
Remember me
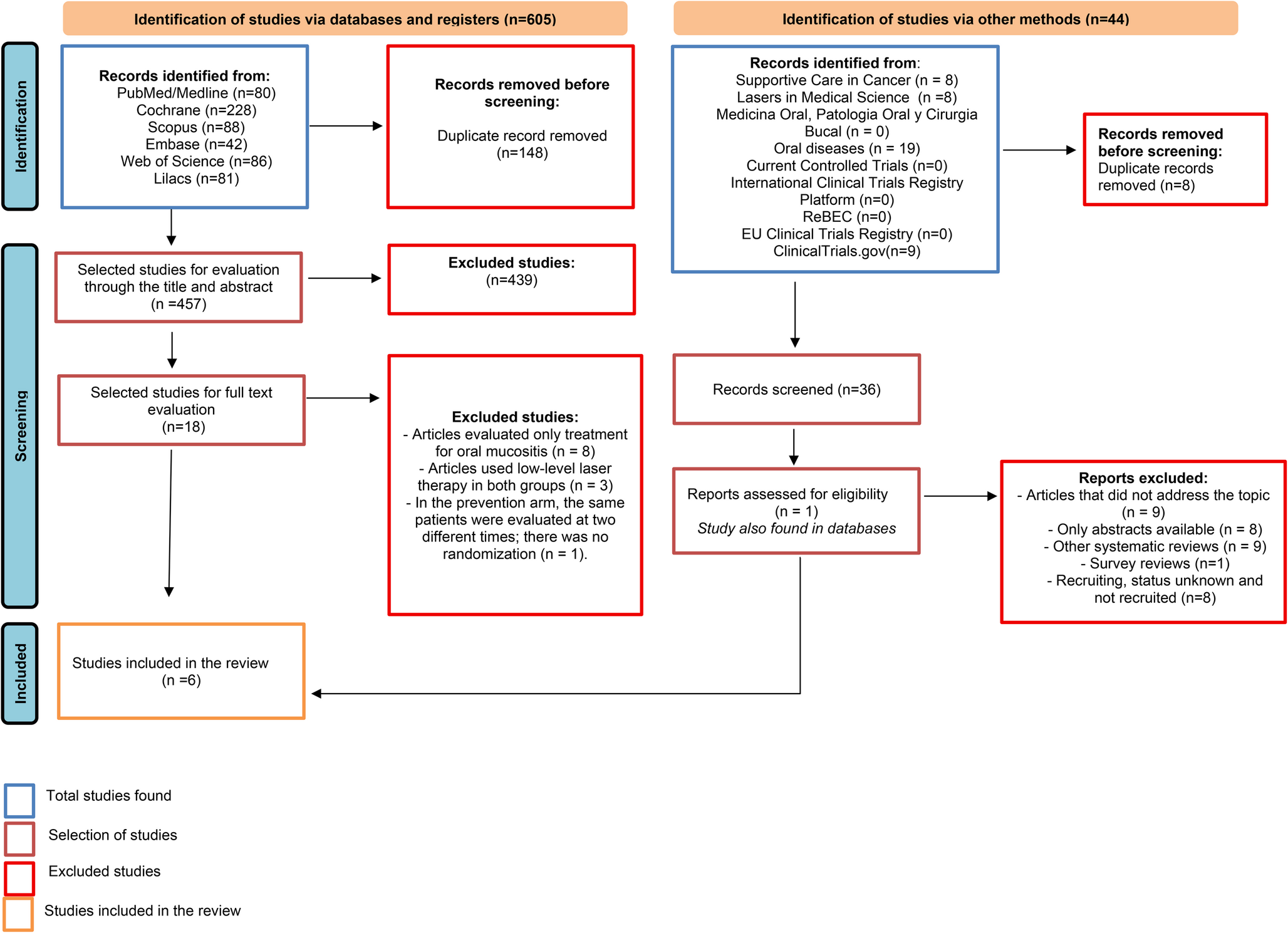
A total of 605 studies were identified in this systematic review, selected from the Embase, Medline/PubMed, Cochrane, Scopus, Web of Science and LILACS databases. After removing duplicates, a total of 457 studies were screened and evaluated, of which 439 did not meet the pre-established eligibility criteria. Only 18 remaining studies passed to the full text evaluation stage, of which twelve were excluded due to methodological criteria and research design. After applying all the predetermined criteria, six RCTs [23,24,25,26,27,28] dated between 1997 and 2024 met the inclusion criteria and comprised the final analysis (Fig. 1). The agreement between the authors according to the Kappa test was 0.81, which means “almost perfect agreement”.
