
Remember me
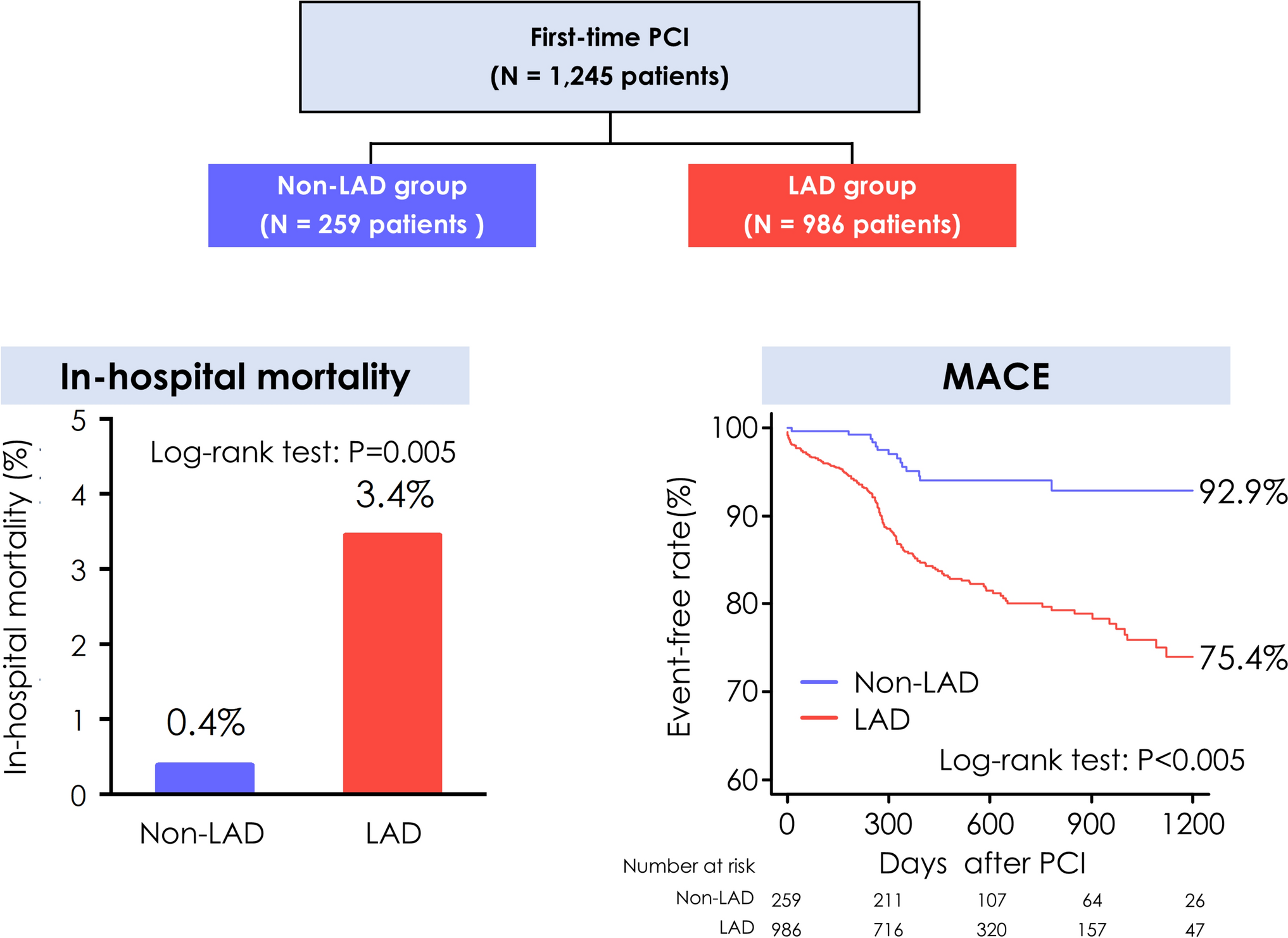
The patient flowchart is shown in Fig. 1. Ultimately, 1,245 patients who underwent PCI for the first time were analyzed. Of these, 986 (79.2%) had LAD lesions, and 259 (20.8%) did not. The median follow-up period was 514 days (IQR: 330–789). Angiographic follow-up was performed in 511 patients (41.0% of the total population) 9–12 months after the index PCI.
Baseline profilesThe clinical profiles of the patients are shown in Table 1. The average age of the study population was 67 years, and 75% of the patients were males. Regarding CV risk factors, the prevalence of dyslipidemia, diabetes, and chronic kidney disease was significantly higher in the LAD group than in the non-LAD group. Mean LVEF was significantly lower in the LAD group. Regarding the clinical presentation of CAD, the distributions of ACS, STEMI, and prior MI were comparable between the two groups. Differences in laboratory data were observed for eGFR and HbA1c levels. HbA1c was analyzed separately in diabetic and non-diabetic patients, showing a significant difference only among diabetic patients.
