
Remember me
In short axial length eyes, anterior segment crowding places cataracts in proximity to the corneal endothelium[12], increasing the risk of endothelial damage during conventional surgery. FLACS revolutionized these challenges after Nagy et al.5 first applied it to key surgical steps. By reducing manual operation in narrow anterior chambers, FLACS reduces phacoemulsification energy, thereby mitigating endothelial injury. Some scholars have said that one of the main challenges in phacoemulsification surgery is achieving a continuous curvilinear capsulorhexis[20]. Its precision in capsulotomy size and centration also improves IOL positioning compared with manual techniques[21,22], making it particularly valuable for short-axial-length patients.
However, laser capsulotomy has limitations: laser-induced capsulotomy rims often have notches, reducing tensile strength and increasing tear risks[23]. Incomplete anterior capsulotomy can also be caused by corneal opacities such as scars or radial keratotomies, laser misfires, or tremors in the eye during laser delivery[23,24]. It has been demonstrated that FLACS induces LEC apoptosis in LEC adjacent to the capsulotomy edge, which is linearly connected with laser energy parameters and time[25,26,27]. FLACS also reliably produces capsulotomies that contribute to bag stability and the eradication of LEC. Theoretically, this impact could lower capsular shrinkage rates after the operation.
As femtosecond laser-assisted cataract surgery becomes increasingly popular, we compare the two most popular femtosecond laser systems in China. Since each device has its own unique characteristics and there are many patients with short axial lengths in China, we hope to identify the advantages and disadvantages of the two devices through this study, so that they can better leverage their strengths in their respective fields.
We discovered during the operation that the femtosecond laser time was quite short when the cataracts of patients in the Catalys group were light in opacity and thin in thickness, with the shortest time being only 15 s, and that the femtosecond laser time could reach 117 s when the cataracts were severely cloudy, hard, and thick. The shortest and longest times in the LenSx femtosecond system are 29 and 74 s, respectively. There were no statistically significant differences between the two groups post-femtosecond laser therapy, CDE, EPT, fluid perfusion volume, or postoperative corneal endothelial counts and corneal endothelial loss. Regardless of the laser time, the results and safety for the two groups are essentially the same. When the cataract is less hazy and thinner, Catalys is quite effective, with acceptable outcomes.
Notably, the baseline ACD in both groups falls within the safe range for femtosecond laser-assisted cataract surgery in short axial length eyes, ensuring the feasibility and safety of both platforms for this anatomically challenging population. Our primary aim was to compare CDE, EPT, and corneal endothelial cell changes between the two systems. The absence of statistically significant differences in these key efficacy and safety metrics provides a critical basis for clinical decision-making. This finding implies that both LenSx and Catalys can achieve comparable therapeutic effects in terms of energy use and endothelial protection, allowing surgeons to prioritize secondary considerations, such as femtosecond laser time, when selecting devices. Specifically, Catalys, with its shorter laser time in softer cataracts, may be preferred for poorly cooperative patients to minimize intraoperative risks associated with eye movement. In contrast, LenSx, with its stable laser performance across all cataract densities, is better suited to dense cataracts, where consistent procedural efficiency is crucial. This strategic device selection, grounded in the non-inferiority of core surgical outcomes, bridges the gap between our primary comparative aims and the observed differences in laser time, providing practical clinical guidance for individualizing treatment in short-axial-length patients.
Theoretically, maintaining the continuity of laser spots is crucial for ensuring the safety and stability of continuous curvilinear capsulorhexis. For instance, smaller spot spacing enhances capsulotomy continuity but tends to prolong laser time, while standardized parameters are essential to ensure comparability between different laser platforms. In the initial study design, we unified all key controllable parameters across the two systems, including Horizontal Spot Spacing (10 μm) and Vertical Spot Spacing (40 μm), to eliminate confounding factors introduced by parameter discrepancies. Thus, the observed differences in femtosecond laser time between LenSx and Catalys are based on a fully comparable foundation and objectively reflect the inherent clinical performance differences between the two platforms. However, the exact mechanisms underlying these differences, despite consistent parameter settings, remain to be explored in future studies, which may involve device-specific laser energy transmission modes, scanning accuracy, or interactions with lens opacity characteristics. This standardized parameter design strengthens the validity of our findings regarding tailored device selection based on laser time variability.
