium is confounded by effects on nonischemic regions [22]. Accordingly, we acknowledge that percent wall thickening may underestimate the work relevant for MVO2 as LV pressure is elevated by dobutamine [22]. Return of regional contractile function to normal baseline levels after transient ischemic episodes (↓ CPP or Dobutamine ↓ flow) could also reflect some degree of recruitment of inotropic reserve at the cost of impaired metabolic performance and shifts toward alternative energy sources such as creatine phosphate and lactate production [45].



Comments (0)