In timely re-perfused, ST-elevation AMI patients, the CXCR4-directed PET agent 68Ga-PentixaFor provided a non-invasive read-out of increased target expression in organs of systemic immune response. Established biomarkers of cardiac damage (infarct size) and systemic inflammation (CRP, WBC) failed to predict myocardial functional recovery. By contrast, cardiac baseline function and CXCR4 uptake in the spleen may be useful to identify patients predisposed to functional recovery 12 months after AMI, indicating that the PET signal provided complementary prognostic value for long-term cardiac outcome. Thus, focusing on distant organs of the systemic immune response, findings of the present trial confirm the usefulness of chemokine receptor PET of extra-cardiac organs post-AMI and tie the concept of whole-body inflammatory imaging to a relevant clinical meaning.
In a previous study, CXCR4 PET signal in the infarct territory was linked to the occurrence of major cardiovascular events [13]. Moreover, a most recent retrospective investigation also focused on the predictive value of 68Ga-PentixaFor PET post-MI to determine the predictive value for cardiac functional changes [12]. This previous work investigated a single FU with an observational period of up to 29.5 months after AMI, while the present trial included multiple FU at fixed time-points (6 and 12 months after the acute event), thereby allowing for harmonized outcome comparison within the enrolled study population. Moreover, previous work also exclusively focused on the infarct territory [12]. Results of the present prospective study, however, go beyond the myocardium as the target region, as the CXCR4 PET signal in extra-cardiac lymphatic organs (LN, spleen) was associated with left ventricular recovery after AMI. Thus, we herein demonstrate a potential added clinical value of a whole-body PET approach also imaging distant organs involved in adaptive immunity post-AMI. In this regard, as shown in uni- and multivariate analyses, increased chemokine receptor PET signal in the spleen was linked to long-term functional recovery 12 months after the acute event. Previous work has demonstrated that modulating the CXCR4 / C-X-C motif chemokine ligand 12 axis can deploy splenic regulatory T-cells from the spleen to the infarcted myocardium, which contribute to cardiac repair [18, 19]. With organs expressing CXCR4 in different cell types including lymphocytes, progenitor or natural killer cells [8,9,10], our molecular imaging approach may therefore provide a non-invasive read-out of the inflammatory cell tracking between the primary site of damage (myocardium) and remote organs of hematopoietic activation (spleen). Nonetheless, PET signal in the spleen exhibited a broad 95% CI, which can also reflect sampling variability inherent to the modest sample size. Relative to the baseline splenic uptake holding predictive potential for long-term outcome twelve months post-MI, we also observed predictive value of LN uptake at least in univariate analysis for short-term cardiac functional changes six months after the acute event. Given the anatomical proximity of heart-draining LN to the primary site of cardiac injury, this phenomenon may be explained by sequential immune activation of first LN, followed by the spleen. LN uptake, however, may also reach significance in future studies including a larger number of subjects as in the present investigation.
There is increasing evidence of substantial benefits of immunomodulating drugs including colchicine or canakinumab for patients after MI [1, 3], while treatment selection was based on systemic biomarkers of inflammation including CRP [3]. While these studies aimed to reduce future vascular events, no specific biomarker is available for identifying patients that might benefit from immunological therapy to improve myocardial function. The observed value of the splenic PET signal for identifying patients predisposed to functional recovery and previous results on CXCR4 expression in the infarct territory for MACE prediction may open avenues for guiding cardiac repair by non-invasive molecular imaging [13]. For instance, recent years have witnessed an increased use of highly specific, targeted drugs such as in-vivo re-programmed chimeric antigen receptor (CAR) T-cells to enhance cardiac repair, which also accumulate in the spleen to provide a target antigen reservoir [20]. Those highly costly targeted interventions necessitate novel approaches for identifying subsets of patients that will most likely benefit from treatment, preferably by providing information on a (sub)cellular level about the absence or presence of the drug target in the myocardium or distant organs, e.g., target antigens in the spleen. Molecular imaging has multiple advantages relative to biopsies that are prone to sampling errors or blood-based systemic biomarkers which cannot provide segregated information on a local cardiac tissue level or on remote lymphatic organs [6]. Relative to morphological imaging, PET can also determine the extent of the underlying pathophysiology, while CMR primarily focus on functional parameters [5]. Nonetheless, in the present study, CMR-derived baseline LVEF and the splenic PET signal were relevant outcome predictors for functional recovery, thereby highlighting the importance of simultaneous assessments of morphological and molecular information for precisely identifying patients with best outcome. Thus, combined devices such as PET/MRI may therefore allow to determine those relevant parameters in a “one-stop-shop” setting, thereby facilitating a broader clinical use of the herein derived findings [21].