Regarding complications, we found that the incidence of in-continuity capsulorhexis was higher in the LenSx group. In contrast, the incidences of Pupil miosis and subconjunctival hemorrhage were higher in the Catalys group. Moreover, one patient in the Catalys group had negative pressure loss. However, there was no statistically significant difference in any of the indicators mentioned above. Of course, this might be attributed to the limited sample size incorporated in this study. This is mainly because the LenSx femtosecond laser system uses a relatively rigid PI connection, unlike the Catalys system. We all know that patients with short axial lengths tend to have shorter corneal diameters, and the PI junction of LenSx may cause the corneal crease to scatter light, resulting in continuous curvilinear capsulorhexis discontinuity[18]. Instead of a flat contact, which does not cause corneal creases[28], Catalys is replaced by a ring of negative-pressure suction, so that the required negative pressure is no more than 15 mmHg, and the patient is more comfortable, and the central fluid is in contact with the laser probe[29].
However, this advantage is not shown in all aspects. We note that the incidence of conjunctival hemorrhage was 6% in the LenSx group and 18% in Catalys. This may be because the PI of the LenSx femtosecond system primarily shows a flattening process, while Catalys primarily uses negative-pressure suction. Most of the cataract patients in this study were elderly, and conjunctival laxity and fragile blood vessels were observed. Negative pressure suction inevitably caused more serious subconjunctival hemorrhage, which has been confirmed by