
Remember me
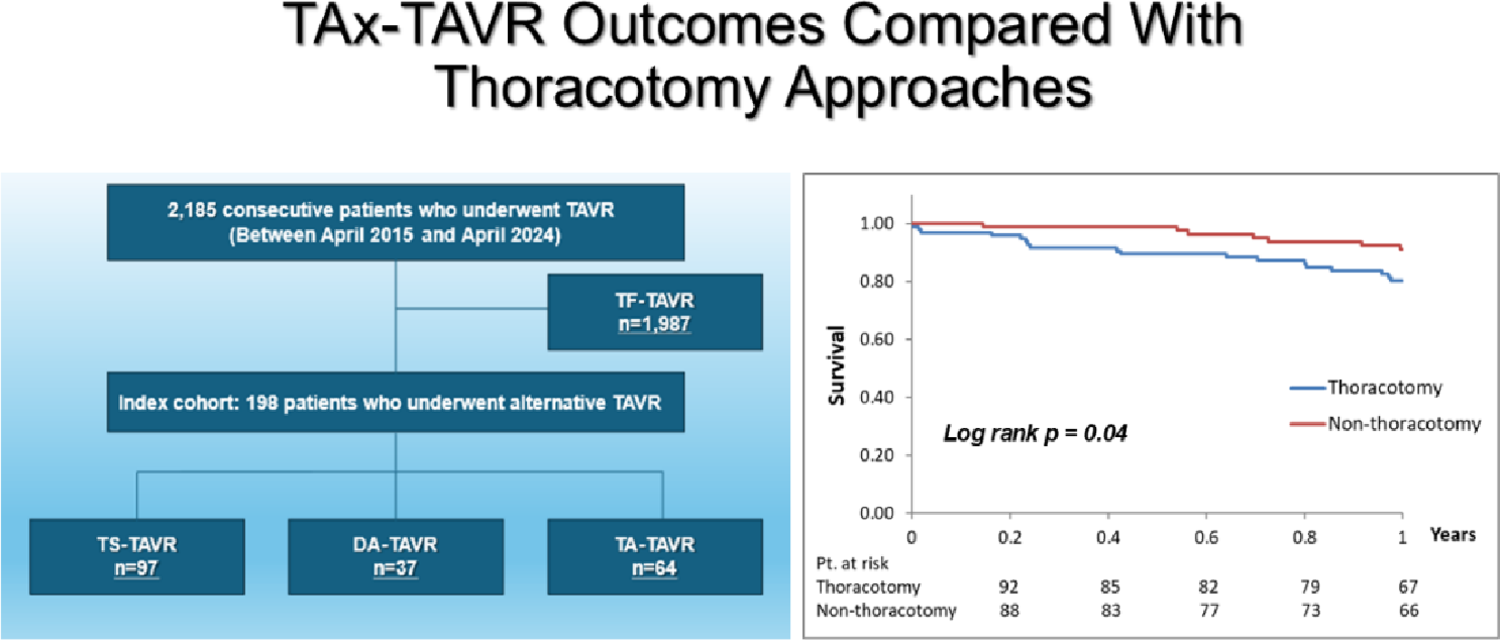
In this study, we compared the perioperative and mid-term outcomes of TAx-TAVR (non-thoracotomy approach) with those of TA and DA-TAVR (thoracotomy approaches) performed as alternative access routes. The thoracotomy group showed a higher tendency toward in-hospital mortality. Most deaths were attributed to pneumonia, which may be associated with impaired respiratory function due to thoracotomy and general anesthesia, as well as delayed postoperative recovery. This difference in early mortality was reflected in the significantly lower 1-year survival rate in the thoracotomy group, underscoring the advantage of the TAx-TAVR. These results suggest that TAx-TAVR is a reasonable and less invasive alternative access option for patients in whom TF-TAVR is not feasible. Consistent with previous reports, TAx-TAVR in our cohort was associated with shorter operative time and reduced length of hospital stay, indicating lower procedural burden for patients [4,5,6].
