Study design and patients
This retrospective study was approved by the institutional ethics committee of Beijing Aier-Intech Eye Hospital and was conducted according to the tenets of the Declaration of Helsinki. The need for informed consent was waived owing to the retrospective nature of the study.
Patients who underwent FS-CRI combined with ICL implantation and TICL implantation at Beijing Aier-Intech Eye Hospital between March 2021 and December 2022 were included in the study.
The inclusion criteria were as follows: (1) age ≥ 18 years; (2) stable refraction within 2 years; (3) regular low-to-moderate astigmatism ranging from 0.75 D to 2.25 D (Regular astigmatism is that refractive condition which is amenable to correction by cylinders. The axes of the principal meridians of the astigmatism are at right angles to each other.); [23] (4) endothelial cell density (ECD) ≥ 2000 cells/mm2; (5) anterior chamber depth (ACD) ≥ 2.8 mm. The exclusion criteria were corneal pathology (e.g., corneal opacity, leukoplakia, pterygium, abnormal topography, subclinical keratoconus and keratoconus), previous ocular surgery, severe dry eye, any systemic contraindications for surgery (e.g., autoimmune disorders) and nystagmus not indicated for femtosecond laser surgery.
Preoperative evaluation
All patients underwent a preoperative evaluation of uncorrected (UDVA) and corrected (CDVA) distance visual acuity, ultrasound biomicroscopy, slit-lamp biomicroscopy, ultrasound biomicroscopy, refraction, endothelial cell density, partial coherence interferometry (IOLMaster − 700, Carl Zeiss Meditec Inc., Dublin, CA, USA), Lenstar LS900 (Haag-Streit Inc., Köniz, Switzerland), and an autorefractor (ARK-510 A, Nidek Inc., San Jose, CA, USA). Scheimpflug pachymetry (Pentacam, Oculus Inc., Saint Louis, MO, USA) was used to examine the regularity of astigmatism. Total wavefront aberration and retinal image quality parameters were obtained at the 4.0-mm zone from OPD Scan III (Nidek Inc., San Jose, CA, USA). The power and size calculation of the ICL or TICL were performed using the STAAR surgical calculator (https://evo-ocos.staarag.ch/). The UDVA and CDVA were examined using standard logarithmic visual acuity charts and then converted to the logMAR scale for the statistical analysis.
Corneal relaxing incisions
The epithelium- and Bowman-penetrating CRIs were designed by the Donnenfeld nomogram using the online calculator (https://www.lricalculator.com/), which already built in adjustment for with-the-rule/against-the-rule astigmatism and age. This nomogram was originally designed for manual LRI; therefore, we modified the diameter and depth of the nomogram based on our previous clinical observations [22, 24].
The data including steep keratometry (K), flat K, and steep meridian, were entered into the online calculator and were determined by the surgeon according to the automated phoropter (RT-5100, Nidek Inc., San Jose, CA, USA) and Scheimpflug pachymetry. For surgically induced astigmatism (SIA) of the primary incision, 0.31 D was entered. The meridian incision location was 150 degrees.
Surgical technique
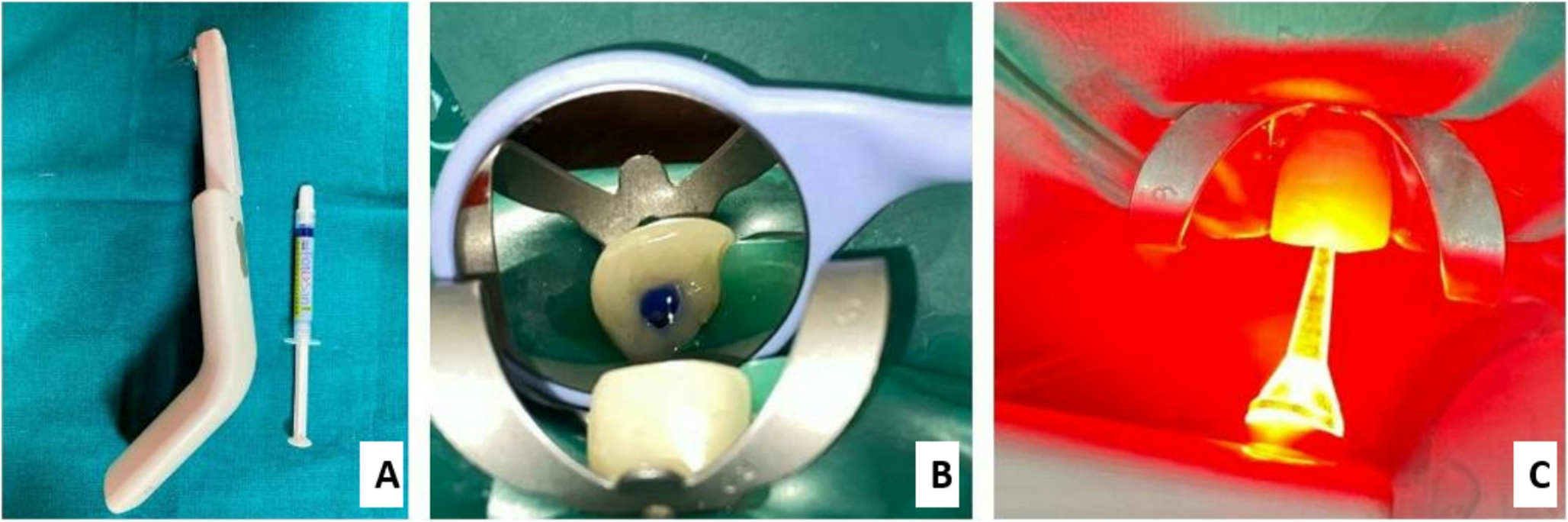