scholars[30]. Fortunately, there was no effect on postoperative visual function. Finally, we found that there was a certain probability of myosis after femtosecond laser surgery in both groups, 8% in the LenSx group and 10% in the Catalys group. This is mentioned in almost all literature on FLACS complications. The production of prostaglandin and other inflammatory mediators by the ciliary body in reaction to the dissipation of laser energy, which causes an increase in temperature, shock waves, and vibrations, is thought to be a cause of pupil miosis[31]. Laser pulse energy is thought to play an important role in the degree of inflammatory response generated by the femtosecond laser[32]. Preventing pupil miosis may be possible with topical NSAID pretreatment since it is thought to reduce prostaglandin production[33], but it’s not entirely avoidable. Finally, one patient in the Catalys group experienced a loss of negative pressure, but fortunately, most of the laser work had already been completed by then. This may be due to the patient’s short corneal diameter, and the negative-pressure suction ring was completely absorbed into the conjunctiva, which allowed the eyeball to remain mobile. Negative pressure loss might occur when the patient does not cooperate.
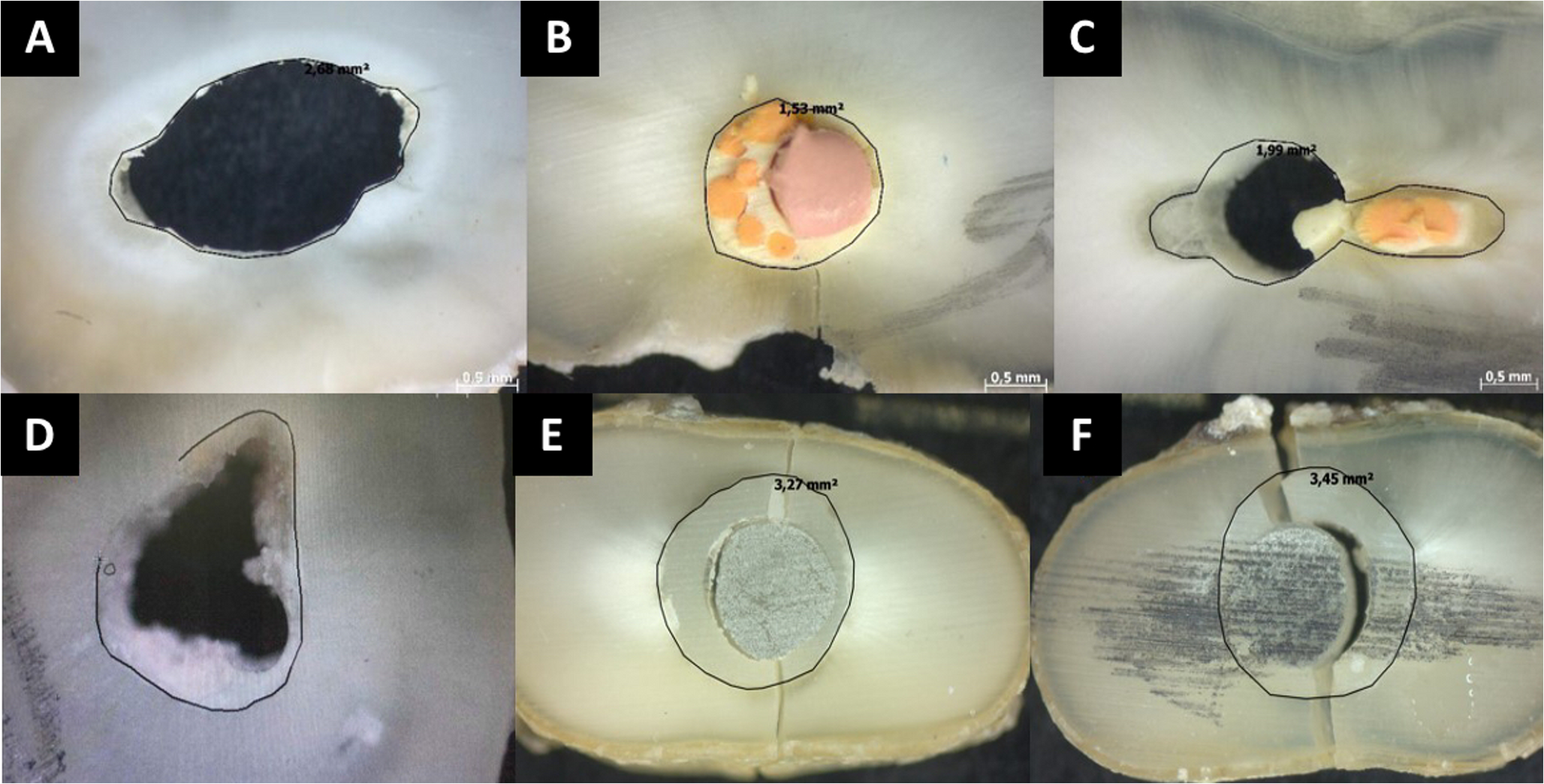
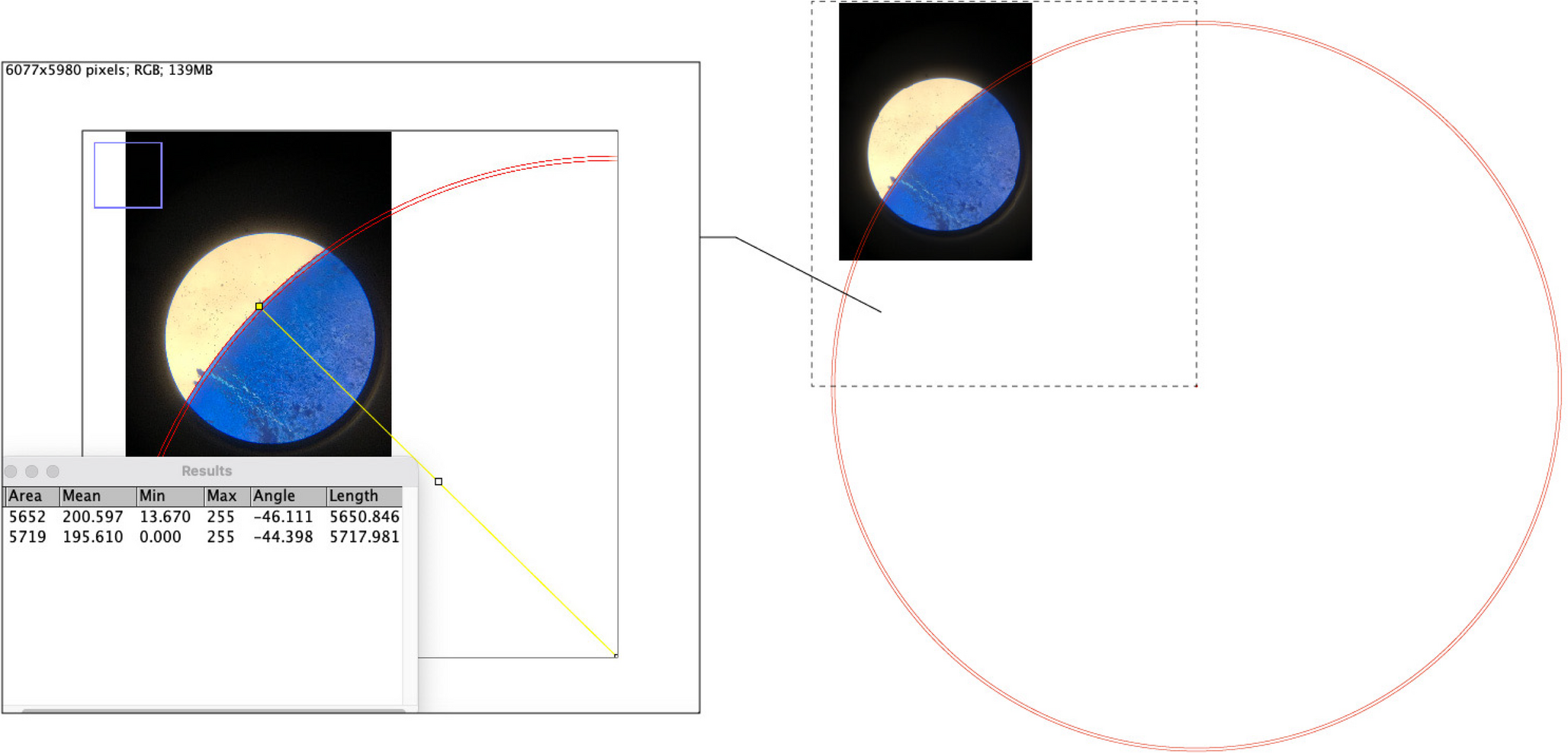
Moreover, we analyzed the cell-free area at the capsule edge to explore the potential of a femtosecond laser to reduce the incidence of capsular shrinkage. Although capsule tissue in the Catalys group was found to have a smaller cell-free area of capsule edge when stained, no capsular shrinkage was observed in either of the