Endodontic success in AP depends on periapical tissue healing and long-term inflammation resolution in addition to microbial eradication. A successful outcome is generally characterized by presence of radiographic signs of healing and the lack of clinical signs and symptoms, and restoration of the tooth function. Clinical indicators such as pain resolution, lack of tenderness to percussion or palpation, and absence of sinus tracts are critical, while radiographic evaluation of periapical healing using tools such as CBCT-PAI adds a deeper dimension to treatment outcome analysis [21].
In the present pilot study, we showed that both NaOCl alone and adjunctive aPDT were comparable in terms of symptom relief at 24 and 48 h post treatment. However, participants who received adjunctive aPDT had a lower post-operative CBCT-PAI score at 6 months. Changes in inflammatory marker- IL-6 were found to be comparable in both the groups.
Sodium hypochlorite (NaOCl) has been the gold standard for root canal irrigation because of its superior antimicrobial activity and tissue-dissolving capacity compared with commonly used irrigants such as saline, chlorhexidine, and hydrogen peroxide [22, 23], . In this pilot study, 5.25% NaOCl was used as the irrigant but was not followed by EDTA in the final rinse to maintain a standardized irrigation protocol across both groups and to prevent possible chemical interaction with the photosensitizer prior to aPDT. Although EDTA has been shown to enhance smear layer removal and potentially improve light penetration (Wang et al., 2021) [24], its omission was intended to eliminate confounding variables and ensure protocol uniformity. The potential impact of this choice on smear layer removal and light transmission warrants further investigation in future studies. Numerous studies report success rates ranging from 74 to 86%, with up to 97% of treated teeth remaining functional post-therapy [25]. However, it has some disadvantages, such as cytotoxicity, the possibility of tissue irritation if extruded in periapical area, and the inability to totally eliminate biofilms in complex anatomical areas [7].
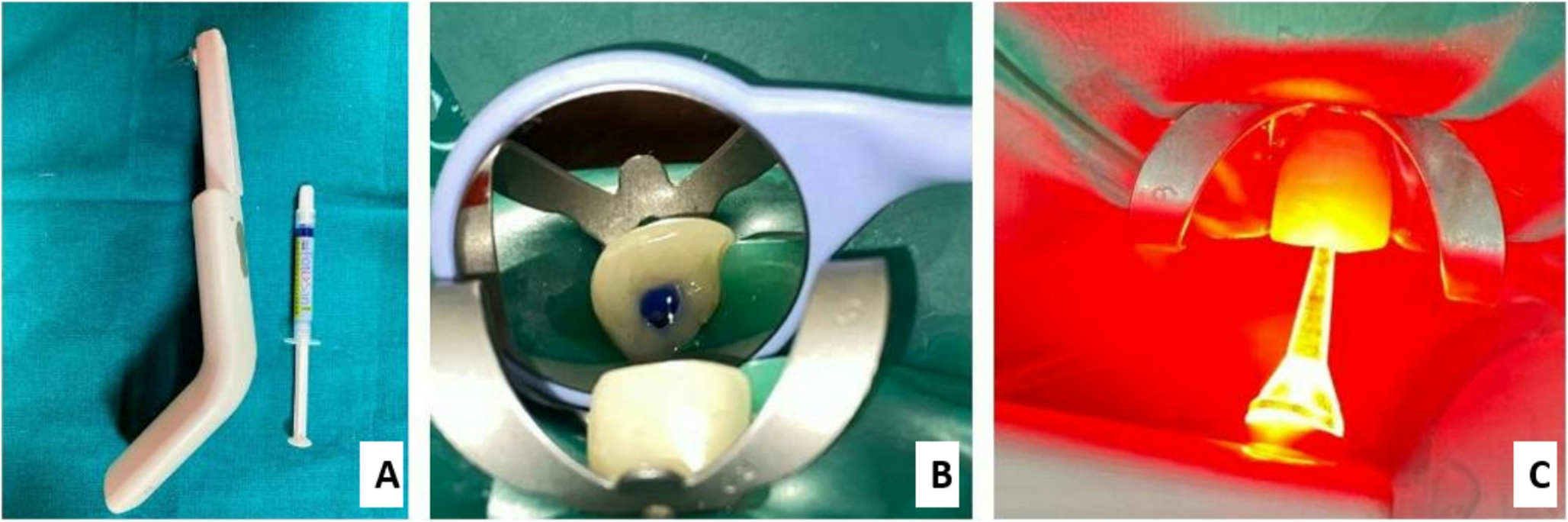
This has led to the adoption of adjunctive techniques to enhance the efficacy of NaOCl, including aPDT. The fundamental principle of aPDT involves the use of a non-toxic photosensitizer (PS) toluidine blue O (TBO). Its absorption spectrum varies with tissue binding characteristics. TBO binds in an orthochromatic state, with an absorption maximum around 630 nm, which is optimal for activation by red light (628 nm) in photodynamic therapy (Sridharan & Shankar, 2012) [26]. When it is activated by light of a specific wavelength 628 nm (630–700 nm), it produces reactive oxygen species (ROS) such as singlet oxygen and free radicals. These reactive oxygen species (ROS) generated during aPDT preferentially damage microbial cells due to their relatively simple cell wall and membrane structures and limited antioxidant defense capacity, leading to oxidative injury of proteins, lipids, and nucleic acids. In contrast, host tissues possess robust endogenous antioxidant systems that neutralize reactive species, thereby reducing collateral cytotoxicity [27, 28]. Toluidine blue has been shown to cause clinically perceptible tooth discoloration following aPDT, which can be significantly reduced by post-treatment irrigation with NaOCl (Figueiredo et al., 2014; Ozkocak et al., 2022) [29, 30]. In the present pilot study, thorough irrigation with 5.25% sodium hypochlorite followed by normal saline was performed after aPDT, and no visible discoloration was observed in any case.
