
Remember me


Prior to its commencement, the protocol for this systematic review was formally documented in the PROSPERO database (ID: CRD420250632120; available at: https://www.crd.york.ac.uk/PROSPERO/view/CRD420250632120), following the PRISMA guidelines to ensure transparency and rigor [9]. Definitions for radiological outcomes, including MFTA, FCCA, TCCA, TCPT, and LFCFEA, are provided in Table 1.
Table 1 Operational definitions of radiographic metricsSearch strategyA comprehensive search of the PubMed, Web of Science, Cochrane Library, Embase, Scopus, ClinicalTrials.gov, China National Knowledge Infrastructure (CNKI), Wanfang, China Biology Medicine Disc (CBM), and China Science and Technology Journal (CSTD) databases was performed to identify comparative studies of MAKO-UKA and C-UKA published before October 2025. The detailed search algorithms for each database, including Boolean operators and search terms, are provided in Supplementary Data 1.
Two independent reviewers (X.J.Z and Q.M.) screened all titles, abstracts, and full texts to identify eligible studies. Discrepancies were resolved through consultation with a third senior investigator (C.J.S). Inter-rater reliability was evaluated using Cohen’s κ coefficient.
Inclusion and exclusion criteriaStudies qualified for inclusion if they utilized a comparative design (such as RCTs or observational cohorts) focusing on patients with end-stage knee osteoarthritis treated with either robotic or manual UKA. Eligibility further required the assessment of at least one clinical or radiographic parameter, including VAS, PCS, AKSS, AKSS Total, AKSSF, OKS, FJS, MFTA, FCCA, TCCA, TCPT, LFCFEA, FCCA outlier, TCCA outlier, operation time, ROM, Complication rate, PJI rate, and revision rate. Furthermore, we only considered studies providing enough raw data to derive effect sizes, specifically risk ratios (RR), odds ratios (OR), or mean differences (MD). Conversely, non-primary research—such as narrative reviews, editorials, and case series—along with conference abstracts and any publications lacking extractable quantitative results, were strictly omitted from this analysis.
Data extraction processA pair of independent investigators (X.J.Z and Q.M.) performed the data harvesting. In instances of disagreement, a senior author (C.J.S.)was consulted to reach a consensus. The information harvested from each trial spanned three primary domains: trial-specific descriptors (including authorship, publication year, geographic origin, and methodology), patient-level baseline attributes (notably age, gender distribution, body mass index, and monitoring duration), and all pre-specified clinical outcomes. To maintain the integrity of our dataset, we proactively reached out to the primary investigators via electronic correspondence whenever essential data points were absent or required further explanation.
Data transformationFor trials that reported medians with ranges or interquartile ranges, we reconstructed the corresponding means and standard deviations (SDs) to ensure data consistency. This approximation was based on the mathematical frameworks validated by Luo et al. [9] and Wan et al. [9]. Such imputation techniques are well documented in the literature [10,11,12,13]. Such imputation techniques are well documented in the literature.
Quality assessmentThe methodological rigor of the included evidence was assessed using specialized instruments tailored to the study design. Specifically, the Newcastle–Ottawa Scale (NOS) [14] was applied to observational cohorts, with a particular emphasis on the integrity of patient selection, the adequacy of comparability controls, and the reliability of outcome tracking. Concurrently, the risk of bias in randomized controlled trials (RCTs) was assessed using the standard frameworks documented in the Cochrane Handbook. This critical appraisal was conducted in parallel by two researchers (X.J.Z. and Q.M.). Any divergent assessments of study quality were reconciled through consultation with a senior investigator (C.J.S.) until consensus was reached.
Data analysesStatistical computations were performed using Stata (version 18.0; StataCorp). Continuous data were presented as mean ± SD. We quantified inter-study inconsistency using the \(\:^\) index, while the Cochran Q test was employed to identify significant heterogeneity. Given anticipated clinical and methodological diversity, all analyses employed a random-effects model using the Restricted Maximum Likelihood (REML) method [15].
