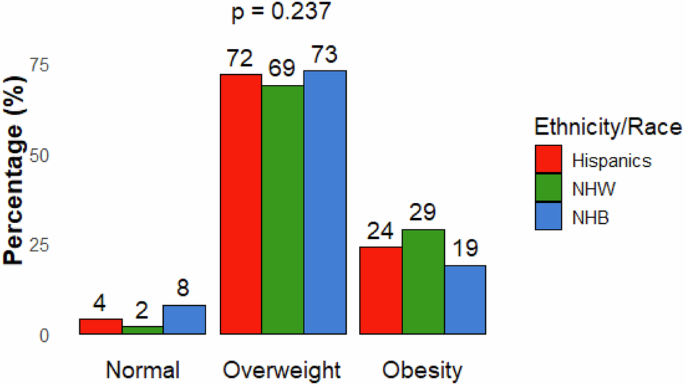
The USA-OBESTIGMA study interviewed adults with obesity in two academic medical centers in Atlanta (Georgia) and Miami (Florida). We observed several important differences in weight stigma among racial and ethnic groups with obesity in the U.S. First, we noticed that despite all participants having obesity (mean BMI ~ 37 kg/m2), only 24% of Hispanic, 29% of non-Hispanic White, and 19% of non-Hispanic Black participants had the self-perception of having obesity. Most considered themselves having overweight, with 72% of Hispanic, 69% non-Hispanic White, and 73% non-Hispanic Black individuals. Second, Hispanic adults reported higher aversion and prejudice towards people with obesity, compared to their non-Hispanic White and non-Hispanic Black counterparts, as measured by the AFA survey. Third, non-Hispanic White individuals reported higher scores on stigmatizing experiences than Hispanic and non-Hispanic Black participants. Fourth, non-Hispanic Black individuals reported lower internalization of negative weight bias scores compared to Hispanic and non-Hispanic White individuals.
It was not surprising that there are high rates of weight misperception among minorities with a BMI ≥ 30 kg/m2 in the U.S. Prior studies have shown that racial and ethnic minority groups, including Hispanic and Black adults, may have a higher prevalence of misperceived weight status [13, 17, 18]. This misperception could be influenced by cultural norms surrounding body image, where a larger body size may be more socially accepted or preferred within certain communities. Additionally, differences in exposure to health education, healthcare access, and societal weight norms may contribute to these variations in self-perception [13, 17].
Racial and ethnic differences in weight-related stigma can be attributed to a variety of factors, including socioeconomic status, cultural norms, and personal experiences. Cultural attitudes towards body weight and shape can vary significantly across different racial and ethnic groups. It is well established that body size and ideal body weight are stigmatizing factors in Hispanic communities, albeit with some differences across countries of origin. For example, Caribbean communities may consider a larger and curvy body as desirable, while other groups may prefer slender body sizes or contours [18, 19]. This again highlights the associated stigma related to obesity, seen by many still as a body image disorder and not an actual chronic metabolic disease with several associated complications. Compared to Hispanic adults, non-Hispanic Black individuals had a lower AFA score, suggesting they are more accepting of people with larger body sizes. This may also explain why non-Hispanic Black individuals had the lowest scores for internalization of negative bias [20]. Recent studies also found that non-Hispanic Black individuals had lower weight bias internalization than other racial and ethnic individuals [21, 22]. Our study also found SSI-B score were lower for non-Hispanic Black individuals, and higher in non-Hispanic White females, aligning with recent studies of diverse U.S. samples [23, 24]. These findings suggest that societal and cultural perceptions of body weight play a role in weight-related stigma and bias internalization across racial and ethnic groups. These findings highlight the need for better education among patients, emphasizing the implications of obesity as a chronic disease of excess adiposity and explaining the different risk categories [25].
Our study also examined how the degree of obesity and personal characteristics influence negative feelings and stigma. The statistically significant negative association between BMI and AFA scores suggests that individuals with higher BMI might be less likely to have prejudice against other people with obesity, possibly due to a coping mechanism or resilience developed over time. Similarly, in multivariate analysis of AFA scores, we found no differences after adjusting for age and gender, but a negative correlation with type 2 diabetes.
The association of higher SSI-B scores with lower education levels highlights the compounded stigma faced by less-educated individuals [11]. One might assume that people living with a disease would be more understanding toward others having the same condition. However, this does not appear to be the case regarding anti-obesity attitudes. Higher degrees of obesity are associated with higher internalized stigma scores, which creates a challenging cycle where negative self-perception can impede effective weight management and potentially contribute to further weight gain [10]. This internalized stigma is often compounded by experiences with healthcare providers, where weight bias can lead to poor communication and inadequate care, ultimately affecting health outcomes and patients’ willingness to seek treatment [26, 27]. Guidelines emphasizes that healthcare providers must confront the widespread issue of fat bias in clinical settings, advocating for increased awareness of weight-biased attitudes and deeper understanding of weight management’s complexities among medical professionals [28].
Notably, we found that SSI-B scores decrease with age, suggesting that younger individuals are exposed to the most weight-related stigmatization experiences. This finding aligns with recent research from a cross-sectional survey of adults with obesity, which demonstrated that individuals with severe obesity before the age of 18 years were nearly three times more likely to report severe experiences of weight stigma compared to those who developed severe obesity later in life ( > 18 years of age) [24]. Similarly to their findings, we found that “Having a doctor recommend a diet, even if did not come in to discuss weight loss”’ was the most common stigmatizing experience among the three groups [24]. Other study among university students in nursing and social work careers in the U.S. and Turkey reported similar patterns, in which younger students had worse scores [29, 30]. Furthermore, the OBESTIGMA study in Spain, recruiting over 1200 participants, with a mean age of 33.3 years, reported that younger participants had more frequent stigmatizing experiences [11]. This highlights the heightened vulnerability of younger individuals to weight stigma and shows that our society, whether in Europe or the U.S., still lacks an inclusive environment for people with obesity. These findings support the incorporation of obesity and stigma in the curriculum, not only for medical or health-related students, but also in the general population, and at early ages. We advocate for professional societies, patient advocacy groups, and society to incorporate these findings into future educational programs. Obesity stigma can lead to poor communication and inadequate care for individuals with obesity, ultimately affecting their health outcomes and willingness to seek treatment [26, 27].
The strengths of this study include a diverse patient population from two large metropolitan areas, inclusion of a diverse ethnic population, the use of multiple surveys, and the exploration of the relationship between obesity and sociodemographic variables. However, the study has a few limitations, including a smaller sample size compared to similar studies in other countries [11]. The small sample size may limit generalizability to the U.S. population. We used BMI to define obesity, which has inherent limitations. Several experts and professional societies have advocated using metrics to diagnose, stage, and manage obesity beyond BMI, including validating metrics such as waist-to-height ratio, body composition studies, and clinical/complications [18]. Although our study actively recruited participants from three specific racial/ethnic groups with balanced representation, we recognize that our Florida-based sampling, where Hispanic/Latino populations constitute a larger demographic proportion than in many other U.S. regions, may not accurately reflect the racial/ethnic distribution of the general U.S. population. This geographical concentration potentially limits the generalizability of our findings to the broader national context despite our efforts to minimize selection bias. In the future, it would be interesting to repeat our approach while incorporating other variables that more reliably address excess adiposity associated with obesity. Additionally, due to the observational nature of the study, associations cannot be interpreted as causal relationships. Lastly, the reliance on self-reported data introduces the potential for recall or social desirability bias.

Comments (0)