Importantly, aPDT targets both planktonic bacteria and biofilms, and is effective against a broad spectrum of gram-positive and gram-negative organisms, fungi, and viruses [31]. Unlike NaOCl, aPDT does not rely on diffusion or chemical concentration gradients, making it especially effective in complex anatomical areas, including dentinal tubules, lateral canals, and apical ramifications. Studies have demonstrated its efficacy against E. faecalis, Candida albicans, and polymicrobial biofilms commonly found in persistent endodontic infections [32].
Additionally, aPDT may have immune-modulatory effects. It has been shown to reduce inflammatory cytokines such as IL-1β and TNF-α in periapical tissues, potentially facilitating faster tissue recovery and reducing postoperative symptoms. This property gives aPDT a dual role, antimicrobial and anti-inflammatory [11].
The present pilot study compared the efficacy of NaOCl and adjunctive aPDT as disinfection method in participants with primary AP in terms of inflammatory response modulation that is change in IL-6, post-operative symptom resolution, and periapical healing. Both groups exhibited significant symptomatic relief, with complete resolution in pain observed in NaOCL group similar to Farzaneh et al. (2018), which reported significantly lower post-operative pain with 5.25% NaOCL during the first 72 h after single visit root canal treatment [33], and in contrary to Rahim et al. (2024) findings which stated that higher concentration 5.25% of NaOCL was associated with more post-operative pain [34]. Prasad et al. (2024) in a systemic review and meta-analysis also showed that low concentration of NaOCL has direct relation with less post-operative pain [35], but in our present pilot study, we reported 100% resolution in post-operative pain within 48 h of root canal treatment with 5.25% NaOCl concentration. The rapid symptom relief observed in the NaOCl group can be attributed to its strong antimicrobial action and ability to dissolve organic tissues, thereby leading to early reduction in the bacterial load within the root canal system.
Adjunctive aPDT on the other hand was comparable in reducing post-operative pain. Alves et al. (2022) previously showed that aPDT was associated in reducing post-operative pain in teeth with necrotic pulp and asymptomatic periapical lesion because low-power laser is linked to the modulation of inflammation through the reduction of inflammatory cells and pain-associated substances, enhancing cellular respiration, facilitating neurotransmitter release in inflamed tissues, and decreasing the presence of inflammatory cells such as leukocytes, neutrophils, mononuclear cells, and mediators like interleukin-1 [12]. This is in contrary to Yoshinari et al. (2019) findings, which concluded that aPDT didn’t have an advantage to control post-operative pain in endodontic treatments. According to their findings, there was no difference in postoperative discomfort in both groups. Neither group experienced any postoperative pain; a selection of exclusively asymptomatic cases without pre-operative pain could be the cause of this outcome [36]. But in our pilot study, 93.3% of post-operative symptomatic relief was seen in participants after 48 h of treatment. This may be attributed to aPDT’s ability to target bacteria within biofilms and dentinal tubules while preserving the structural integrity of periapical tissues, which may contribute to its long-term effectiveness in maintaining symptom resolution.
