
Remember me
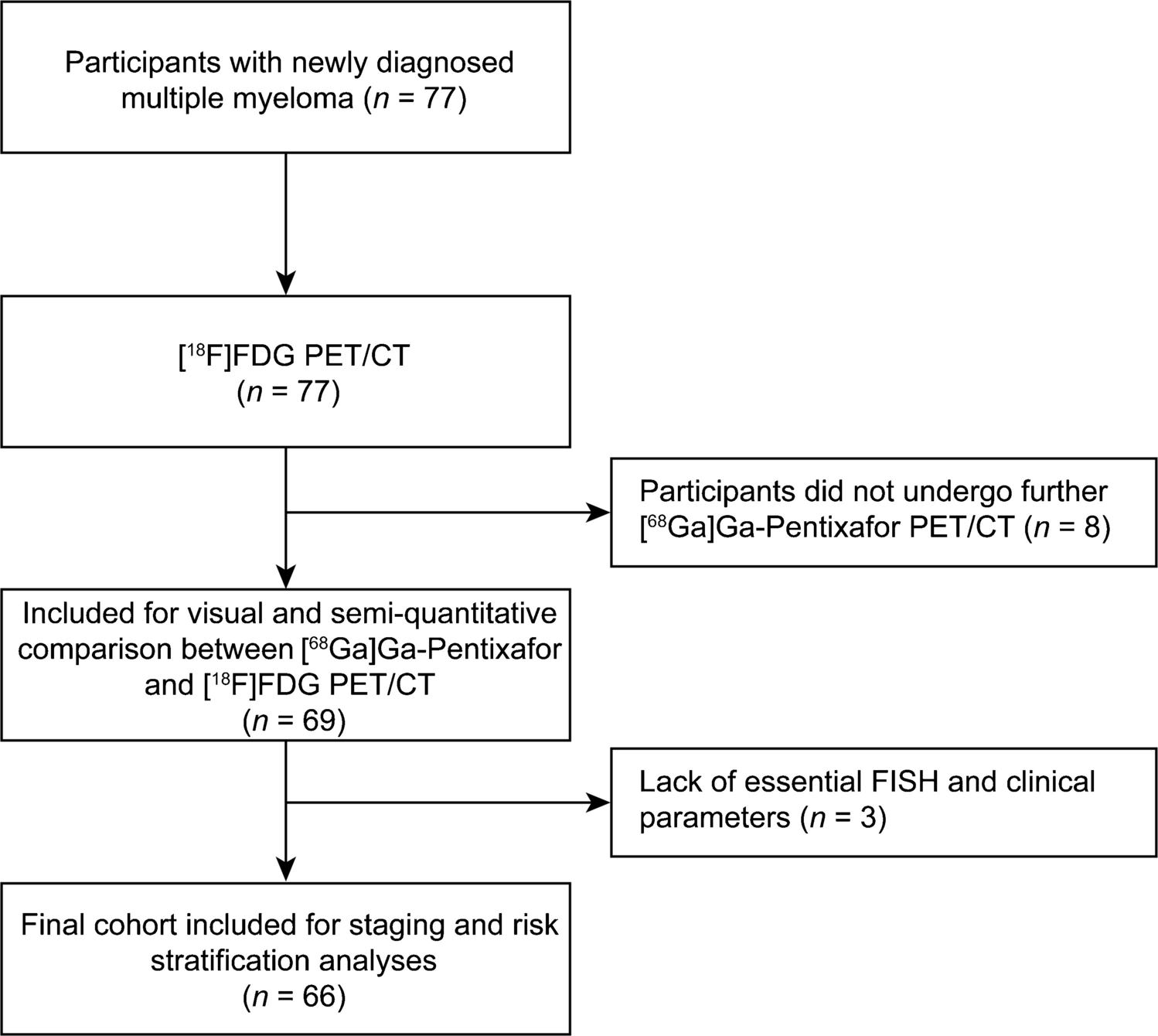
Data for 98 eligible patients was screened for completeness, and a total of 94 patients were available for analysis in the MPI cohort. Four patients were missing either PET (n = 3) or follow up data.
Results 1 : baseline characteristics, survival outcomes and cohort comparisonBaseline characteristics were compared between the MPI cohort and the non-MPI cohort from the CONVERT trial (n = 449). Table 1 summarises the baseline demographic, clinical, and treatment characteristics of both cohorts.