On the other hand, although not statistically significant, postoperative ischemic stroke tended to occur more frequently in the TAx-TAVR group. This finding is consistent with previous studies [7, 8]. One potential explanation is that delivery systems introduced via the subclavian artery may come into contact with atherosclerotic plaques in the aortic arch, increasing the risk of embolic debris dislodgement. Vertebral artery occlusion may also lead to posterior circulation ischemic stroke [9]. In addition, the more frequent use of self-expandable valves in TAx-TAVR may increase embolic risk due to the characteristics of the deployment process [10]. In the present study, ischemic stroke occurred in one patient who underwent DA-TAVR and in five patients who underwent TAx-TAVR. In the DA-TAVR case, severe bilateral carotid artery stenosis had been identified preoperatively, which was considered a possible cause of the ischemic stroke. In contrast, among the TAx-TAVR cases, two patients had atherosclerotic plaques in the aortic arch, one patient had protruding calcification into the lumen of the ascending aorta, one patient developed postoperative Stanford type A aortic dissection, and one patient had severe calcification of the aortic valve.
These findings suggest that the mechanisms underlying ischemic stroke after TAx-TAVR are not uniform but rather multifactorial, involving aortic arch atheroma, extensive calcification of the ascending aorta and annulus, and postoperative complications, with different contributing factors in individual cases. Indeed, no clear causal relationship was observed between stroke occurrence and dominance of the access-side vertebral artery in this study. Therefore, when considering TAx-TAVR, comprehensive vascular assessment is essential, including not only laterality of vertebral artery dominance but also evaluation of aortic arch atheroma and calcification of the ascending aorta and aortic valve. Moreover, in the present study, three cases of intimal injury requiring repair and two cases of aortic dissection occurred in the TAx-TAVR, raising concern that the mismatch between vascular diameter and the delivery system may increase vascular stress. In particular, for patients with a minimal subclavian artery diameter < 5.5 mm, alternative access routes may need to be considered.
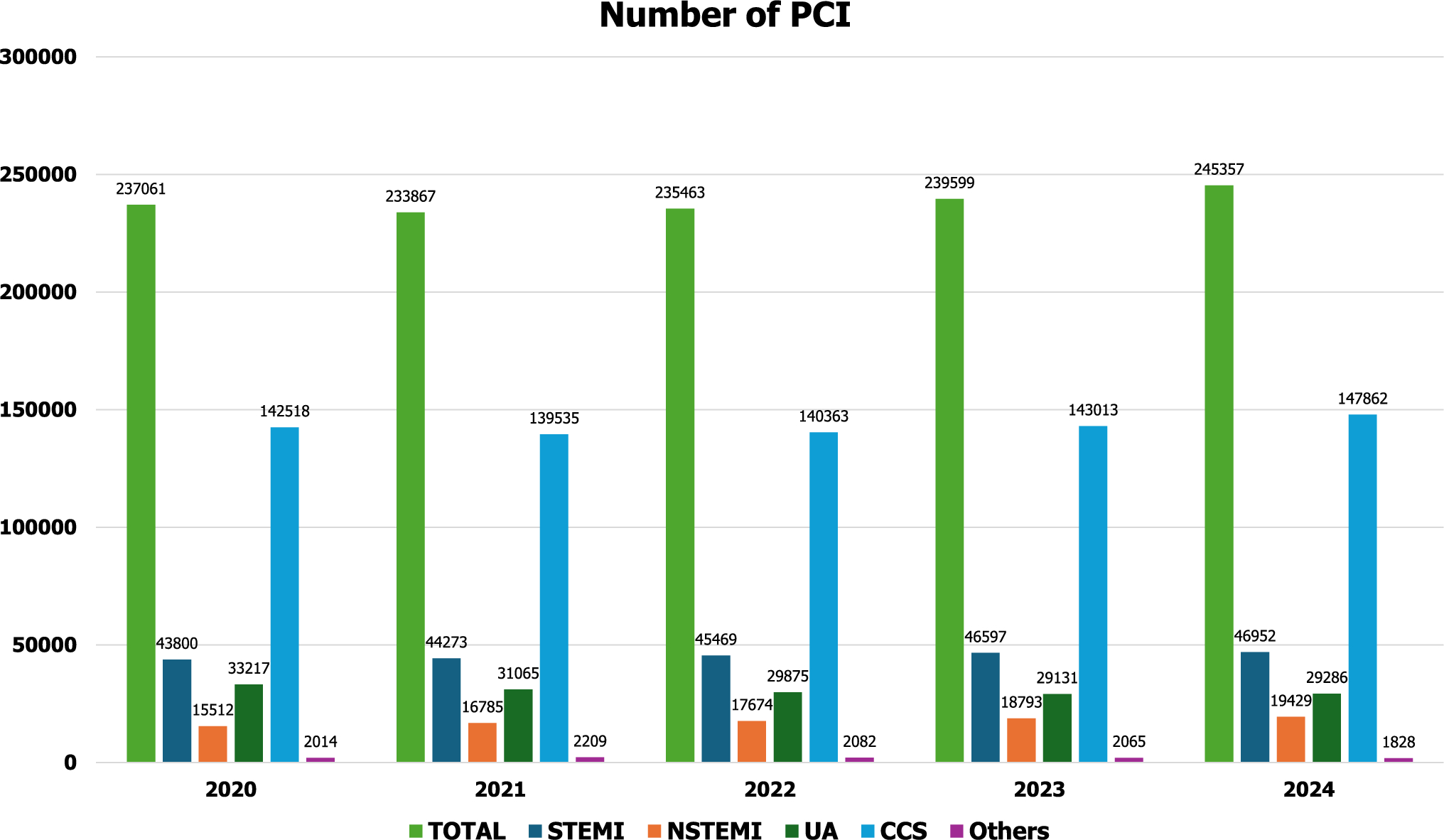