Radiographic healing, as evaluated by CBCT-PAI, provides a quantitative and sensitive measure of periapical changes and is an important indicator for successful treatment. In our pilot study, participants treated with aPDT demonstrated better CBCT-PAI scores at 6-month intervals, both in per-protocol as well as ITT analysis. This could be attributed to preserved collagen matrix and reduced bone resorption. This aligns with preclinical studies by Trindade et al. (2017), which showed that aPDT in rats with induced AP promoted a significant decrease in inflammatory cells and improved histological outcomes [37]. While the exact mechanisms remain under investigation, it is hypothesized that ROS produced during aPDT activate latent growth factors like TGF-β1 in the surrounding tissues [38], which may aid in angiogenesis and repair. aPDT has been reported to modulate the host immune response, leading to enhanced tissue repair. Unlike sodium hypochlorite, which relies on nonspecific chemical dissolution of organic tissues, aPDT generates short-lived and spatially localized reactive oxygen species. It may be hypothesized that this localized antimicrobial action, with minimal collateral tissue effects, could contribute to the improved radiographic periapical healing observed in aPDT treated cases in the present pilot study; however, this warrants further investigation in future studies.
Endodontic infections trigger an immune response characterized by the release of pro-inflammatory cytokines, including IL-6, which plays a pivotal role in mediating inflammation, bone resorption, and periapical lesion progression. Azuma et al. (2014) concluded that IL-6 acts as pro-inflammatory marker leading to bone resorption in AP [5]. However, the change in IL-6 levels was comparable in both the groups in our RCT. This suggests that the host immune response to endodontic disinfection is multifaceted and may depend on factors such as microbial composition, individual immune status, and the extent of periapical involvement at baseline. The findings of this pilot study indicate that while both treatment modalities contribute to inflammatory modulation, neither approach demonstrated a statistically significant advantage over the other in altering IL-6 trends. This aligns with previous studies suggesting that while mechanical and chemical disinfection can reduce bacterial loads, complete eradication of endotoxins and inflammatory mediators remains challenging [39].
According to Freitas and Hamblin., (2016) [40] such light-based mechanisms can positively influence wound healing and inflammation control. These effects may have played a complementary role in the healing outcomes observed in the present pilot study.
Our pilot study had several strengths. It was a randomized controlled study which made the groups comparable with respect to their baseline characteristics. We used allocation concealment to avoid any bias. Our pilot study is novel in the regard that no studies have previously evaluated the role of adjunctive aPDT in periapical healing and immune modulation, in treatment of AP.
However, our pilot study had few limitations as well. We did not formally evaluate the cost-effectiveness of aPDT in therapy selection. aPDT necessitates the purchase of laser equipment and photosensitizers, however, long-term costs are offset by aPDT’s ability to eliminate the need for unplanned visits and retreatments, despite its higher initial costs. Participant blinding was not feasible due to visible light cues. However, the primary outcome i.e. IL-6 levels, and radiographic healing were objective measures that are not influenced by patient perception, and pain scores showed no significant intergroup difference. Additionally, IL-6 levels were evaluated at a 6-month interval to coincide with the radiographic healing assessment and to represent sustained inflammatory resolution rather than immediate post-disinfection changes. While this provides insight into long-term modulation, we acknowledge that IL-6 may exhibit early transient fluctuations following disinfection. Future studies with serial sampling at multiple time points (e.g., baseline, 24 h, 7 days, and 6 months), combined with microbial quantification, would more comprehensively delineate both the immediate and prolonged biological effects of adjunctive aPDT. As this was a pilot randomized controlled study, the sample size was determined using the closest available reference in the literature [19] and included 17 participants in each arm. However, the possibility of getting a type II error cannot be excluded in terms of the effects of aPDT on IL-6 modulation. Hence, further studies with larger sample size would be desirable to further evaluate the role of aPDT on IL-6 modulation. Additionally, a longer follow-up period could have provided a better assessment of long-term radiographic healing outcomes.
To summarize, adjunctive aPDT and NaOCl alone were comparable in managing primary AP with respect to improvements in symptoms and IL-6 levels. However, when periapical healing was assessed radiographically using CBCT-PAI scores, the aPDT group demonstrated superior results. While aPDT cannot be considered a replacement for NaOCl based on these findings, it may serve as a useful adjunct, particularly in cases where reduced NaOCl concentration or exposure is desired due to hypersensitivity or cytotoxicity concerns.

Comments (0)