Table 1 Baseline demographic, clinical, and treatment characteristics of patients who underwent multiparametric imaging (MPI) compared with the non-MPI cohort from the CONVERT trial. Continuous variables are reported as median (range) and compared using the Wilcoxon rank-sum test. Categorical variables are reported as counts (percentages) and compared using the chi-squared testPatients who underwent MPI had a significantly different tumour stage distribution compared with the non-MPI cohort (AJCC stages I–II: 25% vs. 14%; AJCC stage III: 70% vs. 80%; p = 0.012). The MPI cohort also had a smaller gross tumour volume (48.7 cm³ [range 2.2–593] vs. 92.9 cm³ [0.5–635.1]; p < 0.001), were less likely to have a pre-treatment LDH level above the upper limit of normal (12% vs. 26%; p < 0.001), and a smaller proportion received six, as opposed to four, planned chemotherapy cycles (14% vs. 36%; p < 0.001).
Median follow-up was not significantly different between the groups (4.2 years for MPI vs. 5.9 years for non-MPI; p = 0.43). Median overall survival was also not significantly different (1.7 years for MPI vs. 2.4 years for non-MPI; p = 0.37), and there was no significant difference in progression-free survival between cohorts (Supplementary Fig. 4.1).
Results 2 : univariable prognostic analyses (linear and non-linear)Linear univariable Cox regressionResults of univariable Cox regression analyses for overall survival are shown in Table 2. The CPM score demonstrated a strong association with overall survival (HR 3.54, 95% CI 1.53–8.20; p = 0.003). Larger CT-based gross tumour volume was also associated with worse overall survival (HR 1.28, 95% CI 1.05–1.57; p = 0.017).
Table 2 Univariable Cox proportional hazards analyses of clinical, CT-based, and PET-derived parameters for overall survival in the MPI cohort. Volume-related imaging parameters were log₂-transformed and are expressed as hazard ratios per doubling. Non-PET parameters are shown in italicsAmong PET-derived whole-body metrics, measures of tumour burden showed the strongest associations with outcome. Whole-body total lesion glycolysis was significantly associated with overall survival (HR 1.17, 95% CI 1.00–1.37; p = 0.048), while whole-body metabolic tumour volume showed a borderline association (HR 1.19, 95% CI 1.00–1.42; p = 0.057). No statistically significant associations were observed between overall survival and SUV-based metrics or texture- and shape-derived PET features.
Univariable Cox regression analyses for progression-free survival are presented in Supplementary Table 5.1. Similar to overall survival, CPM, CT-based gross tumour volume, whole-body metabolic tumour volume, and whole-body total lesion glycolysis were associated with shorter progression-free survival, whereas SUV-based metrics and radiomic heterogeneity features were not.
Spline-based univariable analysesSpline-based analyses were performed to explore the form of the association between imaging variables and survival. Penalised smoothing spline plots for overall survival are shown in Fig. 1, with corresponding analyses for progression-free survival shown in Supplementary Fig. 5.1.
Fig. 1
Non-linear associations between selected CT- and PET-derived imaging parameters and (A) overall survival and (B) progression-free survival, modelled using penalised smoothing splines. Solid lines represent estimated log hazard ratios relative to the median predictor value, with shaded areas indicating 95% confidence intervals. P-values reflect the overall association from likelihood ratio testing
Across CT-based and PET-derived tumour burden metrics, spline curves demonstrated broadly monotonic relationships, with no clear evidence of any non-linear relationships. Overall spline term p-values did not reach statistical significance for any variable (Supplementary Table 5.2). Borderline overall associations were observed for whole-body metabolic tumour volume (overall survival p = 0.059; progression-free survival p = 0.112) and whole-body total lesion glycolysis (overall survival p = 0.071; progression-free survival p = 0.087).
Results 3 : multivariable analysesClinical-only multivariable Cox models were first examined to assess the independent prognostic contribution of standard clinical factors within the MPI cohort (n = 88; six patients missing clinical data). Variates included age, sex, smoking status, ECOG performance status, LDH, number of chemotherapy cycles, and radiotherapy dose (Supplementary Table 6.1 and 6.2). In these models, individual clinical covariates did not demonstrate strong or consistent independent associations with overall survival. For progression-free survival, smoking status was associated with outcome, with both current smokers (HR 0.15, 95% CI 0.03–0.72; p = 0.019) and former smokers (HR 0.10, 95% CI 0.02–0.50; p = 0.005) demonstrating lower hazard ratios compared with never-smokers (Supplementary Table 6.2).