two groups. This indicates that the LEC characteristics of dissociative capsule tissue alone cannot accurately reflect the actual situation in the patient’s eye. Secondly, we found that the number of irregular structures after femtosecond laser capsulorhexis between the two groups showed significant differences, and the integrity of the Catalys group was better. However, we also found that the marginal irregular structures in the LenSx group were mostly a small range of wedge-shaped irregularities, with the anterior and posterior surfaces of the capsule were not in the same vertical plane. Although the number of irregular structures was small in the Catalys group, a high proportion of filamentous remains were present, as shown in Part B of Fig. 4. Sometimes these filaments can even be seen by the naked eye during surgery through a microscope, which can cause some confusion during the procedure (Fig. 5). This could be due to the slight movement of the patient’s eye during femtosecond capsulorhexis, even though the Catalys laser system can complete capsulorhexis in about 1 s. But our observations indicate these filaments may be inadvertently pulled during operation, introducing irregular, unpredictable tension on the otherwise circular capsular edge. In short axial length eyes with crowded anterior segments, such uneven forces could compromise capsular integrity and increase the risk of capsular rupture- though no such incidents occurred in our series. Given the paucity of existing data, this finding warrants further investigation to clarify its clinical impact. Therefore, Catalys does not have an advantage in capsulorhexis regularity, as the data suggest.
