
Remember me
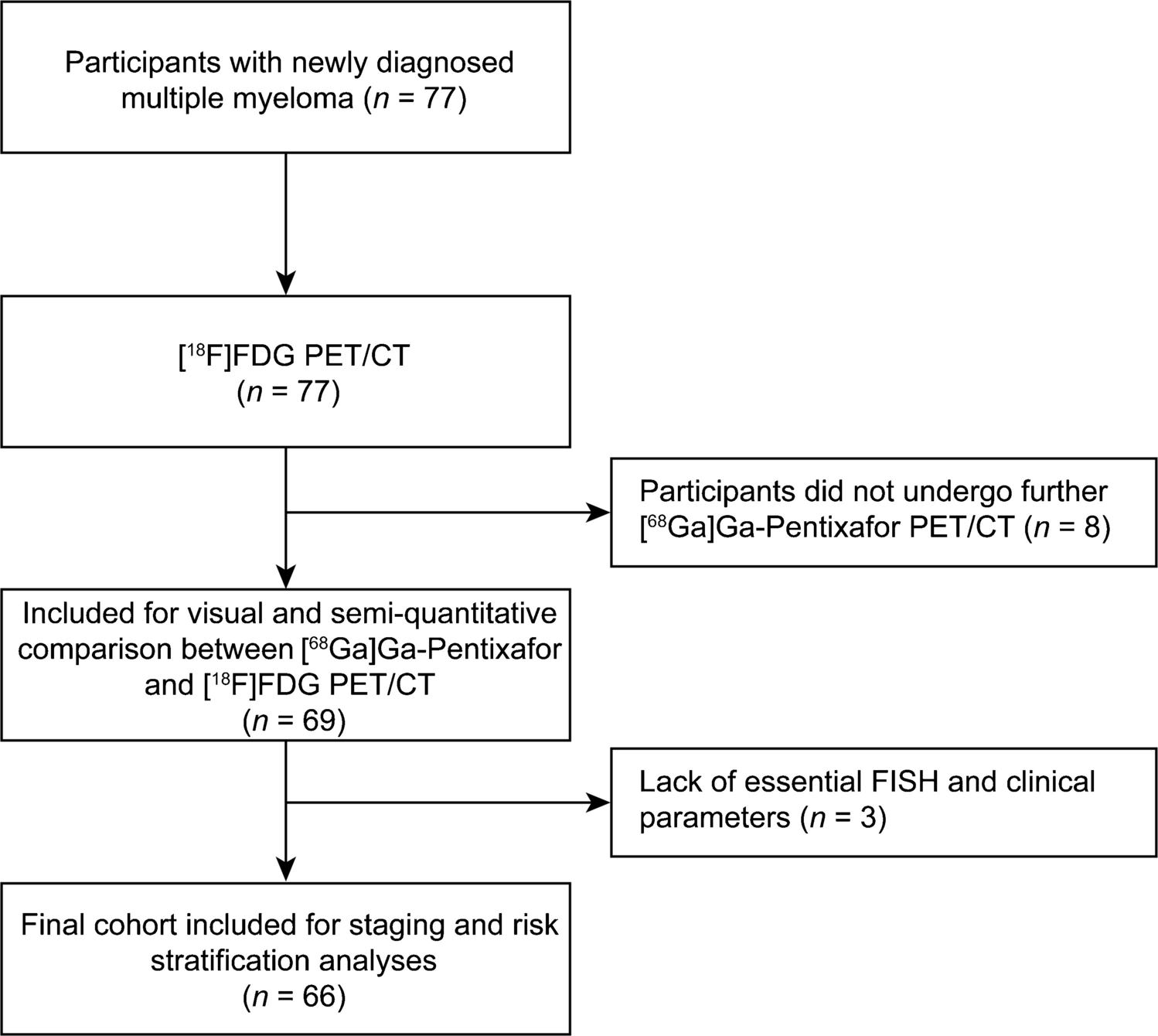
A total of 147 patients with PSA persistence following radical prostatectomy were included in this retrospective analysis. The final cohort was clearly delineated into the Staging Cohort (n = 72, 49%), who received pre-operative [68Ga]Ga-PSMA-11 PET/CT, and the Non-Staging Cohort (n = 75, 51%), who did not (Table 1). The absence of pre-operative PSMA PET in the Non-Staging Cohort was attributed to two primary factors: its non-indication based on standard guidelines at the time of initial diagnosis for patients classified as favorable-intermediate risk, or logistical barriers, including limited local availability. Pre-operative Multiparametric Prostate Magnetic Resonance Imaging (mpMRI) data were analyzed for 99 patients (67% of the total cohort). This analysis found no statistically significant difference in high-risk PIRADS scores (4/5) between the Staging and Non-Staging Cohorts (p = 0.291). Initial staging in the Non-Staging Cohort (n = 75) relied exclusively on conventional imaging. Specifically, 56 patients (75%) underwent a pre-operative BS, and 69 patients (92%) underwent a pre-operative CT scan, and 51 patients (68%) received both BS and CT scan. All bone scans were negative for metastasis. The analysis of cTNM data derived from CT, highlighted locally advanced disease (cT3a/b) in 28 (31%) of cases, with only 2 patients (3%) classified as cN1 (Table 2). Conversely, the Staging Cohort primarily used [68Ga]Ga-PSMA-11 PET/CT, with only a small minority utilizing also conventional imaging (n = 4, 6% both BS and CT scan). The median administered activity of [68Ga]Ga-PSMA-11 was 145Mbq (IQR 134–153) with a standard uptake time of 64 min (IQR 60 -72.5).