Fig. 1
PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers and other sources
Description of included studiesThis systematic review included six RCTs that evaluated the efficacy of PBM as a preventive strategy for OM in patients with hematologic diseases undergoing CT. All studies randomly analyzed the effects of the laser therapy on intervention PBM and control groups (CG) (Simulated PBM and/or oral care). (Table 2).
Table 2 Summary of the characteristics of the studiesCowen et al. [23] followed 30 patients aged 18–58 years, in two groups (15 in the PBM group and 15 in the control/simulated PBM group), diagnosed with acute lymphoblastic leukemia, acute myeloblastic leukemia, non-Hodgkin’s lymphoma and multiple myeloma. All individuals underwent HSCT and were previously conditioned with: intravenous cyclophosphamide (D-5, D-4) or intravenous melphalan (d-5). The He-Ne laser group received application for five consecutive days (from day − 5 to day − 1; before transplantation), in five anatomical sites on the right and left side of the oral cavity: lower labial mucosa and adjacent gum, upper labial mucosa and adjacent gum, buccal mucosa and adjacent gum, ventral and lateral tongue and floor of the mouth (15 points in each anatomical site), with a wavelength of 632.8 nm, 10 s per point and 54 J of total energy. The control group was treated with a sham laser. Therefore, at the end of 21 days, a cumulative OM score was created, demonstrating the effect of PBM in reducing the maximum intensity of OM. Furthermore, daily cumulative pain scores, swallowing ability, and saliva production were better in the intervention group than in the control group.
Antunes et al. [24] analyzed the clinical effects of PBM in preventing and reducing OM induced by conditioning for HSCT. For this purpose, 38 patients were randomized into two groups (19 in the PBM group and 19 in the placebo group), with an average age of 36.5 years. Presenting diagnoses of hematologic cancers or hematologic diseases (Chronic or Acute Myeloblastic Leukemia; Hodgkin’s or non-Hodgkin’s Lymphoma; Acute Lymphoblastic Leukemia; and Myelodysplastic Syndrome). In the PBM group, the 660 nm InGaAlP laser was applied to 15 points per region for 16.7 s on the upper lip, lower lip (redness and lip mucosa), buccal mucosa, dorsum, ventral and lateral tongue, the floor of the mouth, and the hard and soft palates. Application began on day 1 of conditioning (D-7) and was discontinued on the day of neutrophil recovery. The placebo group did not receive PBM. The patients in the laser group who had presented with erythema or ulcers continued to receive the preventive laser with 4 J/cm². A crossover was allowed for patients from the control group who presented with a grade IV oral mucositis index of the World Health Organization (WHO) and/or an ulcer area more than or equal to 12 cm according to the Oral Mucositis Assessment Scale (OMAS). A therapeutic laser with 8 J/cm² per point was applied to these patients. In summary, the results of the study showed that the use of PBM had potential in reducing the incidence and severity of OM.
Khouri et al. [25] conducted a study with 22 patients undergoing allogeneic HSCT, diagnosed with hematologic cancer or hematologic diseases (Acute Myeloid Leukemia, Acute Lymphocytic Leukemia, Chronic Myeloid Leukemia, Severe Aplastic Anemia and Myelodysplastic Syndrome) to compare the frequency and evolution of OM, dividing the participants into two groups. The group undergoing PBM (n = 12) and the group undergoing only conventional therapy with “mucositis formula” (n = 10) underwent a conditioning regimen with High Doses (HD) of CT (Cyclophosphamide, Busulfan and Fludarabine), with different combinations. All patients underwent conditioning regimens with cyclophosphamide associated with other CT agents, and underwent treatment with Methotrexate (MTX) in combination with cyclosporine after HSCT. In the PBM group, InGaAlP lasers (660 nm - red laser) and GaAlAs lasers (780 nm - infrared laser) were applied for 10 s at each point, the application was from the beginning of the conditioning regimen until D + 15 post-transplant, on alternate days, in the following locations: upper and lower lips (vermilion and mucosa), bilateral buccal mucosa, floor of the mouth, lateral surface of the tongue on both sides and ventral surface of the tongue. In the conventional therapy group, the “mucositis formula” consisted of 0.15 g of benzydamine, 1.13 g of nystatin, 2 g of neotutocaine, and 10 mL of distilled water. According to the present study, the PBM group showed a lower frequency and progression of OM, as well as a reduction in the number and severity of lesions, when compared to the conventional therapy group.
