
Remember me
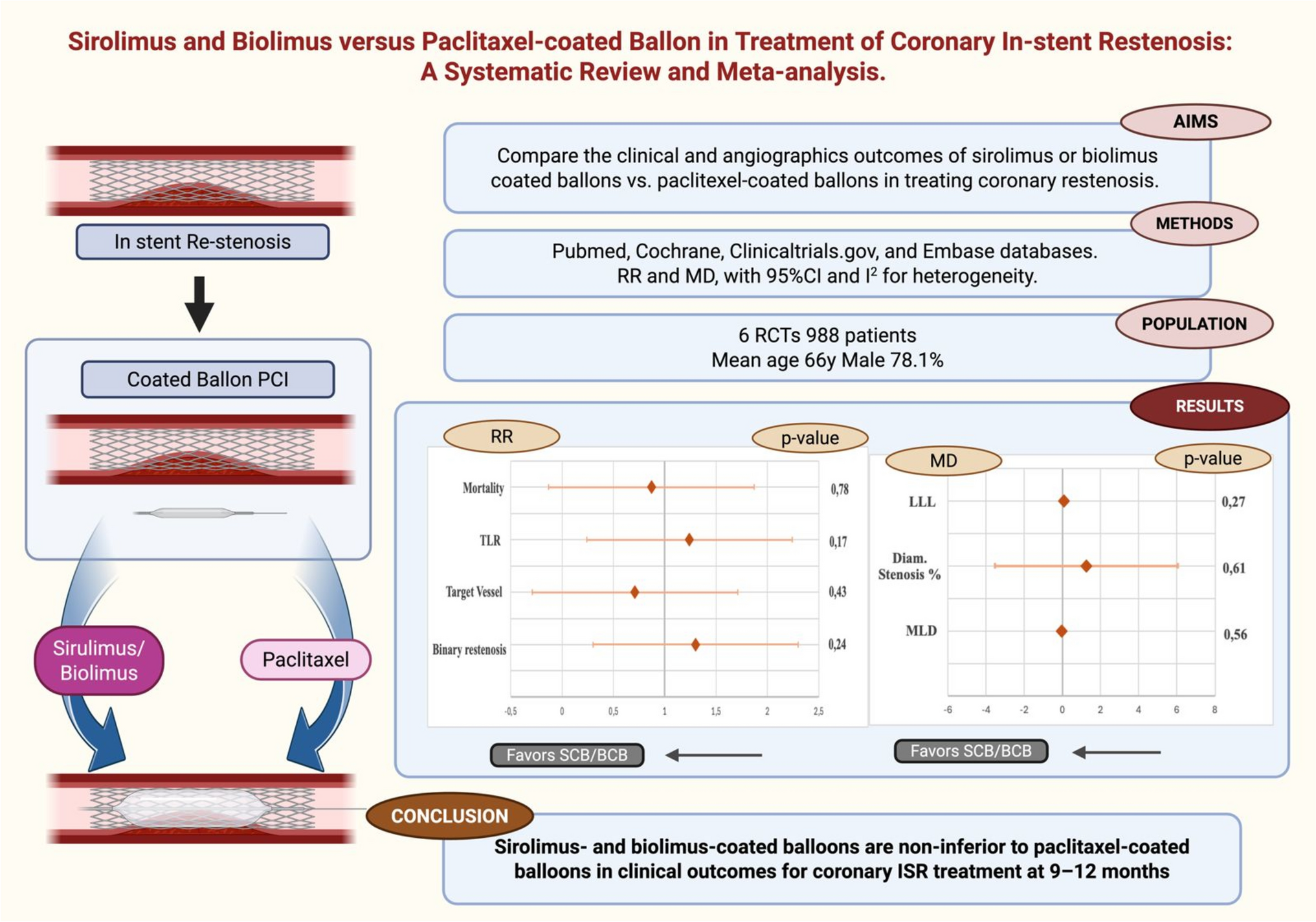
This meta-analysis included 6 randomized controlled trials [9,10,11,12,13,14] with a total of 988 patients with coronary In-stent restenosis, where 527 participants in the SCB(n = 252)/BCB group (n = 275) were compared with 458 patients in PCB group across various clinical endpoints. The mean age of the patients across the studies was 65.4 years, mean BMI of 27.54 kg/m2 and the follow up duration was 9–12 months. The detailed characteristics of the individual studies are provided in Table 1.
ResultsThe pooled analysis demonstrated comparative results between SCB or BCB and PCB across various clinical efficacy and safety endpoints, suggesting no clear superiority of one treatment modality over the other.
The Target lesion revascularization (TLR) did not show any statistically significant difference between both the groups with null heterogeneity (RR = 1.24, 95%CI = 0.91, 1.69, p = 0.17, I2 = 0% Fig. 2A), and subgroup analysis comparing both SCB and BCB independently with PCB showed similar results with no subgroup difference (p = 0.32 Fig. 2B). Subgroup analysis based on type of ISR whether DES and BMS-ISR or DES-ISR, also showed similar results with test for subgroup showing no significance (p = 0.6 Fig. 2C).