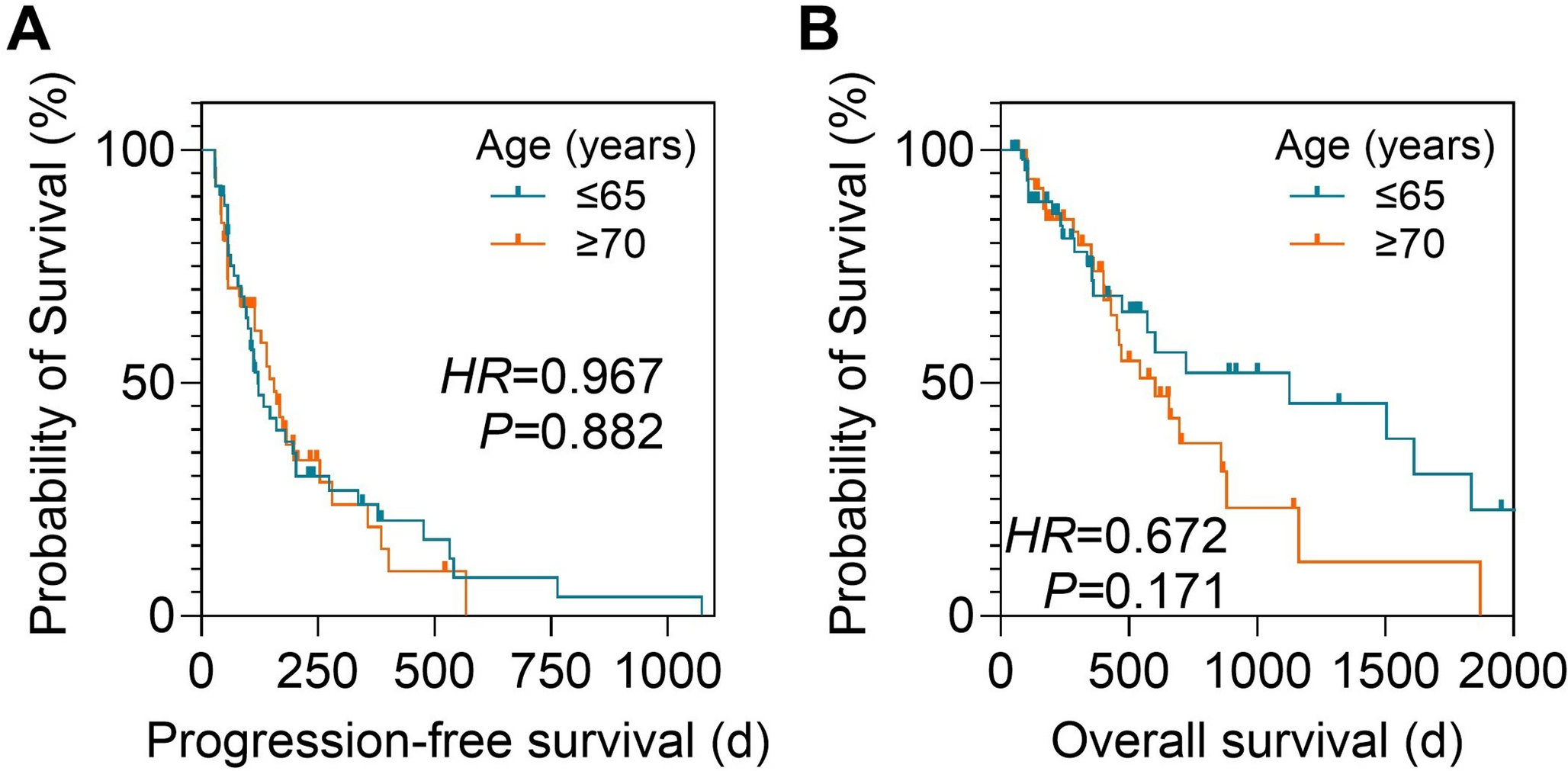
Our study has several limitations, including its moderately impaired cardiac function at baseline. However, in the present prospective trial, we still observed substantially decreased LVEF with a lower range of 34%. In this regard, imaging and therapeutic protocols including timely reperfusion therapies have been strictly followed, thereby presenting a cohort reflecting clinical reality along with standardized functional re-assessments at two fixed FU time-points. Such fixed re-examinations, however, do not allow for time-to-event analyses, such as Kaplan-Meier analysis. We acknowledge that the sample size at the 12‑month follow‑up (n = 36) is relatively small. However, the attrition rate of only 12.2% is low for a longitudinal clinical study [22] and suggests a homogeneous and stable cohort. This low loss to follow‑up may reduce the risk of attrition bias and may support the robustness of the observed effects. Nonetheless, our preliminary findings should be re-evaluated in a larger multicenter setting. Moreover, due to logistic reasons including synthesis procedures and tracer availability, it was not feasible to conduct CXCR4 PET scans on the same day for every patient, while the respective group sizes were still balanced (early, 56.1% vs. late PET imaging, 43.9%). However, to further address timing of PET, we also adjusted for scan timing without significant results in univariate analyses. Given the fact that chemokine receptors are overexpressed on a broad range of leukocytes, which are fluctuating over time early after AMI [23], it cannot be ruled out that such temporal dynamics may also interfere with severity of the PET signal conducted at different time-points, thereby explaining the missing predictive potential for uptake in the infarct region in our patient population. Nonetheless, unlike in previous investigations [12, 13], the aim of the present prospective study was not to assess the predictive value of the infarct territory, but focused on extra-cardiac organs involved in the immune response imaged with chemokine receptor PET. In this regard, we added to the literature by demonstrating that read-out of LN and splenic uptake within a time window of up to 8 days after AMI can identify patients prone to cardiac functional changes. Future work should also re-assess the predictive value of PET for occurrence of MACE in a prospective setting, thereby providing further clinical value beyond LVEF outcome prediction [13].

Comments (0)