Ferreira et al. [26] conducted an RCT with 35 patients (17 in the PBM group and 18 in the placebo group) with hematologic cancer (Leukemia, Lymphoma, Myeloma, and others), with a mean age of 42.44 years, undergoing CT protocols prior to autologous and allogeneic HSCT. The protocols used were Busulfan + Cyclophosphamide, Busulfan + Fludarabine, Carmustine (BCNU), Etoposide, Ara-C, Melphalan (BEAM); Melphalan and others. In the PBM group, applications were obtained at 27 points in the oral cavity, using the InGaAlP laser, with a wavelength of 650 nm, for 20 s per point. Applications were made to the upper and lower labial mucosa; bilateral buccal mucosa; dorsal, ventral and lateral surfaces of the tongue; retromolar region; soft palate; and floor of the mouth. The application was carried out from the 1 st to the 5th day of pre-transplant conditioning. In the placebo group, sham treatments were performed, with the laser on but no light emission. As a result, no statistically significant difference in the incidence of OM was observed between the groups, but PBM contributed to a reduction in the progression to severe OM and a decrease in pain intensity.
Boris et al. [27] included 33 pediatric patients, aged 1 to 17 years, in two groups (17 in the laser group with 47 courses of HD-MTX and 16 in the comparison group with 46 courses of HD-MTX), diagnosed with Acute Lymphoblastic Leukemia and non-Hodgkin’s Lymphoma.Patients were treated according to the following protocols: ALL-MB-2008 and ALL-BFM-2002-Rez, B-NHL-M-2010, NHL-BFM-95, including courses (two to four) of HD-MTX (1, 2, or 5 g/m2). The intervention group received preventive PBM on the 1 st day of the HD-MTX course (before the CT infusion), and afterwards, on the 3rd, 5th, 7th and 9th day. If OM developed, the protocols were performed therapeutically. Thus, the 670 nm wavelength was used in 13 zones of the oral mucosa susceptible to OM was irradiated sequentially: on the left and right - the tissues of the cheek along the line of occlusion of the teeth, the retromolar space, the lateral and ventral surfaces of the tongue, as well as the palate, upper and lower lips for 12 s per point. For therapeutic purposes, the laser was applied directly to the mucositis foci, with the lesion area divided into multiple sub-areas of 0.5 cm², each point being irradiated for 12 to 24 s in confirmed cases of OM. The control group received only oral care. In summary, PBM reduced the incidence of OM, especially during HD-MTX use. However, despite alleviating the progression of inflammation, it did not show a statistically significant difference in the frequency of severe OM or in the reduction of oral cavity recovery time.
Elkady et al. [28] evaluated 42 patients (21 from the PBM group and 21 from the control group), aged between 3 and 18 years, diagnosed with Acute Myeloid Leukemia and treated with protocols containing Cytarabine and Mitoxantrone. In the PBM group, 44 points in the oral cavity: 8 points in the right buccal mucosa, 8 in the left buccal mucosa, 4 in the upper labial mucosa, 4 in the lower labial mucosa, 6 in the dorsum of the tongue, 6 in the floor of the mouth and 4 in the soft palate with a wavelength of 660 nm, for 10 s per point. These procedures were performed on days 1, 2, 3, 4 and 5, with the assessment of OM degrees carried out on the 5th, 12th, 19th and 30th day. In the control group, oral care and simulated PBM were performed, with analyses being performed on the same days mentioned above. According to the trial, the laser group presented a lower incidence of mucositis in grades I, II and III, on the 12th and 19th day. Furthermore, PBM was considered effective, safe and viable for preventing OM in children treated with CT.