Fig. 2
A: Pooled analysis of Target lesion revascularization (TLR) at follow-up comparing both SCB and BCB with PCB in Coronary ISR. B: Subgroup analysis based on type of balloon (SCB or BCB vs PCB) for TLR at follow-up. C: Subgroup analysis based on type of prior stent (DES/BMS) In-stent restenosis (ISR) for TLR at follow-up
The all-cause mortality did not show any difference whether the patients were treated with SCB/BCB vs PCB (RR = 0.87, 95%CI = 0.32, 2.38, p = 0.78, I2 = 0% Fig. 3A), and subgroup analysis based on type of balloon utilized and type of ISR showed similar results with no significant subgroup difference (Fig. 3B, 3C).
Fig. 3
A: Pooled analysis of All-Cause mortality (ACM) at follow-up comparing both SCB and BCB with PCB in Coronary ISR. B: Subgroup analysis based on type of balloon (SCB or BCB vs PCB) for ACM at follow-up. C: Subgroup analysis based on type of prior stent (DES/BMS) In-stent restenosis (ISR) for ACM at follow-up
A similar trend was noted in target vessel myocardial infarction (TVMI) (RR = 0.71, 95% CI = 0.29, 1.69, P = 0.43, I2 = 0% Fig. 4A, 4B, 4C) suggesting similar results upon pooled analysis and subgroup analysis. Binary restenosis percentage did not differ in patients treated with either SCB/BCB or PCB (RR = 1.30, 95% CI = 0.83, 2.05, P = 0.25, I2 = 53% Fig. 5A), despite subgroup analyses based on the type of balloon utilized, SCB vs PCB and BCB vs PCB (p = 0.58 Fig. 5B) and based on type of stent of ISR with test for subgroup statistically non-significant (p = 0.36 Fig. 5C).
Fig. 4
A: Pooled analysis of Target vessel Myocardial Infarction (TVMI) at follow-up comparing both SCB and BCB with PCB in Coronary ISR. B: Subgroup analysis based on type of balloon (SCB or BCB vs PCB) for TVMI at follow-up. C: Subgroup analysis based on type of prior stent (DES/BMS) In-stent restenosis (ISR) for TVMI at follow-up
Fig. 5
A: Pooled analysis Binary stenosis (BS) in segment at follow-up comparing both SCB and BCB with PCB in Coronary ISR. B: Subgroup analysis based on type of balloon (SCB or BCB vs PCB) for Binary stenosis at follow-up. C: Subgroup analysis based on type of prior stent (DES/BMS) In-stent restenosis (ISR) for BS at follow-up
Late lumen loss (LLL) suggests more tissue growth and higher likelihood of restenosis, mean difference (MD) of late lumen loss is 0.07 (95% CI = -0.06, 0.20, p = 0.30, I2 = 69% Fig. 6A) when compared between both the groups, and when SCB was compared with PCB (MD: 0.05 95% CI: -0.04, 0,14 p = 0.31, I2 = 0% Fig. 6B). When BCB was compared with PCB, late lumen loss shows a MD: 0.15 (95% CI -0.20, 0.51, p = 0.39 I2 = 93% Fig. 6B) with very high heterogeneity. Despite subgroup analysis based on type of ISR (DES + BMS or DES), late-lumen loss was comparable in either SCB/BCB or PCB with no significant difference in subgroups (p = 0.4 Fig. 6C).
Fig. 6
A: Pooled analysis of Late Lumen Loss (LLL) at follow-up comparing both SCB and BCB with PCB. B: Subgroup analysis based on type of balloon (SCB or BCB vs PCB) for LLL at follow-up. C: Subgroup analysis based on type of prior stent (DES/BMS) In-stent restenosis (ISR) for LLL at follow-up
Diameter stenosis in percentage showed a mean difference of 1.39% (95% CI = -3.59, 6.37, p = 0.58, I2 = 71% Fig. 7A) between the two groups. When analyzed based on the type of balloon utilized, SCB showed MD of -0.82% with null heterogeneity (95% CI = -3.90, 2.26, p = 0.60, I2 = 0%), and BCB showed MD of 6.23% (95% CI = -4.41, 16.88, p = 0.25, I2 = 89%) (Fig. 7B). Subgroup analysis based on type of stent of ISR, also showed similar results (Fig. 7C). Minimal Lumen diameter showed a reduction of 0.04 mm (95% CI: -0.20, 0.11, p = 0.59, I2 = 68%) with SCB/BCB group vs PCB group (Fig. 8A), when analyzed based on the type of balloon used, SCB and BCB independently showed no significant difference compared to PCB (Fig. 8B). Similar results were also noted when analyzing subgroups based on type of stent of ISR (Fig. 8C).