In Japan, CoreValve (Medtronic Inc., MN, USA) was approved for TAx-TAVR in 2015, and our institution performed its first TAx-TAVR in 2016. Subsequently, with the approval of SAPIEN 3 (Edwards Lifesciences Ltd., Irvine, CA, USA) for TAx-TAVR and for use in dialysis patients in 2021, both the absolute number and proportion of TAx-TAVR procedures have shown a clear increasing trend (Fig. 3). This is likely due to the high prevalence of severe peripheral arterial calcification in dialysis patients, making TF-TAVR anatomically unsuitable in many cases. Given the relatively high proportion of dialysis patients in Japan, the demand for alternative access routes is expected to continue increasing nationwide.
Fig. 3
Number of cases in which the thoracotomy and non-thoracotomy approaches were used each year. In 2013, the Sapien XT (Edwards Lifesciences Ltd, Irvine, CA, USA) received regulatory approval for TF and TA-TAVR. Subsequently, in 2015, the CoreValve (Medtronic Inc., MN, USA) was approved for TF, DA, and TS-TAVR. Our institution performed its first TS-TAVR in 2017. Additionally, since SAPIEN 3 (Edwards Lifesciences Ltd, Irvine, CA, USA) received regulatory approval for TS-TAVR and use in dialysis patients in 2021, the overall number of TAVR procedures, as well as in the absolute number and proportion of TS-TAVR, have shown an increasing trend
Among alternative access options, the transcarotid (TC) approach has recently gained attention. TC-TAVR offers a favorable trajectory to the aortic annulus and may be associated with a lower risk of embolic events [11, 12], and accumulating evidence regarding long-term outcomes and cerebrovascular events is anticipated.
LimitationsThis study has several limitations. First, it was a retrospective observational study, and the choice of access route depended on the operator’s judgment and institutional policy. Therefore, selection bias and residual confounding cannot be fully excluded. Second, a larger proportion of thoracotomy cases were performed during the early study period, and improvements in device technology and procedural techniques over time may have influenced perioperative outcomes and prognosis. Third, the overall sample size was relatively limited, and for low-frequency events such as in-hospital mortality and ischemic stroke, the statistical power may have been insufficient to detect significant differences. Third, to enable a two-group comparison, TA and DA approaches were combined into a single thoracotomy group in this study. However, there may be inherent heterogeneity between the TA and DA approaches in terms of procedural characteristics and complication profiles, which represents one of the limitations of this study.
Comments (0)