Table 1 Baseline profilesThe angiographic and procedural parameters during PCI are shown in Table 2. In the LAD group, 100%, 6.3%, 19.6%, and 22.8% of the patients underwent PCI for the LAD, LMCA, left circumflex artery (LCx), and right coronary artery (RCA), respectively, including both primary and staged procedures. In the non-LAD group, 41.3% of the patients underwent PCI for the LCx and 73.0% for the RCA. Patients in the LAD group had significantly higher rates of multivessel disease, calcified lesions, and long lesions than those in the non-LAD group. Compared with the non-LAD group, the LAD group had a significantly smaller median stent diameter (3.0 [IQR: 2.5–3.5] vs. 3.0 [2.75–3.5] mm, p < 0.001), a longer median stent length (28 [18–35] vs. 23 [16–32] mm, p < 0.001), and a higher distribution of the total number of stents per patient (median 1 [1–2] vs. 1 [1–2], p < 0.001). There was no significant difference in the success rate of the first PCI between the two groups.
Table 2 Procedural characteristicsIn-hospital and long-term prognosisThe in-hospital mortality was significantly higher in the LAD group than in the non-LAD group (3.4% vs. 0.4%; p = 0.005) (Graphical Abstract). Kaplan–Meier analysis demonstrated significantly higher 2-year estimated rates of MACE, CV death, TVR, and all-cause death in the LAD group than in the non-LAD group (MACE: 19.9% vs. 6.0%, p < 0.001; CV death: 3.5% vs. 0.4%, p = 0.004; TVR: 17.0% vs. 5.6%, p < 0.001; all-cause death: 7.6% vs. 3.7%, p = 0.006 (Graphical Abstract, Fig. 2, and Table 3).
Fig. 2
Prognostic comparisons after PCI between patients with and without LAD lesions. Comparison of MACE, CV death, TVR, nonfatal MI, and all-cause death between patients with and without LAD lesions. CV, cardiovascular; LAD, left anterior descending artery; MACE, major adverse cardiovascular event; MI, myocardial infarction; PCI, percutaneous coronary intervention; TVR, target vessel revascularization
Table 3 Clinical outcomes according to the presence of LAD lesions (Kaplan–Meier 2-year estimates)Furthermore, the multivariable analysis confirmed LAD lesions as independent predictors of MACE (hazard ratio (HR): 2.42, 95% confidence interval (CI): 1.28–4.58), along with comorbid diabetes (HR: 1.62, 95% CI: 1.10–2.38), low LVEF (HR: 1.80, 95% CI: 1.18–2.73), and coronary calcification (HR: 2.26, 95% CI: 1.56–3.27; Table 4).
Table 4 Cox regression model for the major adverse cardiovascular eventsTo address potential bias from the high proportion of hemodialysis patients in our cohort, we conducted a sensitivity analysis excluding these individuals. The findings remained robust: the LAD group still exhibited significantly higher rates of MACE (p < 0.001), CV death (p = 0.011), TVR (p < 0.001), and all-cause mortality (p = 0.005). However, the difference in nonfatal MI (p = 0.122) between groups remained non-significant (Supplemental Fig. 1).
Sensitivity analysis stratified by LAD single-vessel and LAD multivessel diseaseWe conducted a sensitivity analysis stratifying patients into Non-LAD, LAD (Only), and LAD (Multivessel) groups (Supplemental Fig. 2). Kaplan–Meier analysis showed significant differences in MACE, CV death, TVR, and all-cause death (all p < 0.001), but not in nonfatal MI (p = 0.100). For MACE and TVR, outcomes worsened progressively from Non-LAD to LAD (Only) to LAD (Multivessel). CV death and all-cause death were significantly higher in LAD (Multivessel) compared to both other groups, while Non-LAD and LAD (Only) did not differ significantly.
ACS vs. Non-ACSConsidering the clinical presentation of ACS and CCS (Supplemental Fig. 3), the in-hospital mortality was significantly higher in patients in the LAD group with ACS (n = 387, 6.2%) than in those in (i) the LAD group with CCS (n = 599, 1.7%), (ii) non-LAD group with ACS (n = 89, 0%), and (iii) non-LAD group with CCS (n = 170, 0.6%) (LAD group with ACS vs. LAD group with CCS, p < 0.001; Supplemental Fig. 4). However, the presence or absence of ACS did not make a statistically significant difference in long-term all-cause death, MACE, TVR, or nonfatal MI in the LAD or non-LAD groups (Supplemental Fig. 4). In contrast, ACS only affected CV death in patients with LAD lesions (LAD group with ACS vs. LAD group with CCS, p = 0.042; non-LAD group with ACS vs. non-LAD group with CCS, p = 0.47; Supplemental Fig. 4).
Impact of LMCATo account for the potential confounding effect of LMCA lesions in the LAD group, this study compared short- and long-term outcomes between the LAD group with LMCA lesions, the LAD group without LMCA lesions, and the non-LAD group. The in-hospital mortality rate was higher in patients in the LAD group with LMCA lesions (7.1%) compared to those in the LAD group without LMCA lesions (3.0%) and the non-LAD group (0.4%) (LAD group with LMCA vs. LAD group without LMCA, p = 0.001). However, for the long-term prognosis, there were no significant differences in the rates of MACE, CV death, TVR, nonfatal MI, or all-cause death between patients in the LAD groups with and without LMCA lesions (Supplemental Fig. 5).
Comments (0)