All surgical procedures were performed by an experienced surgeon. Before docking, the patient’s corneal limbus was marked at the 0 degrees and 180 degrees positions using sterile skin markers (Medplus, Inc., Hyderabad, India) while the patient sat upright. The horizontal marks of the LenSX femtosecond laser platform were manually aligned with the limbal marks. Then, paired symmetrical CRIs were placed at a diameter of 8.7 mm, with a depth of 90% of corneal pachymetry, plus energy of 3.2 µJ, side cut angle of 90 degrees, and spot and layer separation of 4.0 μm for both. All CRIs were epithelium- and Bowman-penetrating. After finishing the FS-CRI, patients were transferred to another room for ICL implantation. A 3.0-mm corneoscleral limbal primary incision at 150 degrees and a 1.2 mm auxiliary incision at 30 degrees were created with a disposable steel keratome, and the ICL was implanted into the ciliary sulcus using a traditional two-step procedure. The CRIs were bluntly opened at the end of the surgery. In the TICL group, all the patients did not perform FS-CRI, and the position of the TICL was adjusted according to the horizontal marks. Conventional anti-inflammatory agents and topical antibiotic were administered for 1 month postoperatively.
Postoperative follow-up measurements at 1 day, 1 week, 1 month, and 3 months included UDVA, CDVA, manifest refractions, OPD Scan III, and anterior segment OCT were uesd to measure the vault. Any surgery-related complications, such as postoperative infection, glaucoma, cataract, epithelial implantation, and excessive or insufficient vault, were documented. The vault was defined as normal when measuring 250–750 μm, low when < 250 μm, and high if > 750 μm [25]. Refractive astigmatism values were measured using an autorefractor.
Vector analysis of astigmatic correction
The Alpins vector analysis method analyzes the changes in astigmatism by converting them into horizontal (X) and vertical (Y) coordinates in a rectangular coordinate system [26, 27]. There are three basic vectors: target induced astigmatism (TIA), surgically induced astigmatism (SIA), and difference vector (DV). TIA indicated the astigmatic correction aimed to achieve with the arcuate incisions (AIs). Meanwhile, SIA indicated the astigmatic correction truly achieved by the AIs. DV indicated the further astigmatism required to achieve the intended outcome. Other indicators were calculated from these three vectors. The correction index (CI) is the ratio of SIA to TIA, with an ideal value of 1.0. The index of success (IOS) is the ratio of DV to TIA. The flattening index (FI) is a measure of SIA on the astigmatic change at its intended axis. The angle of error (AE) is the difference in the angle between the axis of SIA and TIA. The magnitude of error (ME) is the arithmetic difference between SIA and TIA.
Statistical analysis
Sample size calculation formula \(N=\frac\)was employed to determine the required sample size for the study. Statistical analyses were performed using SPSS software (version 22.0, IBM Corp.). Continuous variables were expressed as the mean ± standard deviation, while categorical variables were expressed as frequency and percentage. Shapiro Wilk and P-P plots were used to check the normality of the data distribution. Normally distributed preoperative and postoperative data were compared using a paired t-test, while non-normally distributed data were compared using a Wilcoxon signed-rank test. Between-group comparisons of age and of sex differences were performed using Student’s t-test and the chi-square test, respectively. Linear mixed models were used to compare ocular biometric parameters, refractive astigmatism, vector parameters, total wavefront aberration and retinal image quality parameters among groups while accounting for correlations between the records from the two eyes of the same patients (i.e. a random intercept) [9]. A P-value < 0.05 was considered statistically significant.

Comments (0)