Heterogeneity in the methods used to assess outcomes among the included studies was observed. Cowen et al. [23] used a pre-established scale, as well as the Daily Mucositis Index (DMI) and Cumulative Oral Mucositis Score (COMS). Antunes et al. [24] used the WHO scale, the OMAS, and the Visual Analog Scale (VAS). Similarly, Khouri et al. [25] applied the WHO scale and the OMAS, while Ferreira et al. [26] chose the WHO to assess OM and the VAS to analyze pain. Boris et al. [27] used the WHO Oral Toxicity Index associated with the Sklansky Index to assess QOL. Finally, Elkady et al. [28] used the WHO scale together with the Common Terminology Criteria for Adverse Events (NCI-CTCAE, version 4.0) to measure OM.
In view of the above, it is observed that the red wavelength was used in all RCTs, ranging from 632.5 nm to 670 nm. Furthermore, only the study by Khouri et al. [25] associated the red and infrared wavelengths (780 nm) on alternate days. For other dosimetric parameters of PBM and number of application points/zones in the oral cavity, there was no agreement between the protocols mentioned in Table 3. Regarding the outcomes of the selected studies, PBM proved to be effective in reducing the incidence and/or frequency, in addition to preventing the progression to more severe cases of OM (Table 4).
Table 3 Laser therapy parameters of the studiesTable 4 Outcome and conclusion of studiesAssessment of risk of biasOverall, the included RCTs demonstrated a predominance of low risk of bias across most evaluated domains. Among the six studies analyzed, the studies by Cowen et al. [23], Antunes et al. [24], Ferreira et al. [26] and Elkady et al. [28] achieved low risk of bias in most domains, including the “Outcome Measurement” domain, in which the evaluators who performed the follow-up and outcome assessments were blinded to treatment allocation. This level of rigor minimized the potential for detection bias, increasing the reliability of their findings.
The studies conducted by Boris et al. [27] and Khouri et al. [25] presented a high risk of bias, especially in the Randomization process and Measurement of outcome domains. This risk stems largely from the lack of blinding in the outcome assessment, which can introduce subjective influence in the interpretation of results. Prior knowledge about the intervention received by participants can affect how measurements are recorded or interpreted, compromising the accuracy and impartiality of the findings and, consequently, the methodological robustness of the study and the reliability of the data obtained.
All studies presented some concerns about bias, specifically in the “Selection of the reported outcome” domain, likely due to the lack of a pre-specified analysis plan prior to data collection or analysis and the performance of multiple analyses/outcomes. Despite this limitation, the studies presented a low risk of bias in the “Deviations from the intended interventions” and “Missing outcome data” domains, thus strengthening the internal validity of the study and the credibility of the conclusions.
In summary, although the overall methodological quality of the included RCTs was strong, with a low risk of bias in critical areas such as randomization and data completeness, the lack of blinding in outcome assessment and selection of reported results was a limitation of some included studies. This highlights the need for future studies to further prioritize blinding procedures to increase the reliability and validity of their findings, as well as to adopt prespecified analysis plans, record all outcomes and measures transparently, and fully report all planned results, avoiding selective selection of outcomes and analyses based on the obtained findings (Fig. 2).
Fig. 2
Assessment of risk of bias based on Cochrane risk of bias tool for randomized trials (RoB 2.0)
Certainty of evidenceTable 5 summarizes the quality of the evidence. The certainty of the evidence, based on the GRADE approach, indicated moderate certainty for the prevention of OM with PBM in the included RCTs.The evidence was downgraded for imprecision, but was not inconsistent or indirectly relevant to the broad question. A large magnitude effect was also observed, which contributed to increased confidence in the findings. This means that, although there are methodological limitations and undersized samples, the studies show consistent and clinically relevant results, which can be applicable to the population, intervention and outcomes of interest in clinical practice.
Table 5 Evidence certainty assessment with grading of recommendations, assessment, development, and evaluation (GRADE)
Comments (0)