Effect sizes were expressed with 95% confidence intervals (CIs). Dichotomous variables (e.g., FCCA outliers and TCCA outliers) were analysed using odds ratios (ORs), which approximate relative risk (RR) under Cornfield’s rare-outcome assumption [16]. Continuous outcomes (VAS, PCS, AKSS, AKSS Total, AKSSF, OKS, FJS, MFTA, FCCA, TCCA, TCPT, LFCFEA, operative time, and ROM) were assessed using mean differences (MDs). Statistical significance was defined by a two-tailed P-value threshold of 0.05. To detect potential publication bias, we applied Egger’s linear regression test to any outcome synthesized from eight or more independent datasets, with a P-value below 0.10 serving as the diagnostic cutoff for significant asymmetry. Furthermore, the stability of our meta-analytic results was verified through leave-one-out sensitivity procedures; by iteratively excluding one study at a time, we ensured that the overall pooled estimates remained resilient and were not disproportionately influenced by any single trial.
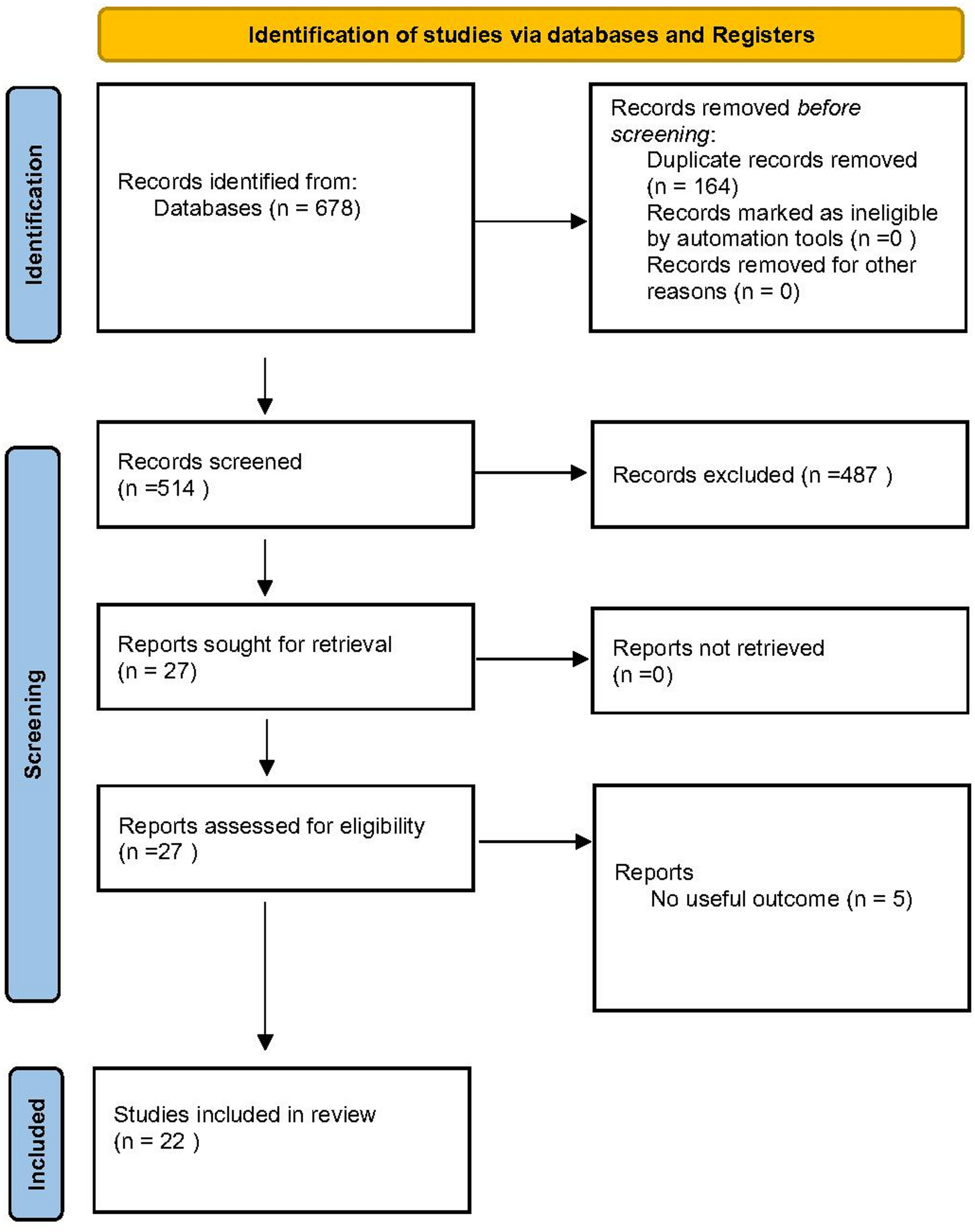
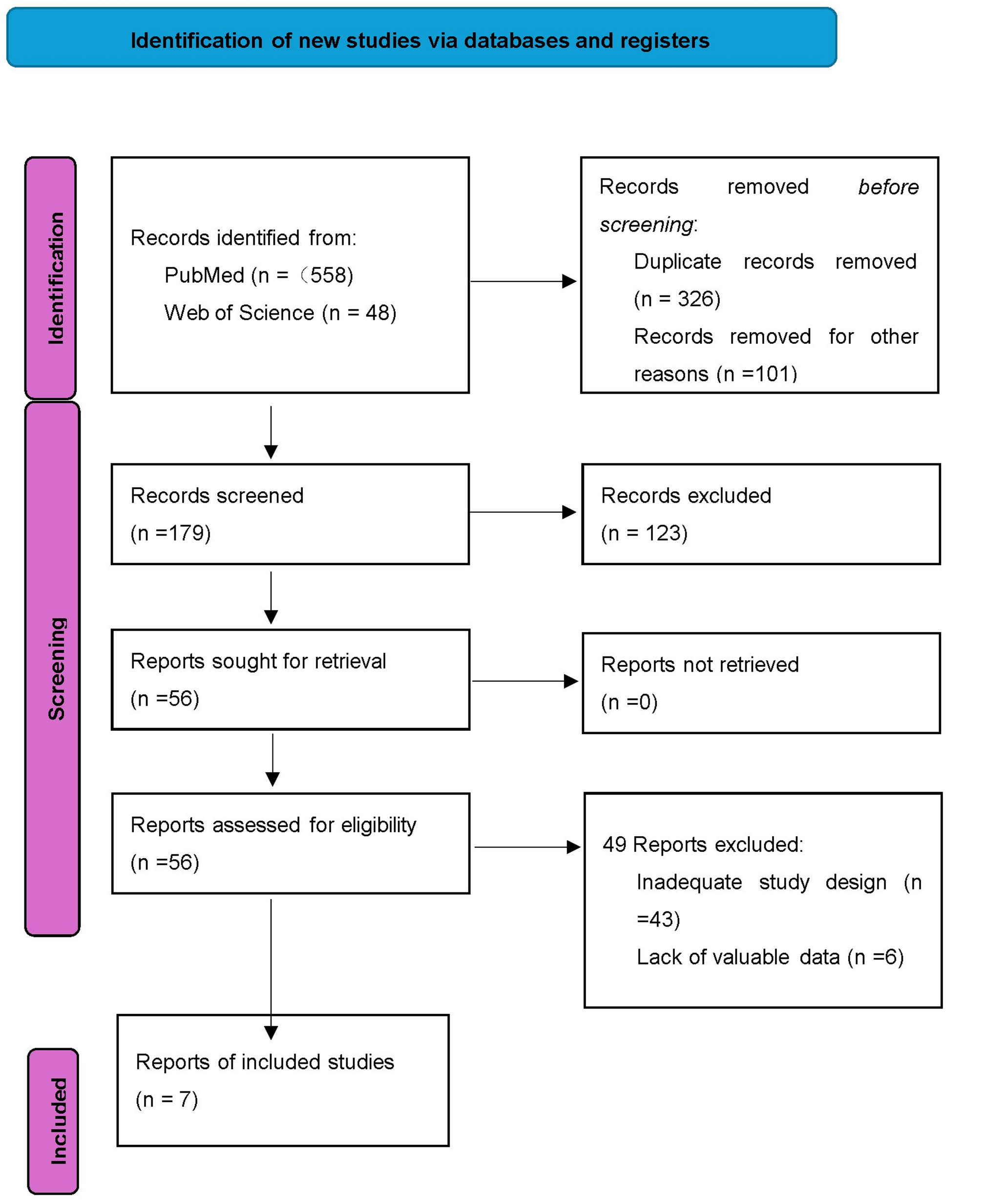
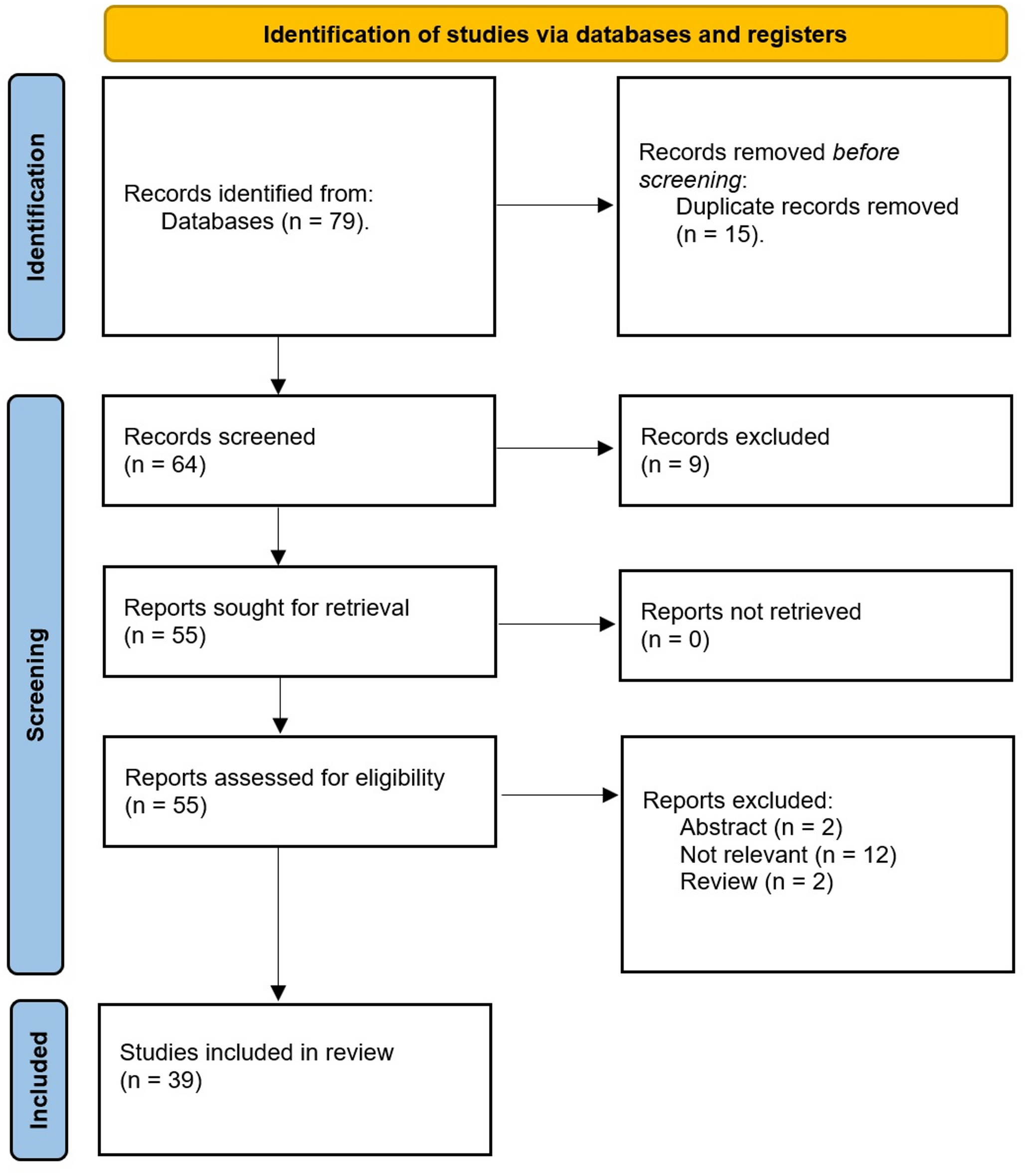
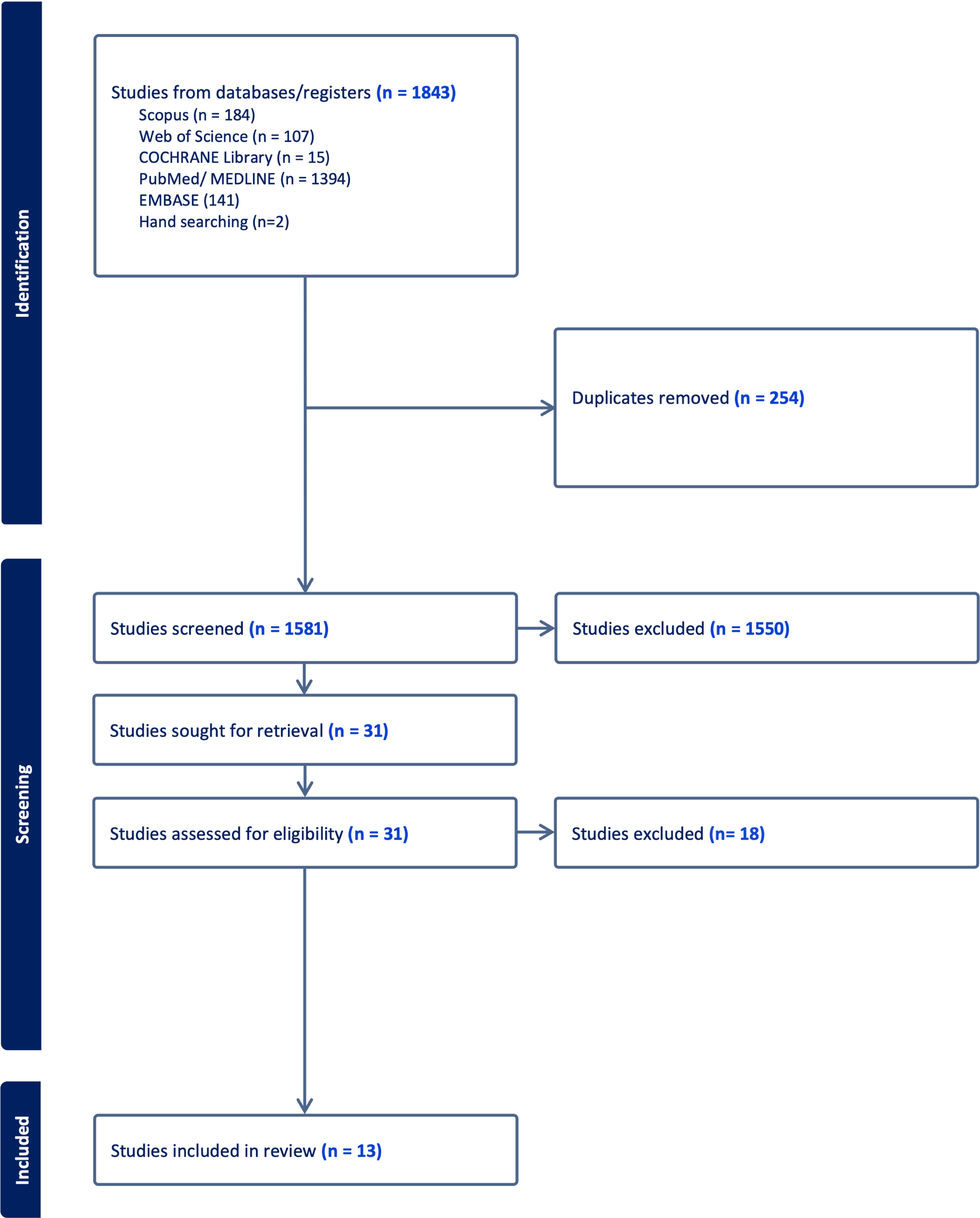
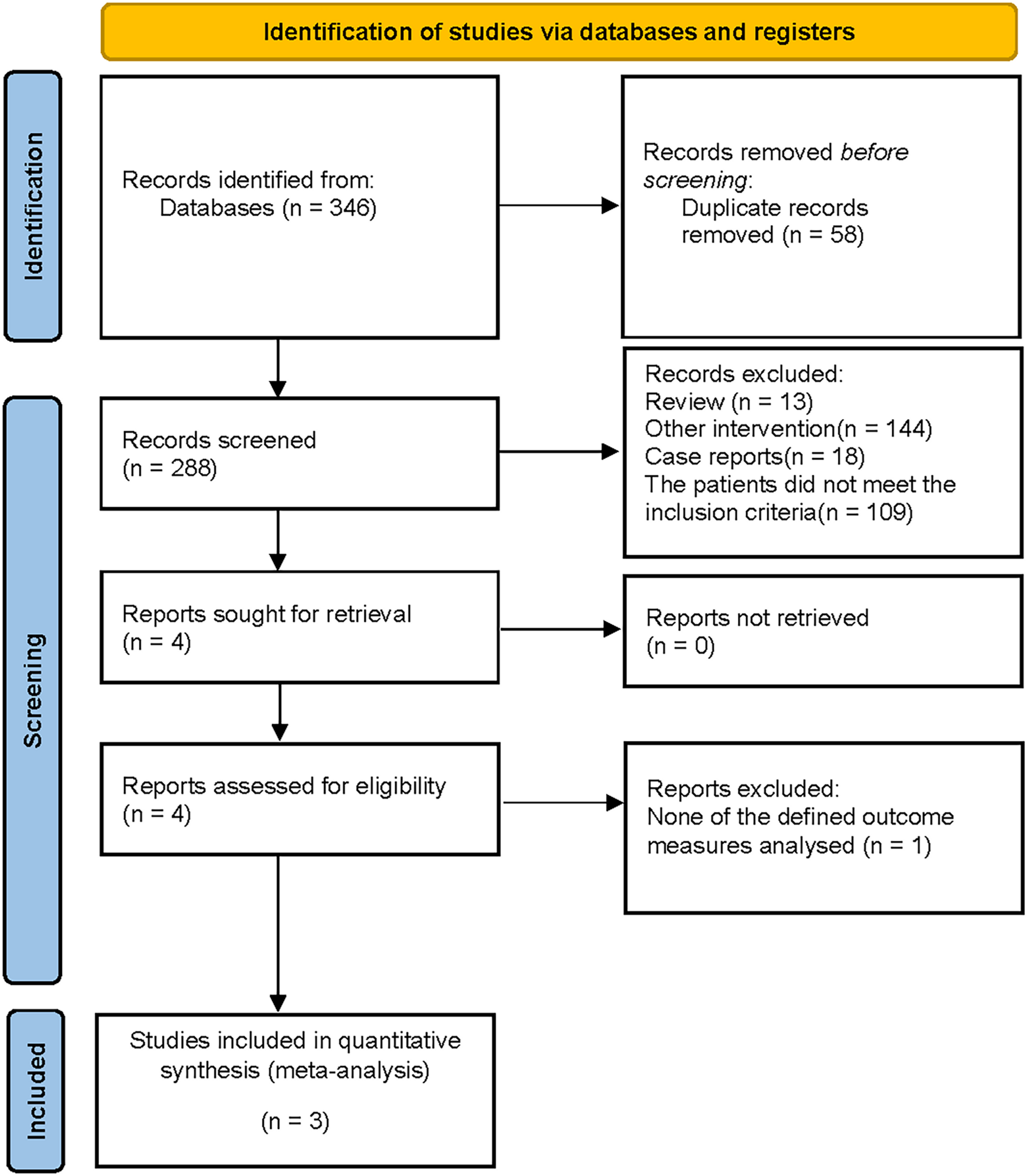
Search resultsThe PRISMA flow diagram summarizes the study selection process. (Fig. 1) The complete search strategy used for each database is provided in Supplementary Data 1. The initial database search yielded 678 records. After importing these records into Zotero, 164 duplicate records were removed. Of the remaining 514 unique articles, 487 were excluded after review of titles and abstracts for irrelevant populations, interventions, study types, or outcomes. The remaining 27 full-text articles were assessed, and 5 were excluded for insufficient or inconsistent outcome data. Ultimately, 22 studies [17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38] met the inclusion criteria. Inter-reviewer agreement was excellent (κ = 0.9040 for title/abstract screening; κ = 0.8670 for full-text review) (see Supplement data 2).
Fig. 1
Flowchart depicting the identification, screening, and inclusion of eligible literature
Sample characteristicsTables 2 and 3 provide a detailed overview of the baseline attributes and clinical outcomes collected from each trial. The literature identified for this systematic review was published between 2010 and 2025.
Table 2 Baseline profiles and descriptive attributes of included trialsTable 3 Comprehensive data reporting for all synthesized clinical and radiographic endpoints
Comments (0)