Fig. 4
(A) Irregular capsular edge structures induced by the LenSx femtosecond laser system (×640 magnification). (B) Filamentous capsular tissues from the Catalys femtosecond laser system (×160 magnification)
Fig. 5
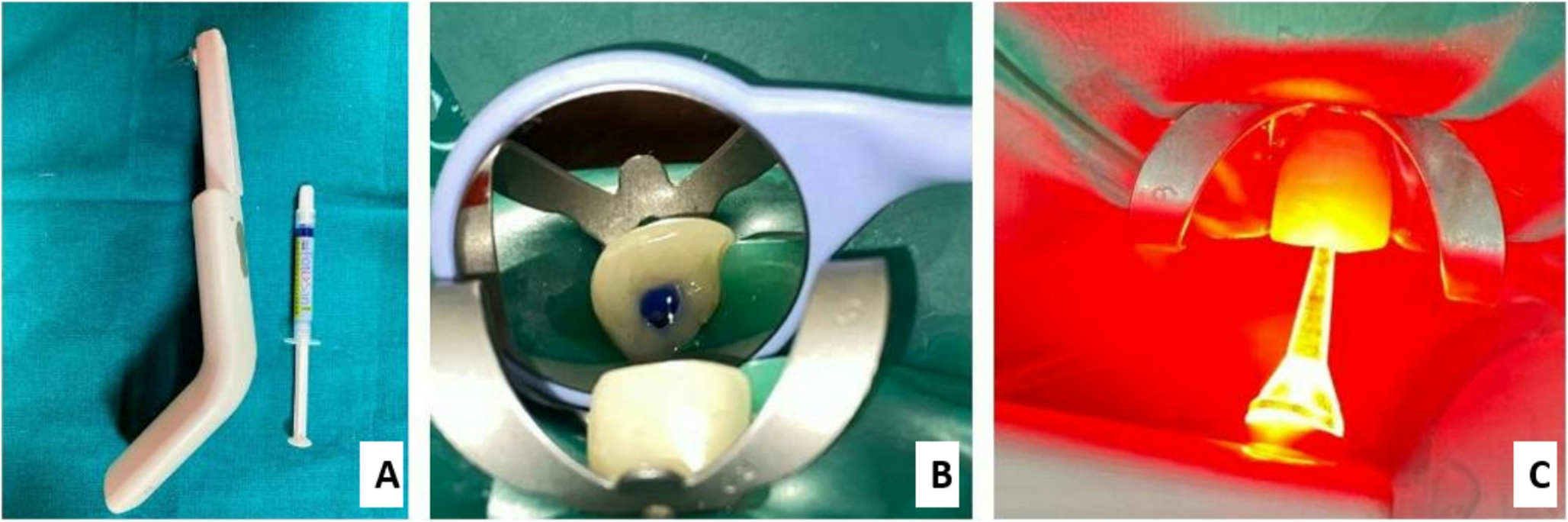
Residual filamentous capsular tissue after Catalys-assisted capsulorhexis. (A) The red arrow indicates filamentous tissue (one end attached to the capsular periphery, the other free). (B) Removal of filamentous tissue via forceps
Regarding capsular tissue analysis, Diff-Quick staining was chosen for its rapidity and sufficient resolution to meet the needs of our study endpoints (cell-free area quantification and irregular structure counting). While HE staining and TEM offer more detailed histological or ultra-structural information, which is a limitation of our study, they are more time-consuming and costly, and unnecessary for the specific observations we focused on. Our targeted investigation of short axial length eyes continues to provide valuable clinical insights for device selection in this population. The capsular shrinkage incidence was 0% in both groups, making this endpoint uninformative for group comparison. This finding may be attributed to the relatively short 6-month follow-up period and limited sample size, as capsular contraction is a rare long-term event that requires larger cohorts and longer follow-up to detect. Our study was underpowered for this exploratory endpoint, and future studies with extended follow-up are needed to evaluate further the impact of the two laser systems on capsular shrinkage.
Beyond capsular-related observations, we also noted device-specific characteristics during surgical implementation with the Catalys system. Specifically, when using the Catalys femtosecond laser, we discovered that despite selecting the correct PI size, the eye fixation effect remained unsatisfactory due to the laser’s annular negative-pressure suction[34]. It is worth noting that the Catalys femtosecond laser system’s machine bed design can make the surgeon more efficient in completing the operation. Dick HB et al.[35] proposed that the femtosecond laser and the operating table should be in the same room. Vasquez-Perez A et al. also proposed that phacoemulsification immediately after the femtosecond laser, so that there is no delay between the femtosecond laser pretreatment and phacoemulsification, is an important measure to reduce the pupil miosis after laser surgery[36], and, in this respect, the Catalys femtosecond laser system will offer greater advantages.
According to the study’s findings, using different femtosecond laser systems for different patients may further enhance the benefits of each system. Catalys may be a favorable choice for soft cataracts or poorly cooperative patients with short axial lengths, given its shorter laser time and better patient comfort with a non-flattening interface. LenSx may be better suited for dense/hard cataracts, as its stable laser time and capsulotomy performance may reduce intraoperative challenges in complex cases. Both systems show comparable safety in endothelial protection and complication rates. Clinicians should prioritize cataract density and patient cooperation to optimize surgical outcomes in this anatomically challenging population. However, these observations need confirmation through subgroup analyses with larger sample sizes. The current study was not powered to detect subgroup differences. Additionally, these conclusions are based on the specific femtosecond laser parameters used in this research. Future advancements in personalized parameter setting are anticipated as more research in this area emerges.
Comments (0)