Table 1 Baseline Patient and Tumor CharacteristicsAs detailed in Table 1, demographic and temporal characteristics, such as median age and time elapsed from RP to the PSMA PET for persistence, showed no significant differences between the two cohorts (p > 0.05). However, a significant disparity in initial risk profiles was evident, reflective of the clinical selection criteria for advanced imaging. The Staging Cohort showed a significantly higher proportion of adverse pathological features: 52 patients (72%) were classified as high-grade (ISUP 4 or 5) compared to 34 patients (45%) in the Non-Staging Cohort (p < 0.05). Similarly, the extent of local disease was greater in the Staging Cohort, with 56 patients (78%) classified as T3a/T3b/T4, versus 46 patients (61%) in the Non-Staging Cohort (p < 0.05).
PSMA PET positivity and extent of disease at persistenceOverall, the [68Ga]Ga-PSMA-11 PET/CT scan performed for PSA persistence demonstrated positive findings in 74 patients (50%) across the entire cohort. The Non-Staging Cohort yielded a significantly higher rate of positive PSMA PET/CT scans for persistence (44/75, 59%) compared to the Staging Cohort (30/72, 42%; p < 0.05).
To account for the influence of tumor stage on outcomes, a subgroup analysis was performed restricted to patients with locally advanced disease (pT3/pT4). In the Non-Staging Cohort, 27 out of 46 patients (59%) with pT3/pT4 disease had a positive PET, compared to 24 out of 56 patients (43%) in the Staging Cohort. Despite both cohorts sharing this same high-risk pathological stage, the rate of PET positivity for persistence differed, although this difference did not reach statistical significance (p = 0.16).
Table 2 Conventional Staging Modalities and Findings in the Non-Staging CohortThe higher positivity translated to a greater extent of aggressive disease in the Non-Staging Cohort. Findings consistent with M1 disease (bone, visceral, common iliac, or extra-pelvic nodes) were identified in 34 patients (45%) of the Non-Staging Cohort, substantially exceeding the 21% (15 patients) found in the Staging Cohort. Overall, positive lymph node findings were observed in 55 patients (37%), with the Non-Staging Cohort having a higher absolute rate (34/75, 45%) compared to the Staging Cohort (21/72, 29%).