Based on univariable analyses, CT-based gross tumour volume and PET-derived whole-body metabolic tumour volume and total lesion glycolysis were taken forward for multivariable imaging analyses. To avoid collinearity, imaging variables were entered individually alongside the clinical covariates. Results of these models are summarised in Table 3.
Table 3 Multivariable Cox proportional hazards models evaluating the association between tumour burden metrics and survival after adjustment for pre-specified clinical covariates (age, sex, smoking status, ECOG performance status, LDH, number of chemotherapy cycles, and radiotherapy dose). Imaging parameters were entered individually to minimise collinearity. Hazard ratios for imaging variables are expressed per doubling following log₂ transformation. Model discrimination is reported using harrell’s concordance index (C-index)After clinical adjustment, CT-based gross tumour volume remained independently associated with both overall survival (HR 1.36, 95% CI 1.06–1.74; p = 0.016) and progression-free survival (HR 1.29, 95% CI 1.03–1.63; p = 0.029). In contrast, PET-derived whole-body metabolic tumour volume and total lesion glycolysis were not independently associated with either endpoint after adjustment, with effect estimates attenuated and no longer statistically significant.
Results 4 : incremental prognostic value of PET metrics beyond CPMThe CPM is a pre-specified clinical nomogram, and PET-derived SUV metrics (SUVmean, SUVpeak, and SUVmax) were added individually to the CPM to assess their impact on model discrimination.
For overall survival, the C-index of the CPM alone was 0.63. The addition of SUVmean, SUVpeak, or SUVmax did not improve model discrimination, with C-indices remaining at 0.63 in all models (ΔC − 0.001, − 0.006, and 0.000, respectively; Table 4). The 95% confidence intervals for the change in C-index crossed zero for all comparisons.
Table 4 Comparison of model discrimination for CPM alone versus CPM plus individual PET-derived SUV metrics (SUVmean, SUVpeak, SUVmax) for overall and progression-free survival. Discrimination was assessed using harrell’s concordance index (C-index). ΔC represents the change in C-index relative to CPM alone. Ninety-five per cent confidence intervals were derived using bootstrap resampling (1,000 iterations)Similar findings were observed for progression-free survival. The C-index for the CPM alone was 0.59, and the addition of SUVmean, SUVpeak, or SUVmax resulted in minimal changes in discrimination (C-indices 0.59–0.60), with ΔC values of − 0.001, − 0.004, and 0.002, respectively. Confidence intervals for all ΔC estimates crossed zero (Table 4).
Results 5: correlation between study variablesCorrelations between PET-derived whole-body metrics, CT-based gross tumour volume, CPM, and circulating tumour cells were assessed using Spearman correlation analysis. Pairwise correlations across all variables are shown in Fig. 2, with CPM-specific correlation coefficients reported in Supplementary Table 7.1.
Fig. 2
Spearman correlation heatmap showing relationships between PET-derived whole-body imaging features, CT-based gross tumour volume, the clinical prognostic model (CPM), and circulating tumour cell counts. Colour intensity represents the magnitude and direction of correlation (blue, negative; red, positive). Variables are hierarchically clustered to highlight patterns of similarity. Circulating tumour cell counts showed no significant correlations with imaging-derived or clinical variables
CT-based gross tumour volume and PET-derived measures of whole-body tumour burden demonstrated strong correlations with the CPM score, including whole-body metabolic tumour volume (ρ = 0.729, p < 0.001), total lesion glycolysis (ρ = 0.711, p < 0.001), and total tumour voxel count (ρ = 0.699, p < 0.001). SUV-based PET metrics showed more modest correlations with CPM, including SUVpeak (ρ = 0.342, p = 0.003), SUVmean (ρ = 0.307, p = 0.008), and SUVmax (ρ = 0.297, p = 0.011). Correlations between CPM and SUV-derived measures of uptake variability were weak and not statistically significant.
Across the full correlation matrix (Fig. 2), texture- and shape-derived PET features demonstrated low correlations with CT-based gross tumour volume, CPM, and SUV-based metrics. Circulating tumour cell counts were available in a limited subset of patients (n = 32), and no significant correlations were observed between CTC and PET-derived whole-body metrics, CT-based gross tumour volume, or CPM.
Comments (0)