Fig. 7
A: Pooled analysis of Diameter stenosis in % at follow-up comparing combined SCB and BCB with PCB in patients with Coronary ISR. B: Subgroup analysis of DS in % at follow-up comparing SCB or BCB with PCB in patients with Coronary ISR. C: Subgroup analysis based on type of prior stent (DES/BMS) In-stent restenosis (ISR) for DS in % at follow-up
Fig. 8
A: Pooled analysis of MLD at follow-up comparing combined SCB and BCB with PCB in patients with Coronary ISR. B: Subgroup analysis of MLD at follow-up comparing SCB or BCB with PCB in patients with Coronary ISR. C: Subgroup analysis based on type of prior stent (DES/BMS) In-stent restenosis (ISR) for MLD at follow-up
When analyzing selectively SCB vs PCB in patients with coronary DES-ISR, late lumen loss, minimal lumen diameter, diameter stenosis in % and binary stenosis in segment all showed no statistically significant difference between the two groups (Fig. 9A ,9B, 9C, 9D).
Fig. 9
A: LLL at follow-up comparing SCB and PCB in patients with Coronary DES-ISR. B: MLD at follow-up comparing SCB and PCB in patients with Coronary DES-ISR. C: Diameter stenosis in % at follow-up comparing SCB and PCB in patients with Coronary DES-ISR. D: BS in segment at follow-up comparing SCB and PCB in patients with Coronary DES-ISR. SCB: Sirolimus-coated balloons, BCB: Biolimus-coated balloons, PCB: Paclitaxel-coated balloons, RR: relative risk, CI: confidence interval, M-H: Mantel-Haenzel, MD: mean difference, SD: Standard deviation, DES: Drug Eluting Stent, ISR: In-stent restenosis, BMS: Bare Metal Stent
The absence of statistical significance in this study’s outcomes could be due to inadequate sample size, short follow-ups or a smaller number of events.
Subgroup analysis based on individual use of either SCB or BCB compared to PCB and type of stent of ISR, either DES + BMS or DES, for the outcomes of Target lesion revascularization, all-cause mortality, target vessel myocardial infarction, binary restenosis, late lumen loss, diameter stenosis in % and minimal lumen diameter also exhibited similar results as the overall pooled analysis.
Sensitivity analysisHeterogeneity is null for most of the outcomes, suggesting consistency across the included studies. However, few outcomes, like late lumen loss, diameter stenosis percentage, minimal lumen diameter, and binary restenosis, revealed high heterogeneity, which was assessed by leave-one-out analysis (Supplementary Figs. 9.1—9.4). Sensitivity analysis was conducted by omitting one study at a time via leave-one-out analysis, which significantly eliminated the heterogeneity and maintained the direction of association, further indicating robust results. With the low level of heterogeneity and the drop in heterogeneity upon leave-one-out sensitivity analysis, there is a level of consistency and uniformity across the included studies.
Funnel plots were also performed to assess publication bias of each outcome, where the horizontal axis represents effect size, either MD or RR, and the vertical axis represents standard error (SE) of the effect size. Each circle represents an individual study, with the size indicating study precision—larger distances from the dashed line at zero may indicate potential bias or variability in study results. The symmetric appearance of the funnel plot generally indicates a low risk of publication bias. However, asymmetry may suggest selective publication or other biases impacting the results. The point farther from the cluster might indicate a study with distinct results, warranting further investigation. On examining all the funnel plots, mild asymmetry is noted in outcomes like binary restenosis in the segment, LLL, diameter stenosis in percent, and MLD (supplementary Figs. 10.4 to 10.7), indicating consistency of the outcome in all studies and minimal bias. Funnel plot of TLR and Target vessel MI (supplementary Fig. 10.1 and 10.3) shows relative symmetry with one study appearing as an outlier, potentially due to different methodologies or populations, indicating the need for further exploration. Visual inspection shows moderate asymmetry with mortality outcome, suggesting some degree of publication bias or heterogeneity among the included studies, but not substantial, highlighting the need for cautious interpretation of pooled results (supplementary Fig. 10.2).
Quality assessmentRisk of bias was evaluated by two independent authors (C.L. and J.M.) at the study level using the Cochrane Risk of Bias 2 (RoB 2) tool across the following domains: [1] bias arising from the randomization process; [2] bias due to deviations from intended interventions; [3] bias resulting from missing outcome data; [4] bias in outcome measurement; [5] bias in selection of the reported results; and [6] overall risk of bias. All included RCTs were judged to have a low risk of bias, as illustrated in Supplemental Fig. 11.
GRADE assessment and certainty of evidenceThe certainty of evidence for each outcome was assessed using the GRADE framework, and a summary of findings table was created (supplementary Table 3). Overall, the evidence ranged from moderate to very low certainty. For target lesion revascularization (TLR), the relative effect estimates favored neither SCB/BCB nor PCB definitively, with low certainty due to imprecision and risk of bias. Mortality and target vessel myocardial infarction were rare, resulting in wide confidence intervals and low certainty ratings. Binary restenosis showed high variability, particularly with BCBs, leading to very low certainty due to serious inconsistency and imprecision. Continuous outcomes, including late lumen loss, diameter stenosis percentage, and minimal lumen diameter, showed no statistically significant differences between treatment groups. These were generally rated as low certainty, except in the SCB vs PCB subgroup for late lumen loss, which reached moderate certainty due to consistent and precise estimates. The overall body of evidence suggests no clear superiority of SCB/BCB over PCB, with limitations in precision, consistency, and event frequency reducing confidence in the findings.
Comments (0)