Analysis of the anatomical distribution of positive lymph node sites further highlighted the difference in disease extent. While the Staging Cohort showed a higher proportion of positive sites in obturator nodes (48% of positive sites), suggesting more contained regional failure, the Non-Staging Cohort exhibited a significantly higher burden of advanced nodal involvement, including common iliac (34%) and external/internal iliac sites. Bone findings were observed in 32 patients (22%) across both cohorts, and visceral lesions in 2 patients (1%) (Table 3; Figs. 1 and 2).
Table 3 PSMA PET Findings for PSA PersistenceFig. 1
Nodal Distribution of PSA Persistence: Staged vs. Non-Staged Cohorts. This bubble plot compares the nodal distribution of PSA persistence across different lymph node locations between the Non-PET Cohort (red circles) and the PET Cohort (blue circles). The x-axis shows the Relative Frequency of Positive Sites (%) for each location within the respective cohort. The Frequency (%) of involvement for a specific lymph node site is represented by the size of the bubble
Fig. 2
Anatomical schematic illustrating the Nodal Distribution of PSA Persistence: PET vs. Non-PET Cohorts. A schematic anatomical overlay showing the relative frequency and distribution of positive lymph node sites for the Non-PET Cohort (red circles) and the PET Cohort (blue circles). The size of the bubble indicates the Frequency (%) of involvement for that specific lymph node location, as shown in the legend. This schematic highlights the difference in common metastatic sites between the two staging strategies
Subgroup analysis and clinical impactAmong the Non Staging cohort, 15/75 patients (20%) were low and favorable-intermediate risk PCa (ISUP 1–2), for whom pre-operative PSMA PET is not indicated based on current guidelines. Among this group, 4 out of 15 patients (27%) were found to have positive [68Ga]Ga-PSMA-11 PET/CT findings for persistence, totaling 7 lesions. All 4 patients had previously undergone both a pre-operative BS and a CT scan for initial staging. Notably, 3 out of 7 lesions were classified as M1 disease, specifically: 1 bone lesion in the left iliac wing and 2 common iliac lymph nodes. The remaining 4 lesions included 2 para-rectal, 1 obturator node and 1 external iliac lymph node. All these lesions were not detectable (bone) or interpreted as benign (sub centimetric lymph nodes) at conventional imaging.
The clinical consequence of the diagnostic gap was demonstrated through a retrospective evaluation of the Non-Staging Cohort. A pre-operative PSMA PET/CT would have triggered a “theoretical change of management” in all 44 cases with a positive scan. Based on the positive findings, 34 patients (77% of positive cases) would have been immediate candidates for systemic therapy due to M1 disease (common iliac lymph node involvement: n = 12, 27% ; extra-pelvic lymph node involvement: n = 5, 11% ; and bone involvement: n = 17, 39%). The remaining 10 patients (23% of positive cases) with only pelvic lymph node involvement would have been candidates for extended lymphadenectomy or primary radiotherapy, representing a change in local management strategy (Figure 3).
Fig. 3
Theoretical Change of initial therapeutic management in the Non-Staging Cohort (n = 75) guided by [68Ga]Ga-PSMA-11 PET/CT findings. The Sankey diagram illustrates the proposed triage of patients in the Non-Staging Cohort based on the findings of the [68Ga]Ga-PSMA-11 PET/CT performed for PSA persistence. The width of the bands is proportional to the patient count (n = 75), demonstrating the profound clinical shift that molecular imaging would have enabled. The single node on the left represents the uniform actual treatment pathway received by all 75 patients (RP or primary RT) without PSMA PET/CT guidance. The nodes on the right represent the optimal, individualized pathways that would have been chosen had PSMA PET/CT findings been available pre-treatment. The flow reveals that 44 patients (59% of the cohort) should have been diverted to a different management strategy. Specifically, the 34 patients (77\% of the positives, shown in red) with M1 disease (osseous or common iliac lymph nodes) would have been managed with immediate Systemic Treatment, thereby avoiding inappropriate local therapy. The 10 patients (shown in blue) with locoregional disease would have prompted a change to Intensified Local Treatment (eLND or SBRT). Only the 31 patients with PSMA PET/CT-negative scans would have optimally remained on the initial RP or Primary RT pathway (shown in gray)
Comments (0)